Show me the complete screening algorithm and management plan for rhesus negative mothers from booking visit
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the complete screening algorithm and management plan.
Rh-Negative Mothers: Complete Screening Algorithm & Management Plan
Background: Why This Matters
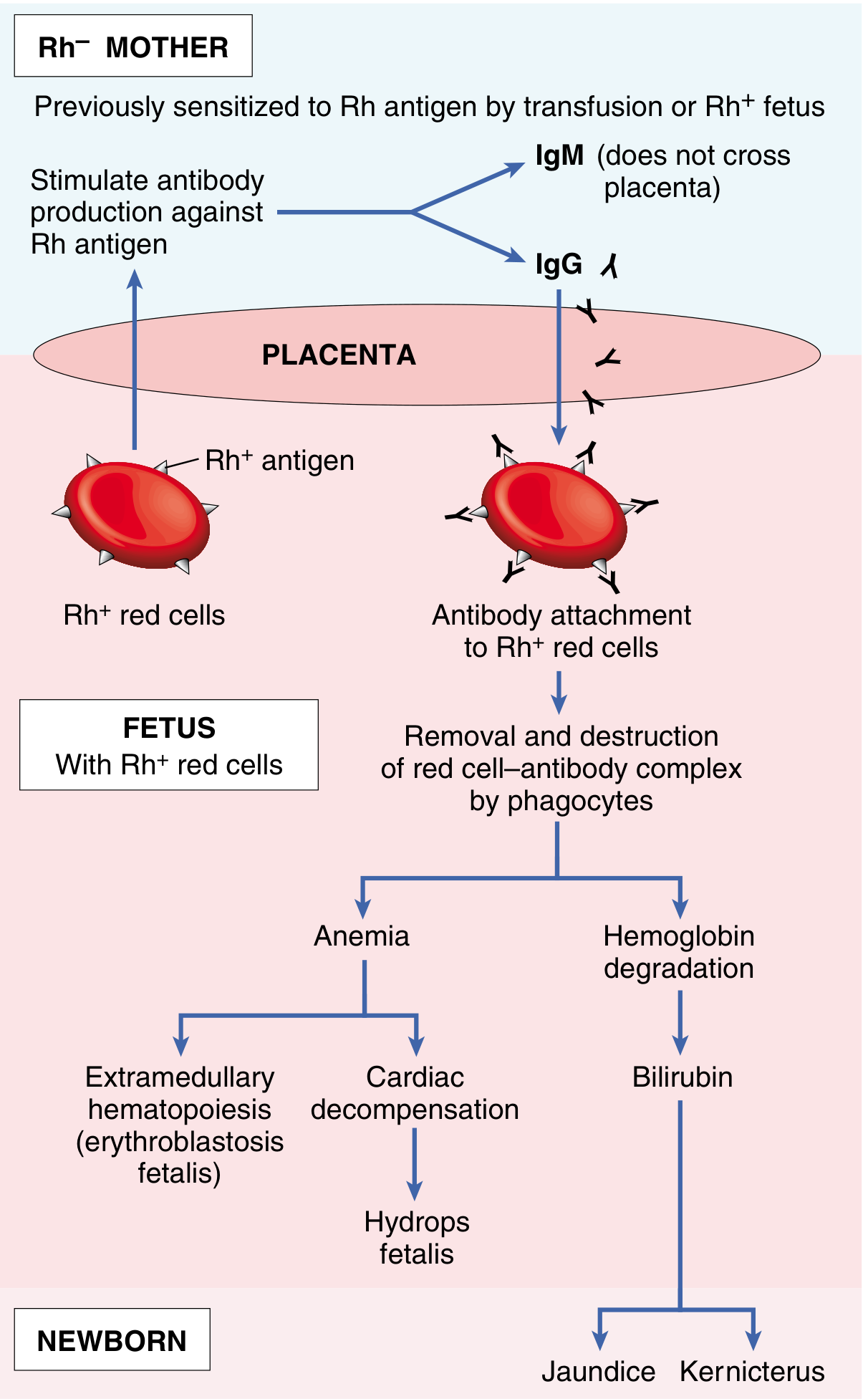
The D antigen of the Rh blood group system is the primary cause of Rh incompatibility. An Rh-negative mother carrying an Rh-positive fetus can have fetal red cells cross the placenta into her circulation, triggering maternal IgG anti-D antibody formation. In subsequent pregnancies, these antibodies cross the placenta and destroy fetal red cells, causing hemolytic disease of the fetus and newborn (HDFN) — manifesting as erythroblastosis fetalis, hydrops fetalis, jaundice, and kernicterus.
First pregnancies are usually safe because the primary immune response generates IgM (which cannot cross the placenta). The danger escalates with subsequent pregnancies: ~3% of 2nd babies are affected, ~10% of 3rd babies, and rising thereafter. — Guyton and Hall Textbook of Medical Physiology
Screening Algorithm from Booking Visit
STEP 1 — Booking Visit (First Antenatal Visit, ~8–12 weeks)
| Action | Detail |
|---|---|
| Blood group & Rh typing | ABO and RhD status must be determined for ALL pregnant women |
| Indirect Coombs Test (ICT) / Antibody Screen | Test for pre-existing anti-D (or other) antibodies in maternal serum |
| Partner blood grouping | Determine if father is Rh-positive (if Rh-negative father → fetus must be Rh-negative → no risk) |
Interpret the antibody screen:
- Antibody screen NEGATIVE + Rh-negative → Unsensitized → proceed with prophylaxis protocol below
- Antibody screen POSITIVE (anti-D detected) → Already sensitized → escalate to alloimmunized pregnancy management
STEP 2 — Antenatal Monitoring (Unsensitized Rh-Negative)
| Timing | Action |
|---|---|
| ~20 weeks | Repeat ICT/antibody screen |
| 28 weeks | Repeat ICT — if still negative, administer routine antenatal anti-D prophylaxis |
| 34–36 weeks | Repeat antibody screen before second dose (where two-dose regimen used) |
STEP 3 — Routine Antenatal Anti-D Prophylaxis (RAADP)
Who: All unsensitized (antibody screen negative) Rh-D-negative pregnant women
Dose & Timing:
- Standard regimen: Anti-D immunoglobulin 300 mcg IM at 28 weeks (single-dose protocol — ACOG-endorsed)
- Alternative two-dose: 100–125 mcg at 28 weeks AND 34 weeks
The anti-D antibody is given antepartum at 28–30 weeks of gestation. The mechanism involves clearing Rh-positive fetal cells from maternal circulation before B-lymphocyte sensitization can occur — thereby preventing formation of memory B cells that would activate in future pregnancies. — Guyton and Hall Textbook of Medical Physiology
Rh(D) immune globulin (300 mcg IM) is a concentrated solution of human IgG with high-titer anti-Rh(D) antibodies. For this prophylaxis to succeed, the mother must be Rh-D-negative and not already immunized. — Katzung's Basic and Clinical Pharmacology, 16th Edition
STEP 4 — Sensitizing Events Requiring Additional Anti-D Doses
Anti-D must be given within 72 hours of any potential fetomaternal hemorrhage (FMH), regardless of gestational age:
| Sensitizing Event | Anti-D Dose |
|---|---|
| Miscarriage / threatened miscarriage | 50 mcg if <12 weeks; 300 mcg if ≥12 weeks |
| Ectopic pregnancy | 50 mcg (<12 weeks); 300 mcg acceptable |
| Chorionic villus sampling (CVS) | 300 mcg |
| Amniocentesis | 300 mcg |
| External cephalic version (ECV) | 300 mcg |
| Antepartum hemorrhage (APH) | 300 mcg; repeat if continued bleeding |
| Abdominal trauma | 300 mcg — "If as little as 0.1 μL of Rh-positive fetal blood enters an Rh-negative mother's circulation, the mother can develop Rh antibodies" — Tintinalli's Emergency Medicine |
| Intrauterine procedures | 300 mcg |
| Delivery of Rh-positive baby | 300 mcg within 72 hours of delivery |
ACOG and ACEP both recommend 50 mcg for procedures/events before 12 weeks (due to small fetoplacental blood volume ~4.2 mL at 12 weeks); 300 mcg for events at ≥12 weeks. — Tintinalli's Emergency Medicine
Kleihauer-Betke (KB) test / Flow cytometry: Performed when large FMH is suspected (e.g., trauma, significant APH, abruption after 12 weeks). Quantifies fetal cells in maternal blood — additional anti-D vials are given if FMH exceeds the coverage of 300 mcg (~30 mL fetal whole blood).
STEP 5 — Postnatal Management
| Neonatal result | Action |
|---|---|
| Baby Rh-positive, mother still unsensitized | Give anti-D 300 mcg IM within 72 hours of delivery |
| Baby Rh-negative | No anti-D required |
| Large FMH on KB test | Additional anti-D doses proportional to estimated hemorrhage |
Management of the Sensitized (Alloimmunized) Rh-Negative Mother
When anti-D antibodies are already present at booking or develop during pregnancy, prophylaxis is futile and management shifts to fetal surveillance:
Monitoring Protocol for Alloimmunized Pregnancy
| Anti-D Titer | Management |
|---|---|
| Low titre (<1:4–1:8) | Serial antibody titres every 4 weeks; fetal surveillance with growth scans |
| Rising titre (≥1:16 or critical titre) | Doppler assessment of fetal middle cerebral artery peak systolic velocity (MCA-PSV) every 1–2 weeks |
| MCA-PSV >1.5 MoM | Strongly predictive of fetal anemia → proceed to fetal blood sampling (FBS) |
Fetal Blood Sampling (FBS) & Intrauterine Transfusion (IUT)
- FBS via cordocentesis (umbilical vein) confirms fetal hemoglobin
- If fetal Hb <2 SD below mean for gestational age → Intrauterine intravascular transfusion (IVT) with O-negative, CMV-negative, irradiated, leukodepleted blood
- May be repeated every 2–4 weeks until fetus is mature enough for delivery
Delivery Timing
- Unaffected or mildly affected fetuses: Deliver at 37–38 weeks
- Severely affected or post-IUT: Deliver at 34–37 weeks depending on fetal condition
- Post-delivery: neonatal exchange transfusion and/or phototherapy for jaundice/hyperbilirubinemia; monitor for kernicterus
Antenatal identification and management of the at-risk fetus have been greatly facilitated by amniocentesis and chorionic villus and fetal blood sampling. Severe intrauterine hemolysis may be treated by fetal intravascular transfusions via the umbilical cord and early delivery. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Complete Algorithm Summary
BOOKING VISIT
│
▼
Blood group + Rh typing + ICT (antibody screen)
│
├─── Rh POSITIVE ──────────────────► Standard antenatal care
│
└─── Rh NEGATIVE
│
├─── ICT POSITIVE (anti-D present)
│ │
│ └─► ALLOIMMUNIZED pathway:
│ • Serial titres q4 weeks
│ • MCA-PSV Doppler if titre ≥ critical level
│ • FBS + IUT if MCA-PSV >1.5 MoM
│ • Planned delivery 34–38 wks
│
└─── ICT NEGATIVE (unsensitized)
│
▼
Check partner Rh type
│
├─ Partner Rh-NEGATIVE → Fetus must be Rh-negative
│ → No anti-D needed; routine care
│
└─ Partner Rh-POSITIVE or unknown
│
▼
PROPHYLAXIS PROTOCOL:
• Repeat ICT at 20 wks
• Anti-D 300 mcg IM at 28 wks (± 34 wks)
• Anti-D at ANY sensitizing event within 72 hrs
• Post-delivery: check baby's Rh type
│
├─ Baby Rh-POSITIVE → Anti-D 300 mcg within 72 hrs
│ ± KB test if large FMH suspected
└─ Baby Rh-NEGATIVE → No anti-D needed
Key Points to Remember
| Point | Detail |
|---|---|
| Window for anti-D | Must be given within 72 hours of sensitizing event (ideally within 24 hrs) |
| First pregnancy risk | Usually safe — initial IgM response doesn't cross placenta; danger is in subsequent pregnancies |
| ABO protection | Concurrent ABO incompatibility partially protects the mother (fetal cells cleared by anti-A/B IgM before sensitization occurs) |
| Rh-negative = homozygous deletion | Rh-negative individuals lack the RHD gene entirely — so no "d" antibody exists |
| Weak D / partial D | Some women type as Rh-positive but have partial D antigens — may still be at risk; management is institution-specific |
| Non-D antigens | Anti-Kell (K), anti-c, anti-E can also cause HDFN — detected by ICT; managed similarly to anti-D alloimmunization |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease — Immune Hydrops / Etiology & Pathogenesis
- Guyton and Hall Textbook of Medical Physiology — Erythroblastosis Fetalis & Prevention
- Katzung's Basic and Clinical Pharmacology, 16th Edition — Rh(D) Immune Globulin
- Tintinalli's Emergency Medicine — Rh Seroconversion & Anti-D Indications
- Emery's Elements of Medical Genetics and Genomics — Rhesus Hemolytic Disease of the Newborn
What is the algorithm of investigation approach for a mother coming with a low SFH for period of gestational age
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a comprehensive, algorithm-based answer. Let me compile it.
Investigation Algorithm for Low Symphysis-Fundal Height (SFH) for Period of Gestation
What Does Low SFH Mean?
SFH (in cm) between 24–36 weeks normally approximates gestational age in weeks (±2 cm). A measurement ≥3–4 cm less than expected for gestational age is the standard trigger for further investigation, raising suspicion of Fetal Growth Restriction (FGR) — a fetus that has not achieved its growth potential.
"Measurement of the symphysis-fundal height is helpful in screening for abnormal fetal growth... but [is] not sensitive enough for accurate detection of most infants with growth restriction." Clinical diagnosis of FGR by physical examination alone is missed almost half the time. — Creasy & Resnik's Maternal-Fetal Medicine
Clinical signs of IUGR include poor increase in fundal height (>4 cm difference from expected) or inadequate maternal weight gain (<100–200 g/week in the third trimester). Diagnosis by clinical means alone is possible in only ~33% of pregnancies. — Pfenninger and Fowler's Procedures for Primary Care
Step 1 — Clinical Assessment at the Visit
Before ordering investigations, take a targeted history and examination to identify the cause of the small fundus.
Confirm Dates First
| Question | Significance |
|---|---|
| Last menstrual period (LMP) — reliable? | Inaccurate dates are the most common explanation for apparent low SFH |
| First-trimester ultrasound (CRL)? | Crown-rump length before 14 weeks is the most accurate dating method (±5–7 days) |
| Any previous growth scans as baseline? | Serial measurements by the same observer are more meaningful than single readings |
If LMP is unreliable and no first-trimester dating scan was done, any "low SFH" may simply reflect miscalculation of gestational age — this must be excluded before labelling as FGR.
Exclude Non-Pathological Causes
| Cause | Feature |
|---|---|
| Inaccurate dates | No reliable LMP; no early USS |
| Maternal body habitus (obesity) | SFH notoriously inaccurate in obese patients |
| Fetal lie (transverse/oblique) | Fundus appears low; on palpation — no pole in pelvis |
| Engaged head (late 3rd trimester) | Head descends into pelvis → apparent fall in SFH |
| Empty bladder (slight) | Minimal impact but worth standardising technique |
Maternal History for Risk Factors of FGR
Maternal factors:
- Hypertension (chronic or gestational / pre-eclampsia)
- Diabetes with vasculopathy
- Chronic renal insufficiency
- Antiphospholipid syndrome / SLE
- Smoking, alcohol, cocaine/heroin use
- Severe malnutrition / poor weight gain
- Prescribed medications (beta-blockers, steroids)
- Pregnancy at high altitude
Fetal/placental factors:
- Multiple gestation
- Chromosomal/structural abnormalities
- Congenital infections (rubella, CMV, toxoplasma)
- Placental insufficiency / abnormalities
— Creasy & Resnik's Maternal-Fetal Medicine, Box 44.2
Step 2 — First-Line Investigation: Ultrasound
Ultrasound is the single most important investigation. It should be arranged promptly (same-day or within 48 hours depending on urgency).
Biometry — confirm FGR and determine type
| Parameter | Role | Notes |
|---|---|---|
| Abdominal Circumference (AC) | Best single predictor of FGR — reflects liver glycogen stores / nutritional status | Suspect FGR if AC <15th percentile; >95% sensitivity if AC <2.5th percentile |
| Estimated Fetal Weight (EFW) | Combines AC, HC, BPD, FL | FGR = EFW or AC <10th percentile (ACOG); more clinically significant <5th or 3rd percentile |
| Head Circumference (HC) | More shape-independent than BPD | Spared in asymmetric FGR early on |
| Biparietal Diameter (BPD) | Less useful alone | Falls late in asymmetric FGR; reduced proportionately in symmetric FGR |
| Femur Length (FL) | Often parallels GA in asymmetric FGR | Most useful in ratios |
| HC/AC ratio | Distinguishes symmetric from asymmetric | HC/AC ≥0.95; HC/AC >1.0 after 36 wks detects 85% of IUGR |
| FL/AC ratio | ≥23.5% suggests IUGR |
Classify FGR Type
| Type | Description | Cause |
|---|---|---|
| Asymmetric FGR (~80%) | AC/body small; head spared (brain-sparing) | Uteroplacental insufficiency — late onset; hypoxia redistributes blood to brain |
| Symmetric FGR (~20%) | All measurements proportionately reduced | Early insult — chromosomal, infection, structural; all organs equally affected |
Symmetric FGR requires serial scans at 2–3 week intervals if gestational age is uncertain. — Pfenninger and Fowler's Procedures for Primary Care
Amniotic Fluid Volume
| Finding | Significance |
|---|---|
| Oligohydramnios (AFI <5 cm / single deepest pool <2 cm) | Reflects decreased fetal renal perfusion from hypoxia; combined with FGR = high-risk outcome; sensitivity >85% in high-risk populations |
| Normal fluid | Does not exclude FGR |
If oligohydramnios is present with no PROM and no anomalies, FGR is the likely cause. Combination of oligohydramnios + FGR portends a less favourable outcome; delivery at ≥36 weeks generally indicated. — Pfenninger and Fowler's Procedures for Primary Care
Placental Assessment
| Finding | Significance |
|---|---|
| Premature grade III placenta (before 35 weeks) | Further evidence of uteroplacental insufficiency and FGR |
| Placental mosaicism, infarcts, haematomas | May be primary cause of FGR |
Step 3 — Doppler Velocimetry
Once FGR is confirmed on biometry, Doppler studies are essential to assess fetoplacental blood flow and fetal cardiovascular compensation.
Sequence of Doppler Deterioration in FGR
| Stage | Doppler Finding | Clinical Significance |
|---|---|---|
| Stage 1 | ↑ Umbilical artery (UA) PI / S:D ratio | Increased placental resistance; early compromise |
| Stage 2 | Absent end-diastolic flow (AEDF) in UA | Severe placental insufficiency |
| Stage 3 | Reversed end-diastolic flow (REDF) in UA | Critical — imminent fetal compromise |
| Redistribution | ↓ MCA PI ("brain-sparing") — MCA/UA ratio (CPR) <1.0 | Fetus redistributing blood to brain; brain-sparing response |
| Late/severe | Absent/reversed a-wave in Ductus Venosus (DV) | Cardiac decompensation; pre-terminal |
| Late/severe | Pulsations in umbilical vein (UV) | Severe cardiac compromise; imminent death |
Step 4 — Fetal Well-being Assessment
Run concurrently with Doppler once FGR is confirmed:
Biophysical Profile (BPP)
| Parameter (1 point each) | Normal = 2; Abnormal = 0 |
|---|---|
| Fetal breathing movements (≥1 episode ≥30 sec in 30 min) | |
| Gross body movements (≥3 discrete movements) | |
| Fetal tone (≥1 active extension + return to flexion) | |
| Amniotic fluid volume (AFI ≥5 or deepest pool ≥2 cm) | |
| Non-stress test (NST) (reactive = 2 accelerations in 20 min) |
| Score | Interpretation |
|---|---|
| 8–10/10 | Normal — reassuring |
| 6/10 | Equivocal — repeat in 24 hrs or deliver if ≥36 wks |
| ≤4/10 | Abnormal — deliver regardless of gestational age |
AFV assessment appears to have value as an indicator of fetal outcome. Severe oligohydramnios is associated with a high risk of fetal compromise. In early-onset FGR, AFI <5 cm was present in 89% of pregnancies. — Creasy & Resnik's Maternal-Fetal Medicine
Non-Stress Test (NST) / Cardiotocography (CTG)
- Reactive NST: two accelerations of ≥15 bpm × ≥15 sec in 20 minutes
- Loss of variability and decelerations are ominous in FGR
Step 5 — Targeted Investigations for Underlying Cause
Once FGR is confirmed, investigate the cause to guide management:
Maternal Investigations
| Investigation | Indication / Purpose |
|---|---|
| Full blood count | Anaemia, thrombocytopenia (pre-eclampsia, HELLP) |
| Urine dipstick / PCR | Proteinuria → pre-eclampsia |
| BP measurements | Hypertensive disorders |
| TORCH serology (if not done) | Rubella, CMV, toxoplasma, HSV — all associated with symmetric FGR |
| Antiphospholipid antibodies (lupus anticoagulant, anti-cardiolipin, anti-β2-GPI) | Antiphospholipid syndrome — common cause of placental-mediated FGR |
| Renal function tests | Chronic kidney disease |
| Uterine artery Doppler | High RI/notching → uteroplacental insufficiency; useful early predictor |
| Thyroid function | Hypothyroidism → FGR |
| Random blood glucose / HbA1c | Diabetes with vasculopathy |
| Drug screen (urine) | Cocaine, heroin use |
Fetal Investigations
| Investigation | Indication |
|---|---|
| Detailed anomaly scan | FGR + structural defects → karyotype indicated |
| Fetal karyotype (amniocentesis or CVS) | FGR diagnosed in 2nd trimester with structural defect; trisomy 13/18/21 all cause FGR |
| Chromosomal microarray | Standard karyotype + microarray detects 18.8% abnormalities vs 9.3% with karyotype alone in FGR |
| Viral PCR (amniotic fluid) | If CMV/rubella suspected clinically |
| Fetal blood sampling (cordocentesis) | Severe FGR — assess pH, PO₂, haematocrit; confirms acidaemia |
In FGR diagnosed in the second trimester with a structural defect, karyotype is recommended. Microarray provides a 4% incremental yield for pathogenic copy number variants in isolated FGR with normal karyotype. — Creasy & Resnik's Maternal-Fetal Medicine
Full Investigation Algorithm (Flow Chart)
LOW SFH (≥3–4 cm below expected for GA)
│
▼
STEP 1: CONFIRM DATES
Reliable LMP + first-trimester CRL?
│
├─── NO/UNCERTAIN ──► Revise EDD using USS biometry
│ If dates change → reassess SFH discrepancy
│
└─── YES → Proceed
│
▼
STEP 2: EXCLUDE CLINICAL CAUSES
- Fetal lie (transverse/oblique)?
- Engaged head (term)?
- Maternal obesity (SFH unreliable)?
│
▼
STEP 3: ULTRASOUND (urgent)
┌─────────────────────────────────────┐
│ Biometry: AC, EFW, HC, BPD, FL │
│ Ratios: HC/AC, FL/AC │
│ Amniotic fluid: AFI / deepest pool │
│ Placental appearance/grading │
│ Fetal anatomy survey │
└─────────────────────────────────────┘
│
┌─────────┴────────────┐
│ │
EFW/AC ≥10th EFW/AC <10th percentile
percentile (FGR confirmed)
│ │
Repeat scan CLASSIFY:
in 2–4 weeks ┌───────────────────────┐
│ │ Asymmetric (AC small, │
│ │ HC spared) vs │
│ │ Symmetric (all small) │
│ └───────────────────────┘
│ │
│ ▼
│ STEP 4: DOPPLER STUDIES
│ ┌──────────────────────────────────┐
│ │ Umbilical artery (UA) PI/S:D │
│ │ Middle cerebral artery (MCA) PI │
│ │ Cerebroplacental ratio (CPR) │
│ │ (± DV, UV if UA absent/reversed) │
│ └──────────────────────────────────┘
│ │
│ ┌──────────┴──────────────────┐
│ Normal Doppler Abnormal Doppler
│ │ │
│ NST/BPP weekly NST/BPP TWICE WEEKLY
│ Deliver at 39 wks + serial Doppler
│ │
│ ┌──────────┴──────────┐
│ UA AEDF UA REDF
│ │ │
│ Deliver ≥33 wks DELIVER
│ NST/BPP guides (hospitalize
│ if <33 wks if <30 wks;
│ daily testing)
│
└──────► STEP 5: INVESTIGATE CAUSE
┌───────────────────────────────────┐
│ Maternal: BP, urine, FBC, LFTs │
│ TORCH serology, aPL antibodies │
│ Renal/thyroid/glucose │
│ Uterine artery Doppler │
│ │
│ Fetal: Detailed anomaly scan │
│ Karyotype + microarray if anomaly │
│ Viral PCR if infection suspected │
└───────────────────────────────────┘
Delivery Timing Summary
| Situation | Timing |
|---|---|
| FGR, normal Doppler, normal BPP/NST | Deliver at 39 weeks |
| FGR, abnormal UA/MCA, normal BPP/NST | Deliver at 37 weeks |
| UA AEDF at ≥33 weeks | Deliver |
| UA AEDF at <33 weeks | Intensive surveillance; DV Doppler guides timing |
| UA REDF at ≥30 weeks | Deliver |
| UA REDF at <30 weeks | Hospitalize; daily BPP + Doppler; individualise |
| Reversed DV a-wave or UV pulsations | Deliver regardless of gestational age if viable |
| FGR + pre-eclampsia with severe features | Maternal status may dictate earlier delivery |
Weekly BPP/NST and UA + MCA Doppler is recommended. Reversed UA end-diastolic flow is an ominous finding — delivery is indicated unless the fetus is extremely premature (<30 weeks). — Creasy & Resnik's Maternal-Fetal Medicine
Antenatal Therapy
| Intervention | Evidence |
|---|---|
| Low-dose aspirin 100–150 mg/day (started before 16 weeks in high-risk women) | Significant reduction in FGR risk (RR 0.56, CI 0.44–0.70) — must start early |
| Maternal oxygen therapy | Inconclusive evidence; limited use |
| Vitamins C/E (antioxidants) | Not effective in reducing FGR risk |
| Delayed cord clamping (≥30–60 sec) at delivery | Associated with decreased odds of mortality/major morbidity in preterm FGR infants |
| Magnesium sulphate intrapartum | Neuroprotection when delivery <29 weeks |
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice — Chapter 44: Fetal Growth Restriction (Definition, Diagnosis, Doppler, Management)
- Pfenninger and Fowler's Procedures for Primary Care — Intrauterine Growth Retardation (Ultrasound Parameters)
- Robbins, Cotran & Kumar Pathologic Basis of Disease — Fetal Growth Restriction / Etiology
This is a shared conversation. Sign in to Orris to start your own chat.