Cardioplegia
Reading File
Finding Sources
Finding Sources
Searching PubMed
cardioplegia myocardial protection cardiac surgery
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have rich, comprehensive content from four major textbooks plus recent meta-analysis data. Here is a thorough synthesis:
Cardioplegia
Cardioplegia is the deliberate, pharmacologically induced arrest of the heart in diastole, used during cardiac surgery on cardiopulmonary bypass (CPB) to create a still, bloodless operative field while protecting the myocardium from ischemic damage.
1. Purpose and Rationale
The heart is arrested to allow the surgeon to operate on a motionless target. The primary threat during arrest is ischemia - complete cessation of coronary flow deprives cardiomyocytes of oxygen and substrates. The two key strategies used in tandem to minimize this injury are:
- Arrest of electromechanical activity - potassium-induced diastolic arrest reduces myocardial oxygen consumption (MVO2) by ~90%.
- Hypothermia - cooling the myocardium below 22°C further reduces MVO2. Together, potassium arrest + hypothermia (myocardial temp <22°C) can reduce MVO2 by 97%, allowing safe ischemic times of 20-90 minutes depending on the solution used.
- Miller's Anesthesia, 10e, p. 7558
- Barash Clinical Anesthesia, 9e, p. 3339
2. Mechanism of Arrest
Cardioplegia solutions contain supranormal potassium (typically 10-40 mEq/L). Elevated extracellular [K⁺] reduces the transmembrane resting potential, bringing it closer to the threshold potential, and maintains the myocyte in a depolarized, electrically silent state. The heart arrests in diastole - the most energetically favorable phase - within:
- 30-60 seconds with antegrade delivery
- 2-4 minutes with retrograde delivery
Once the cross-clamp is removed and warm normokalemic blood reperfuses the coronaries, electromechanical activity resumes.
- Morgan & Mikhail Clinical Anesthesiology, 7e, p. 818
3. Components of Cardioplegia Solutions
Despite considerable variation between institutions, solutions share common design principles:
| Component | Role | Typical Values |
|---|---|---|
| Potassium (arrest agent) | Depolarizes resting membrane, induces arrest | 10-40 mEq/L (induction); ~10 mEq/L (maintenance) |
| Sodium | Reduced relative to plasma to counteract ischemia-related intracellular Na⁺ rise | <140 mEq/L |
| Calcium | Maintains cellular integrity | 0.7-1.2 mmol/L |
| Magnesium | Controls intracellular Ca²⁺ influx | 1.5-15 mmol/L |
| Buffer (bicarbonate, histidine, THAM) | Neutralizes acidic metabolites; alkalotic solutions improve preservation | Variable |
| Osmotic agents (mannitol) | Reduces cellular edema; solution kept slightly hypertonic | Variable |
| Membrane stabilizers (lidocaine, glucocorticoids) | Reduce ionic channel activation | Variable |
| Energy substrates (glucose, glutamate, aspartate) | Fuel anaerobic metabolism, replenish ATP | Variable |
- Morgan & Mikhail, 7e, p. 819; Miller's Anesthesia, 10e, p. 7559
4. Cardioplegia Delivery Routes
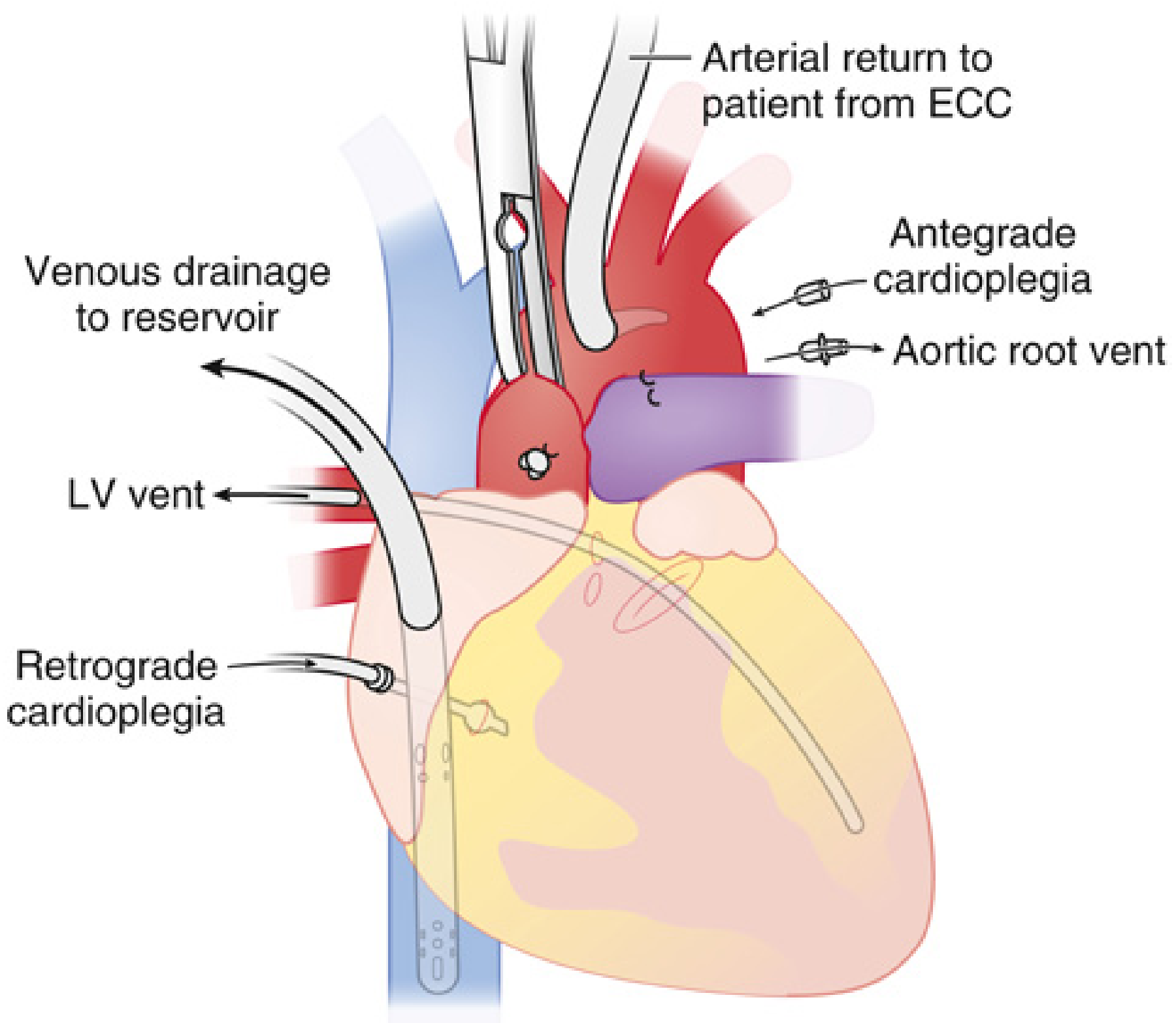
Antegrade
- Delivered into the aortic root (proximal to the cross-clamp) at 60-100 mmHg, or directly into individual coronary ostia when the aorta is opened (e.g., aortic valve replacement) or in the setting of significant aortic insufficiency (AI).
- Mimics normal coronary flow direction.
- Limitation: High-grade coronary stenoses can block distal delivery - the areas that need protection most receive the least.
Retrograde
- A balloon-cuffed catheter is placed through the right atrium into the coronary sinus; solution is delivered at 200-400 mL/min to a venous pressure of 30-50 mmHg.
- Perfuses the coronary circulation in the reverse (venous) direction.
- Advantages: More uniform distribution in diffuse coronary artery disease; independent of aortic valve competence; particularly useful when AI would cause antegrade solution to reflux into the LV.
- Limitation: Slower onset of arrest (2-4 min vs. 30-60 sec antegrade).
Combined Antegrade + Retrograde
-
Many centers use both simultaneously or sequentially. Evidence suggests the combination is superior to either alone for maximal protection. During CABG, cardioplegia can also be delivered via completed distal anastomoses ("graft cardioplegia").
-
Barash, 9e, p. 3340; Morgan & Mikhail, 7e, p. 818-819; Schwartz's Principles of Surgery, 11e, p. 835
5. Cardioplegia Solution Types
Crystalloid vs. Blood Cardioplegia
- Crystalloid cardioplegia (e.g., St. Thomas solution): Simple, reproducible. However, it contains no oxygen-carrying capacity.
- Blood cardioplegia: Blood is mixed with crystalloid in ratios of 4:1 or 8:1 (blood:crystalloid, for Buckberg and St. Thomas-based formulas). Blood contains oxygen and provides buffering capacity. Most centers in North America now favor blood cardioplegia, particularly for high-risk patients.
Temperature
-
Cold cardioplegia (4-15°C): Most traditional. Delivered intermittently every 20-30 minutes. Hypothermia reduces metabolism but must be repeated as the heart gradually rewarns (from adjacent aorta, ambient air).
-
Warm/Tepid (normothermic) cardioplegia: Associated with better postoperative cardiac indices in some studies, but must be delivered continuously since the metabolic protective effect of cold is absent. Requires an unobstructed surgical field.
-
True normothermia raises additional concerns about losing the neuroprotective effects of systemic hypothermia.
-
Barash, 9e, p. 3340-3341; Morgan & Mikhail, 7e, p. 819
6. Dosing Regimens
Multidose (Intermittent)
- Induction ("high-K"): ~1,000-1,500 mL of high-potassium solution (20-30 mEq/L) to achieve diastolic arrest.
- Maintenance ("low-K"): 200-500 mL doses of low-potassium solution (~10 mEq/L) every 20-30 minutes to replenish nutrients, flush metabolites, and maintain arrest.
Single-Dose Solutions
Increasingly used in adult cardiac surgery. Two notable formulations:
| Solution | Ratio | Safe Arrest Time | Notes |
|---|---|---|---|
| Del Nido | 1:4 (blood:crystalloid) | ~45 min | Contains lidocaine, MgSO₄, NaHCO₃, mannitol, KCl; popular in pediatrics and adult cases with short cross-clamp times |
| HTK (Custodiol) | Crystalloid only | ~60-90 min | Histidine-tryptophan-ketoglutarate; used in transplantation and complex cases |
- Miller's Anesthesia, 10e, p. 7559; Barash, 9e, p. 3350
7. Monitoring Adequacy of Myocardial Protection
Intraoperative assessment of protection is empirical, based on:
- ECG quiescence (isoelectric arrest confirmed)
- Time since last dose (relative to expected safe arrest window)
- Myocardial temperature
- Ventricular filling state (TEE) - LV distension indicates inadequate venting, which increases wall tension and MVO2, worsening protection. Particularly important in AI patients.
Postoperatively: potassium levels may be elevated from cardioplegia washout.
- Miller's Anesthesia, 10e, p. 7559-7560; Barash, 9e, p. 3352
8. Reversal
Electromechanical activity is restored by:
-
Removing the aortic cross-clamp, allowing warm normokalemic blood to reperfuse the coronaries.
-
Alternatively, a "hot shot" - infusion of warm blood through the cardioplegia cannulas as a reperfusion substrate - can be given before cross-clamp removal to reduce reperfusion injury and flush metabolites.
-
Miller's Anesthesia, 10e, p. 7560
9. Special Considerations
- Aortic insufficiency: Antegrade cardioplegia refluxes into the LV rather than the coronary ostia - direct ostial delivery or retrograde approach is required; TEE monitoring for LV distension is critical.
- Severe coronary stenoses: Differential distribution of antegrade cardioplegia occurs; retrograde delivery or revascularization of the territory first is recommended.
- Ventricular fibrillation during cooling: VF below 28-29°C consumes high-energy phosphates rapidly - cardioplegia should be established immediately.
- Hypothermia + CPB: At 20°C, pump flows as low as 1.2 L/min/m² may be adequate, allowing complex aortic arch reconstruction.
10. Recent Evidence - Del Nido Cardioplegia
Three recent meta-analyses (2024-2025) specifically address del Nido cardioplegia:
- Li et al. (2024) [PMID 38909234]: Del Nido vs. cold blood cardioplegia in adult cardiac surgery - found comparable outcomes, with del Nido offering the convenience of fewer reapplications.
- Yamashita et al. (2025) [PMID 39909765]: Del Nido in isolated CABG - meta-analysis showing non-inferior myocardial protection vs. conventional formulas.
- Yamashita et al. (2025) [PMID 39797758]: Del Nido in reduced EF patients - favorable results supporting its use in high-risk subgroups.
Summary Table
| Parameter | Options | Notes |
|---|---|---|
| Vehicle | Crystalloid / Blood | Blood favored; 4:1 or 8:1 ratio typical |
| Temperature | Cold / Tepid / Warm | Cold most common; warm requires continuous delivery |
| Route | Antegrade / Retrograde / Both | Combined approach preferred in diffuse CAD or AI |
| Dosing | Intermittent / Single-dose | Del Nido ~45 min, HTK ~60-90 min |
| Arrest agent | Potassium | 20-30 mEq/L (induction), ~10 mEq/L (maintenance) |
Sources: Morgan & Mikhail Clinical Anesthesiology 7e; Miller's Anesthesia 10e; Barash Clinical Anesthesia 9e; Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.