Tympanoplasty
Reading File
Finding Sources
Searching PubMed
tympanoplasty outcomes techniques
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Here is a comprehensive overview of tympanoplasty based on authoritative otolaryngology textbooks (Cummings Otolaryngology and Shambaugh Surgery of the Ear):
Tympanoplasty
Definition and Goals
Tympanoplasty is a surgical procedure performed to:
- Eradicate middle ear infection/pathology
- Restore middle ear function - specifically the middle ear transformer mechanism
- Repair the tympanic membrane (TM)
- Reconstruct the ossicular chain (ossiculoplasty) when needed
The Wullstein classification (introduced historically) categorizes tympanoplasty based on (1) remaining middle ear structures after eradication of pathology and (2) how sound is transferred to the oval window while protecting the round window.
Middle Ear Mechanics - Functional Basis
Understanding why tympanoplasty works requires understanding middle ear sound transmission:
- Ossicular coupling: Sound pressure gain through TM and ossicular chain. Mean middle ear gain is ~20 dB at 250-500 Hz, peaks ~25 dB at 1 kHz, then decreases ~6 dB/octave above 1 kHz.
- Acoustic coupling: Direct sound pressure difference between oval and round windows. Normally negligible but becomes significant in diseased/reconstructed ears.
- TM perforation effect: Reduces the sound pressure difference across TM, causing frequency-dependent hearing loss proportional to perforation size. Hearing loss does NOT vary significantly with perforation location.
- Middle ear aeration: A minimum of ~0.5 mL of middle ear air is required to maintain ossicular coupling within 10 dB of normal.
Preoperative Evaluation
- Detailed history: infections, drainage, prior surgery, PE tube placement
- Otomicroscopic examination: perforation type (central vs. marginal), extent, TM remnant health, myringosclerosis, atrophic areas
- Central perforation: surrounded circumferentially by residual TM
- Marginal perforation: no TM remnant between part of the perforation and bony canal wall
- Perforations >50% of the membrane have lower success rates
- Eustachian tube function assessment (no current test reliably predicts postoperative function when perforation is present)
- Complete audiometry + tuning fork tests
- Radiographic evaluation usually not needed for dry central perforations
Surgical Approaches
Three main approaches are used, selected based on perforation size, canal anatomy, and surgeon preference:
| Approach | Indications | Notes |
|---|---|---|
| Transcanal | Small-to-medium posterior perforations, large canal | Avoids mastoid dressing; less morbidity (less pain, hematoma, infection risk) |
| Endaural | All perforation sizes; limited atticotomy planned | More common in Europe; self-retaining retractor available |
| Postauricular | Large perforations, small canals, anterior perforations | Most common in the US; best anterior visualization; allows bimanual technique |
The postauricular approach is most commonly used in the United States.
Graft Techniques
Medial (Underlay) Technique
- Graft placed medial to the TM remnant and manubrium of malleus
- Easier to master; high success rates
- Most common technique today
- Advantages: avoids blunting of the anterior sulcus, no epithelial pearl formation
Lateral (Overlay) Technique
- Graft placed lateral to the malleus handle
- Better for total perforations and when cholesteatoma lines the TM remnant (allows excision of remnant)
- Complications: anterior sulcus blunting (~10-15%), epithelial pearl formation, graft lateralization
- Requires meticulous removal of all squamous epithelium
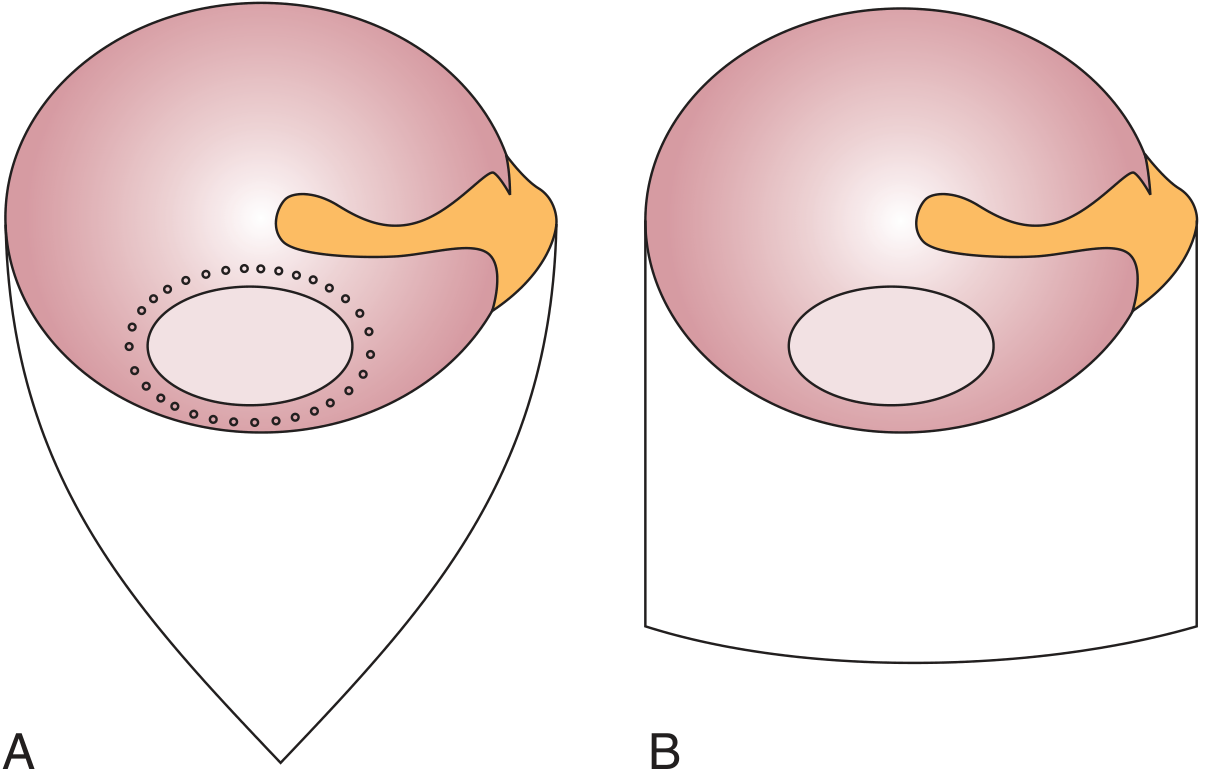
Fig. 142.1 (A) Triangular tympanomeatal flap with perforation edge prepared for excision (dotted outline). (B) Rectangular tympanomeatal flap. - Cummings Otolaryngology
Graft Materials
Temporalis Fascia (TF)
- Most widely used; high success rates (88-97% graft take)
- Harvested from the temporalis muscle fascia via postauricular or endaural approach
Perichondrium
- Harvested from tragus or concha
- Good results; often used with cartilage as composite graft
Cartilage Grafts
Increasingly used, especially in challenging situations:
- Eustachian tube dysfunction (ongoing or anticipated)
- Revision surgery
- Perforation >50%
- Ear draining at time of surgery
- Atelectatic ear / retraction pockets
- Reconstruction after cholesteatoma
- Bilateral perforations
Cartilage types:
- Palisade technique: strips of cartilage arranged side-by-side
- Composite cartilage/perichondrium island graft: eccentrically placed cartilage disk attached to perichondrial flap
- Butterfly/inlay technique: for small-to-medium perforations without elevating a tympanomeatal flap; scored circumferentially 2 mm and nestled between freshened perforation edges
Source: tragal cartilage (thicker, flatter, better for larger perforations) or conchal cartilage
Fat Graft
- For small persistent perforations (e.g., after PE tube extrusion), failed myringoplasty
- Can be done under local anesthesia as office/ambulatory procedure
- Earlobe fat harvested via small incision, inserted in dumbbell fashion
Ossiculoplasty (Ossicular Chain Reconstruction)
Indicated when the ossicular chain is disrupted or fixed.
Common Causes of Ossicular Problems
- Erosion by cholesteatoma (most commonly the lenticular process or long process of incus)
- Trauma (longitudinal temporal bone fractures - incus dislocation most common)
- Chronic infection with ossicular necrosis
Audiometric Patterns
- Ossicular discontinuity: near-maximal (~55-60 dB) conductive loss across all frequencies; deep tympanometric pattern (type Ad)
- Ossicular fixation: low-frequency predominant conductive loss; flat tympanogram; Carhart notch (5-10-15-5 dB dip at 500-1000-2000-4000 Hz in bone conduction)
- Partial incudostapedial separation (fibrous union): air-bone gap greater in high frequencies
Prosthesis Types
| Type | Description | Use |
|---|---|---|
| PORP (Partial Ossicular Replacement Prosthesis) | Connects TM/malleus to intact stapes head | Stapes arch intact |
| TORP (Total Ossicular Replacement Prosthesis) | Connects TM/malleus to stapes footplate | Stapes arch absent |
Materials
- Autografts: Reshaped incus or cortical bone/cartilage (biocompatible, low extrusion, no cost, but time-consuming to shape; concerns about cholesteatoma recurrence)
- Allografts (synthetic prostheses): Titanium, hydroxyapatite, plastipore/TORP/PORP. Trend has shifted toward allografts over autografts.
- Cartilage placed between TM and prosthesis reduces extrusion risk
Anesthesia
- General anesthesia: preferred in children and anxious adults
- Local anesthesia: feasible for adults; ear canal injected with 1% lidocaine + epinephrine 1:100,000 for vasoconstriction
- Povidone-iodine (Betadine) prep should not enter the middle ear
Postoperative Care
- Discharged same day (next day if nausea/vomiting)
- Mastoid dressing and drain removed next day
- Antibiotic ear drops at bedtime
- Water precautions; cotton ball with petroleum ointment when showering
- No nose blowing until TM healed; open mouth if sneezing
- First visit: 1 week (remove Merocel/Pope's ear wick)
- Second visit: 3-4 weeks (suction remaining Gelfoam; cauterize granulations with 25% silver nitrate)
- Hearing improvement noted within 6-8 weeks
- Audiogram at 4-6 months postoperatively
Outcomes
Graft take rates are generally excellent:
| Author | N | Technique | Graft | Take (%) |
|---|---|---|---|---|
| Vartiainen | 404 | Overlay + underlay | Temporalis fascia | 88% |
| Sheehy | 472 | Overlay | Temporalis fascia | 97% |
| Glasscock | 1,556 | Underlay | Autogenous/homograft TF | 93% |
| Cueva | 406 | Underlay | Areolar tissue | 97.5% |
Overall graft-take success rate: >90%
Experienced surgeons should close TM perforations in approximately 90% of cases regardless of graft technique.
Negative Prognostic Factors
- Eustachian tube dysfunction
- Presence of cholesteatoma or atelectasis
- Previous tympanoplasty failure
- Lateralized tympanic membrane
- Smoking
- Drainage at time of surgery
- Perforation >50% of TM
Complications and Failure Modes
Causes of Tympanoplasty Failure
- Persistent/recurrent perforation
- Blunting of the anterior sulcus (associated with overlay technique; requires meticulous technique to prevent)
- Graft lateralization (graft migrates away from manubrium; can occur if placed lateral to manubrium at primary surgery)
- Epithelial pearl formation (keratin accumulation; associated with overlay technique; meticulous epithelium removal at primary surgery is preventive)
- Conductive hearing loss
Contributing Factors
- Poor Eustachian tube function
- Inadequate visualization of anterior sulcus
- Extensive tympanosclerosis of TM remnant
- Inadequate Gelfoam support anteriorly
- Recurrent/residual cholesteatoma
Cholesteatoma After Tympanoplasty
- Recurrent cholesteatoma: ~14% after intact canal wall (ICW) mastoidectomy
- Residual cholesteatoma: ~12% after ICW mastoidectomy
- Higher in children (25% vs 11.7% in adults)
- Requires "second look" procedure at 12 months after ICW mastoidectomy
Revision Tympanoplasty
- Slightly less successful than primary cases but still satisfactory
- Cartilage "shield" technique for revision: graft-take ~93.5%, majority achieve air-bone gap <25 dB
Special Situations
Pediatric Tympanoplasty
- Generally deferred until age 7-8 (Eustachian tube more mature)
- Higher failure rates than adults due to ongoing ET dysfunction and otitis media
- Cartilage grafts preferred
Atelectatic Ear
- End-stage Eustachian tube dysfunction
- Management controversial (observe vs. cartilage tympanoplasty)
- Risk: converting a dry, asymptomatic ear into one requiring ongoing care
Secondary Acquired Cholesteatoma
- Keratinized epidermis migrates into middle ear through perforation
- Suspect when: no retraction/adhesion; smooth epidermal transition around perforation margins; opaque TM adjacent to perforation
- Lateral technique preferred to allow complete excision of cholesteatoma-lined remnant
Recent Evidence (2024-2026)
- A 2024 meta-analysis (PMID 38415937) comparing endoscopic vs. microscopic tympanoplasty found endoscopic approaches offer comparable outcomes with less invasiveness.
- A 2025 systematic review (PMID 39786316) on endoscopic vs. microscopic ossicular chain reconstruction showed similar functional hearing outcomes between approaches.
- A 2024 meta-analysis (PMID 39113516) evaluated tympanic cavity packing in Type 1 tympanoplasty.
Sources: Cummings Otolaryngology Head and Neck Surgery, Chapter 142; Shambaugh Surgery of the Ear, Chapters 20 & 28; Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2
This is a shared conversation. Sign in to Orris to start your own chat.