Phenytoin
Reading File
Finding Sources
Searching PubMed
phenytoin antiepileptic pharmacology
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a complete reference on Phenytoin, compiled from Katzung's Basic and Clinical Pharmacology (16th ed.) and Goodman & Gilman's Pharmacological Basis of Therapeutics.
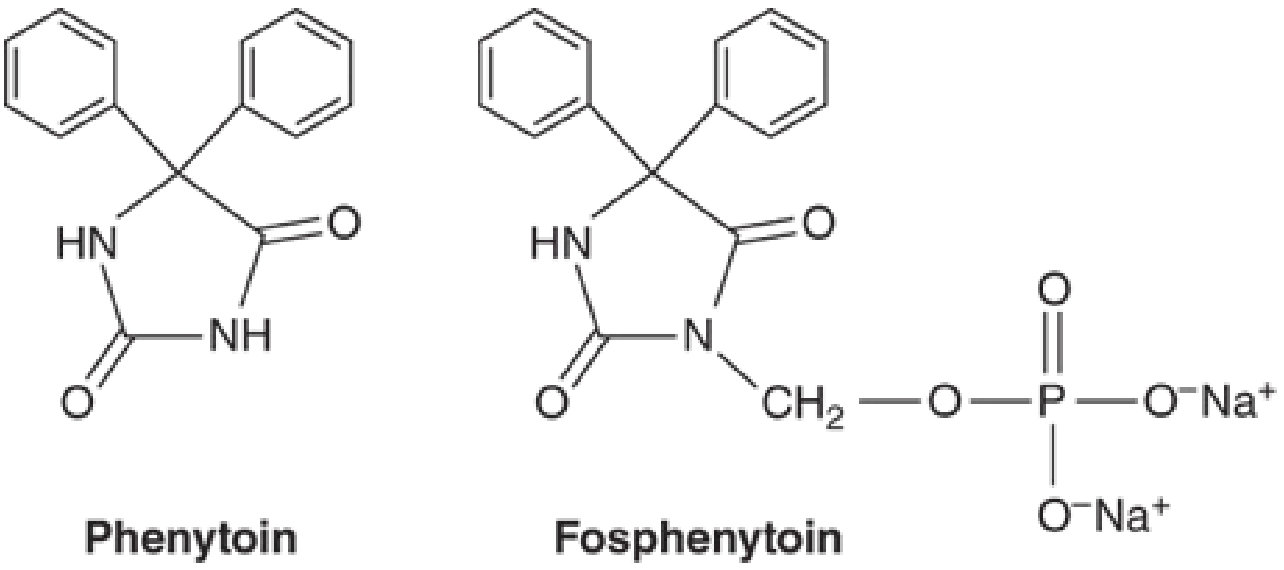
Phenytoin (Diphenylhydantoin)
Chemistry & Formulations
Phenytoin is the 5,5-diphenyl-substituted analog of hydantoin - a five-membered ring structurally related to barbiturates (six-membered ring). Its prodrug, fosphenytoin, is a water-soluble phosphate ester that is rapidly converted to phenytoin in plasma and is preferred for IV use.
- Phenytoin free base: pKa = 8.06-8.33; poorly water soluble
- Phenytoin sodium: dissolves in water (17 mg/mL); the IV solution contains propylene glycol and alcohol at pH 12
- Oral forms: extended-release capsules (peak 4-12 h), prompt-release capsules (peak 1.5-3 h), suspension, and chewable tablets
- Intramuscular injection is not recommended - absorption is unpredictable and precipitation in muscle occurs
Mechanism of Action
Phenytoin limits the repetitive firing of action potentials evoked by sustained depolarization. It does this by slowing the rate of recovery of voltage-activated Na+ channels from inactivation - the effect is both:
- Voltage-dependent: greater effect when membrane is depolarized
- Use-dependent: frequency of firing determines how much drug binds
At therapeutic concentrations, effects are selective on Na+ channels with no change in spontaneous activity or GABA/glutamate responses. At 5-10x therapeutic levels, additional effects appear (reduced spontaneous activity, enhanced GABA responses) - these underlie toxicity.
- Goodman & Gilman's, p. 392-394
Clinical Uses
| Indication | Notes |
|---|---|
| Focal (partial) seizures | First-line (historically), now second-line |
| Generalized tonic-clonic seizures | Focal-to-bilateral and idiopathic |
| Status epilepticus (acute) | IV fosphenytoin preferred |
| NOT effective | Absence epilepsy |
| May worsen | Juvenile myoclonic epilepsy, Dravet syndrome, absence seizures |
Phenytoin is no longer considered first-line for chronic therapy due to adverse effects and drug-drug interactions.
- Katzung's, p. 651
Pharmacokinetics
Absorption
- Highly formulation-dependent; nearly complete GI absorption but time to peak ranges 3-12 hours
- Extensively (~90%) bound to serum albumin - displacement by other drugs (warfarin, valproate, sulfonamides) or hypoalbuminemia increases free (active) drug
Elimination - Saturation (Zero-Order) Kinetics
This is phenytoin's most clinically important pharmacokinetic feature:
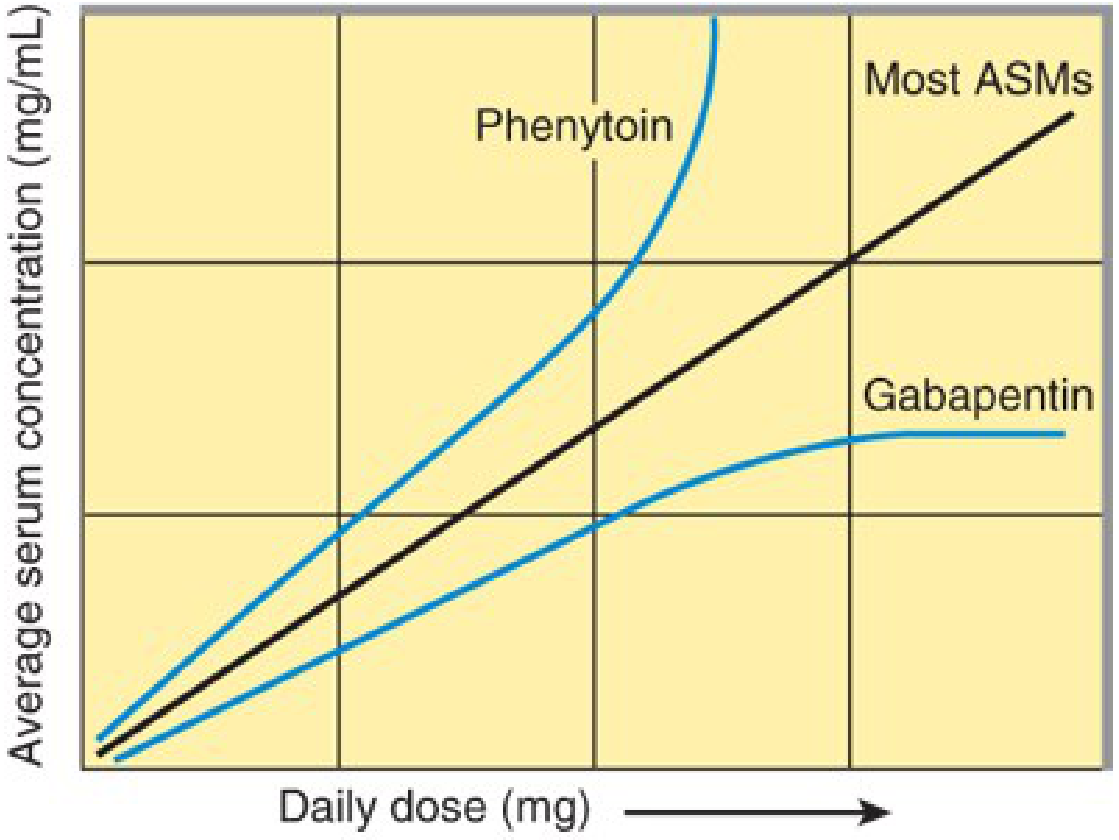
- At low levels: first-order kinetics (constant fraction eliminated per unit time)
- As levels rise into the therapeutic range: hepatic metabolism (CYP2C9/CYP2C19) becomes saturated → shifts to zero-order kinetics (constant quantity per unit time)
- A small dose increase can cause a disproportionately large rise in plasma level, leading to rapid toxicity
- Half-life: 12-36 hours (average 24 h) at low-mid therapeutic range; much longer at higher levels
- Steady-state after dose change: 5-7 days at low levels; up to 4-6 weeks at higher levels
Key Parameters
| Parameter | Value |
|---|---|
| Protein binding | ~90% (albumin) |
| Therapeutic range | 10-20 mcg/mL (total); free level preferred in hypoalbuminemia |
| Metabolism | CYP2C9 (primary), CYP2C19 |
| Kinetics | Zero-order at therapeutic doses |
| Elimination | Urine (inactive metabolites); minimal unchanged |
- Katzung's, p. 652
Correction for Hypoalbuminemia (Sheiner-Tozer formula)
Corrected level = measured total level / [(0.2 × albumin) + 0.1]
Drug Interactions
Phenytoin is a major enzyme inducer (CYP1A2, CYP2C, CYP3A4) and therefore reduces levels of many co-administered drugs.
Drugs that INCREASE phenytoin levels (inhibit CYP2C9/2C19):
- Isoniazid (primarily in slow acetylators)
- Fluoxetine, fluvoxamine
- Fluorouracil
- Metronidazole, miconazole
- Valproate (also displaces from protein binding - dual effect, most significant)
- Amiodarone, cimetidine, omeprazole
Drugs that DECREASE phenytoin levels (enzyme inducers):
- Alcohol (chronic), barbiturates, carbamazepine
Drugs whose levels are REDUCED by phenytoin (induces their metabolism):
- Oral contraceptives (CYP3A4) - risk of contraceptive failure
- Valproate, tiagabine, ethosuximide, lamotrigine, topiramate, zonisamide, felbamate
- Many benzodiazepines, warfarin, cyclosporine
Adverse Effects
Dose-Related (Concentration-Dependent)
These appear in a stepwise fashion as levels rise:
| Plasma Level | Effects |
|---|---|
| 10-20 mcg/mL | Therapeutic range; nystagmus may appear at upper end |
| >20 mcg/mL | Nystagmus (horizontal), mild diplopia |
| >30 mcg/mL | Ataxia, incoordination |
| >40 mcg/mL | Mental changes, lethargy, encephalopathy |
| Very high | Paradoxical seizure worsening, decerebrate posturing |
Chronic/Long-Term Effects (Dose-Independent)
These are the classic adverse effects associated with long-term use:
- Gingival hyperplasia: occurs in ~20% of patients; due to altered collagen metabolism; more common in younger patients; not related to plasma level
- Hirsutism: coarsening of facial hair, especially troublesome in women/girls
- Coarsening of facial features
- Peripheral neuropathy: reduced deep tendon reflexes with chronic use
- Osteomalacia / rickets: increased vitamin D catabolism (CYP induction); bone mineral density loss
- Megaloblastic anemia: impaired folate absorption/metabolism
Idiosyncratic / Hypersensitivity
- Morbilliform rash: most common (~5-10%); may progress to Stevens-Johnson syndrome or toxic epidermal necrolysis (TEN) - rare
- Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS): serious multi-organ hypersensitivity
- Hepatotoxicity: rare but potentially severe
- Hematologic: leukopenia, aplastic anemia (rare)
- Lupus-like syndrome
IV/Infusion Complications
- Purple glove syndrome: purplish-black discoloration + edema + pain distal to IV site; related to propylene glycol vehicle and high pH. Risk is lower with fosphenytoin
- Cardiovascular: hypotension and cardiac arrhythmias (AV block, bradycardia) if infused too rapidly - maximum IV rate is 50 mg/min (25 mg/min in elderly or cardiac patients); fosphenytoin can be infused faster (150 mg PE/min)
Teratogenicity - "Fetal Hydantoin Syndrome"
Phenytoin is Category D / FDA-X equivalent in pregnancy:
- Cleft lip/palate, cardiac defects
- Digital hypoplasia, nail dysplasia
- Growth restriction, dysmorphic facial features
- Cognitive impairment
- Risk is increased with polytherapy
Dosing
- Adults oral: Start at 300 mg/day; increase in increments of no more than 25-30 mg/day due to saturation kinetics
- Loading dose (status epilepticus): IV fosphenytoin 15-20 mg PE/kg at ≤150 mg PE/min
- Monitoring: measure free phenytoin in hypoalbuminemia, renal failure, or when protein displacement interactions are suspected
- Pediatric dosing: weight-based; different formulations have different bioavailability
Summary: Key High-Yield Points
- Mechanism: Na+ channel blocker - slows recovery from inactivation (voltage- and use-dependent)
- Kinetics: Zero-order (Michaelis-Menten / saturation kinetics) at therapeutic doses - small dose increase → large level increase
- Therapeutic range: 10-20 mcg/mL (total); adjust for albumin
- Classic ADRs: gingival hyperplasia, hirsutism, nystagmus, ataxia, fetal hydantoin syndrome
- Enzyme inducer: reduces levels of OCP, warfarin, other ASMs
- IV risk: purple glove syndrome; cardiac toxicity if infused too fast; fosphenytoin preferred
- Not for absence seizures; may worsen JME and Dravet syndrome
- No longer first-line for chronic epilepsy management
Sources: Katzung's Basic and Clinical Pharmacology, 16th ed., pp. 651-654; Goodman & Gilman's Pharmacological Basis of Therapeutics, pp. 392-430
Note on recent evidence: A 2025 network meta-analysis (PMID 39808752) on antiseizure medications in post-stroke seizures and a 2025 Neurocritical Care Society guideline (PMID 39707127) suggest newer agents (levetiracetam, lacosamide) are preferred over phenytoin in acute symptomatic settings, consistent with phenytoin's demotion from first-line status in current practice.
This is a shared conversation. Sign in to Orris to start your own chat.