Connections and functions of internal capsule
Reading File
Finding Sources
Searching the Web
internal capsule connections functions anatomy fiber tracts
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Excellent - I now have comprehensive textbook data and diagrams. Here is the full answer:
Internal Capsule: Connections and Functions
Overview
The internal capsule is a compact lamina of white matter representing the largest projection fiber tract in the brain. It carries afferent and efferent nerve fibers passing between the brainstem and the cerebral hemispheres. It continues rostrally as the corona radiata and caudally as the cerebral peduncles (basis pedunculi).
- Medial relations: Caudate nucleus (anteriorly) and thalamus (posteriorly)
- Lateral relation: Lenticular nucleus (globus pallidus + putamen)
In horizontal section, the internal capsule forms a V-shape (like two letter Vs with their points facing inward - also called the Flechsig shape), with the convexity facing medially.
Parts and Their Connections
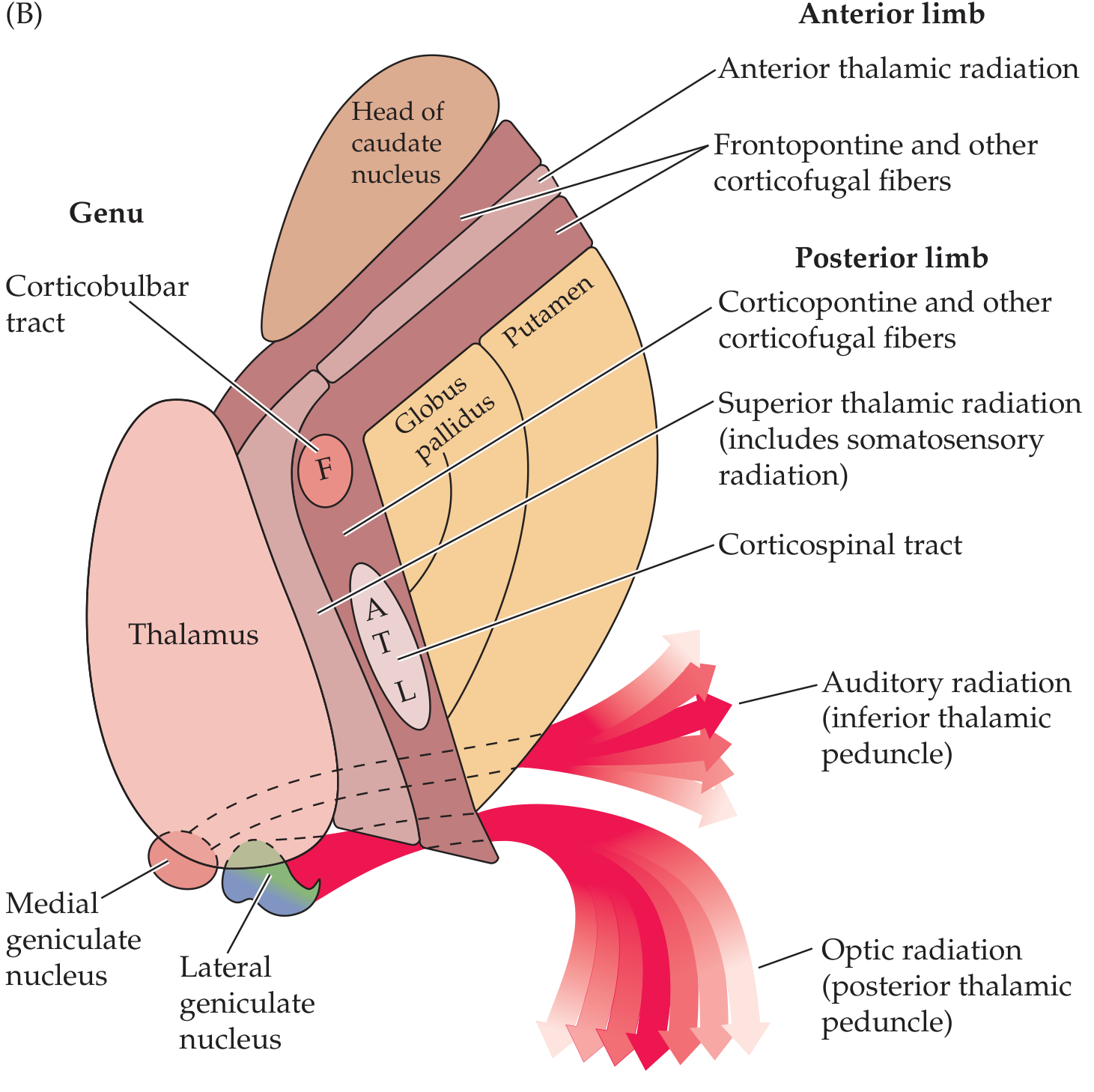
1. Anterior Limb (Lenticulocaudate Segment)
- Boundaries: Separates the lenticular nucleus (laterally) from the head of the caudate nucleus (medially)
- Length: ~2 cm
- Fibers carried:
- Frontopontine fibers (Arnold's bundle) - from frontal cortex to pontine nuclei
- Anterior thalamic radiation - connecting frontal lobe and anterior/medial thalamic nuclei (mediodorsal nucleus)
- Corticothalamic and thalamocortical fibers (frontal lobe <-> thalamus)
- Caudate-putamen fibers
- Function: Frontal lobe relay to pons and thalamic connections involved in prefrontal/limbic activity
2. Genu ("Knee")
- Position: At the apex of the pallidal part of the lentiform nucleus, at the level of the foramen of Monro, between the anterior and posterior limbs
- Fibers carried:
- Corticobulbar (corticonuclear) fibers - from motor cortex to cranial nerve nuclei in the brainstem
- Corticoreticular fibers - to both sides of the brainstem reticular formation
- Motor corticopontine fibers (possibly)
- Function: Voluntary control of head, face, and neck musculature via cranial nerves; the genu syndrome (lesion here) causes facial and lingual hemiparesis with relatively mild limb weakness
3. Posterior Limb (Lenticulothalamic Segment)
- Boundaries: Separates the lenticular nucleus (laterally) from the thalamus (medially)
- Length: ~3-4 cm
- Fibers carried (anterior to posterior):
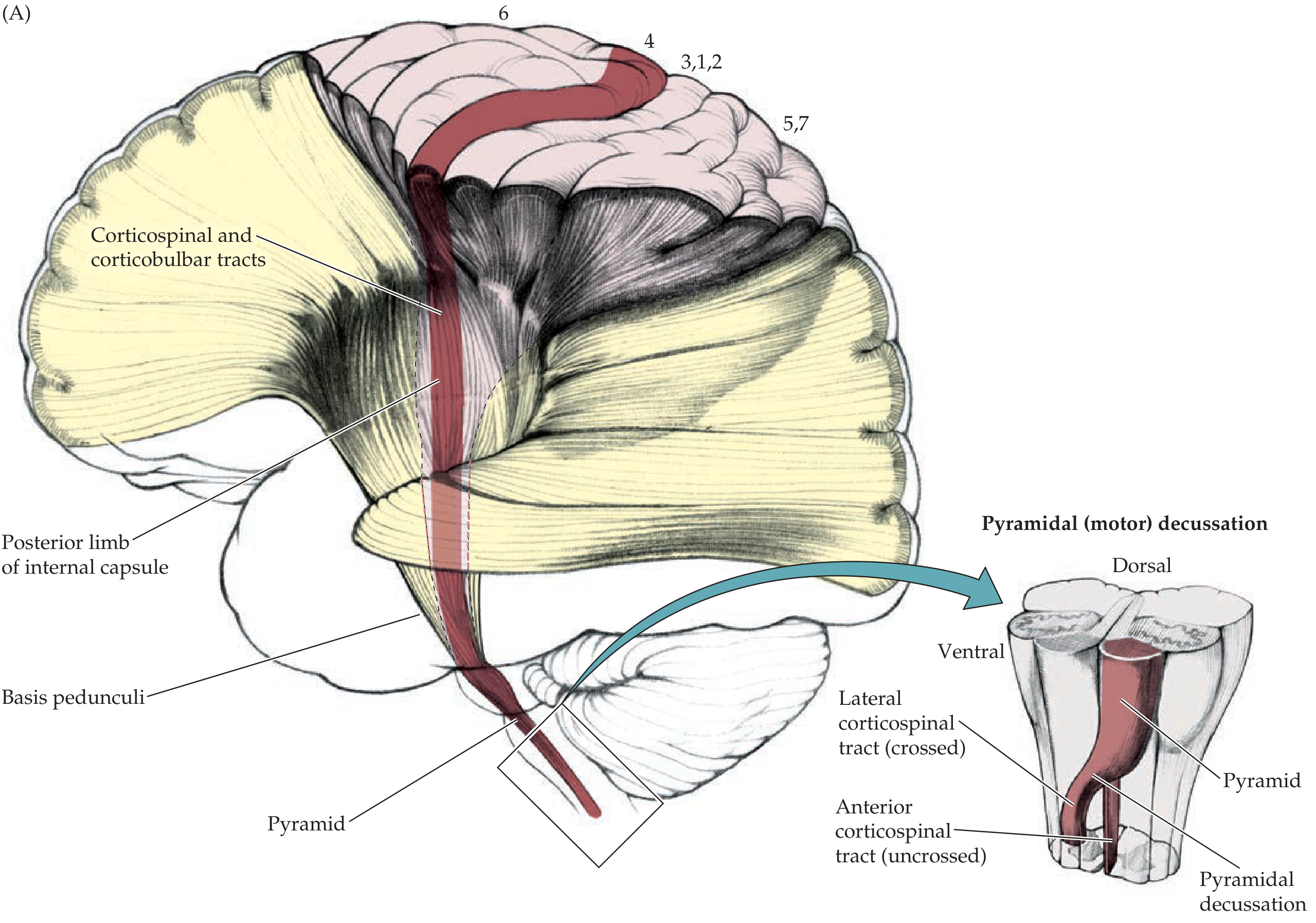
- Corticospinal tract (pyramidal tract) - occupies the posterior half; somatotopically organized: face (F) most anteriorly, then arm (A), trunk (T), leg (L) most posteriorly
- Superior thalamic radiation - includes somatosensory fibers from VPL/VPM nuclei of thalamus to postcentral gyrus (parietal lobe)
- Corticorubral fibers - cortex to red nucleus
- Corticothalamic fibers - cortex to thalamus
- Corticopontine fibers (parietal, temporal, occipital portions)
- Function: Voluntary motor control of limbs and trunk; relay of somatosensory information to cortex
4. Retrolenticular Segment
- Position: Behind the lenticular nucleus
- Fibers carried:
- Visual (optic) radiations (Gratiolet's radiation / geniculo-calcarine tract) - from lateral geniculate nucleus (LGN) to primary visual cortex (calcarine cortex)
- Corticotectal fibers (to superior colliculus)
- Corticonigral and corticotegmental fibers
- Function: Transmission of visual information from thalamus to occipital cortex
5. Sublenticular Segment
- Position: Below the lenticular nucleus
- Fibers carried:
- Auditory radiations (inferior thalamic peduncle) - from medial geniculate nucleus (MGN) to primary auditory cortex (Heschl's gyri, temporal lobe)
- Temporopontine and parietopontine fibers
- Function: Relay of auditory information from thalamus to temporal cortex
Summary Table
| Part | Medial Border | Lateral Border | Key Fibers | Function |
|---|---|---|---|---|
| Anterior limb | Head of caudate | Lenticular nucleus | Frontopontine, anterior thalamic radiation | Frontal-thalamic, frontal-pontine relay |
| Genu | Caudate/Thalamus junction | Apex of lenticular nucleus | Corticobulbar, corticoreticular | Cranial nerve motor control |
| Posterior limb | Thalamus | Lenticular nucleus | Corticospinal, superior thalamic radiation (somatosensory) | Limb/trunk motor + sensory relay |
| Retrolenticular | - | Behind lenticular | Optic radiation | Visual pathway |
| Sublenticular | - | Below lenticular | Auditory radiation | Auditory pathway |
Blood Supply
| Region | Artery |
|---|---|
| Anterior limb | Recurrent artery of Heubner (branch of ACA) |
| Genu + middle/inferior posterior limb | Anterior choroidal artery (from ICA) |
| Superior anterior + posterior limb | Lenticulostriate arteries (branches of MCA) |
Clinical Significance
- Posterior limb lesion (e.g., hypertensive hemorrhage or lacunar infarct): Contralateral hemiplegia (face, arm, and leg - "pure motor stroke") due to corticospinal tract involvement. If sensory radiations are also affected, hemianesthesia is added.
- Genu lesion: "Capsular genu syndrome" - contralateral facial and lingual weakness with mild limb involvement, sometimes with dysarthria.
- Retrolenticular lesion: Contralateral homonymous hemianopia (optic radiations).
- Sublenticular lesion: Contralateral superior quadrantanopia or cortical deafness (auditory radiation).
- Because all motor and sensory fibers are tightly compacted, even small capsular lesions produce large deficits - a key principle distinguishing internal capsule strokes from cortical strokes.
Sources: Localization in Clinical Neurology, 8e - Anatomy of the Motor System, pp. 31-32; Neuroanatomy through Clinical Cases, 3rd Ed. - Lateral Corticospinal Tract, pp. 256-258; Bradley & Daroff's Neurology in Clinical Practice
Ascending tracts
Finding Sources
Searching the Web
ascending sensory tracts spinal cord dorsal column spinothalamic anatomy
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive textbook data and a key diagram. Here is the full answer:
Ascending Tracts of the Spinal Cord
Ascending (sensory) tracts carry afferent information from the periphery to the brain. They are found in the white matter of the spinal cord and are organized into conscious (reach the cortex) and unconscious (reach the cerebellum) pathways.
General Principles
- Almost all sensory input enters the spinal cord via dorsal nerve roots
- The central end of the dorsal root splits into:
- Lateral bundle - finely myelinated/unmyelinated fibers (pain, temperature) - enter the zone of Lissauer
- Medial bundle - heavily myelinated fibers (touch, proprioception) - enter dorsal funiculus directly
- All ascending pathways use a 3-neuron relay: 1st order (periphery to spinal cord/medulla), 2nd order (to thalamus), 3rd order (thalamus to cortex)
I. CONSCIOUS SENSORY PATHWAYS
A. Posterior Column - Medial Lemniscal (DCML) Pathway
Modalities: Fine/discriminative touch, vibration, proprioception (joint position), two-point discrimination, stereognosis, pressure touch, weight perception
| Neuron | Cell Body | Pathway | Decussation |
|---|---|---|---|
| 1st order | Dorsal root ganglion | Enters dorsal funiculus ipsilaterally and ascends the whole way to medulla | None in spinal cord |
| 2nd order | Nucleus gracilis / nucleus cuneatus (medulla) | Internal arcuate fibers cross → ascend as medial lemniscus through brainstem | At medulla (sensory decussation) |
| 3rd order | VPL nucleus of thalamus | Thalamic somatosensory radiation → posterior limb of internal capsule → postcentral gyrus (areas 3, 1, 2) | None |
Key anatomical points:
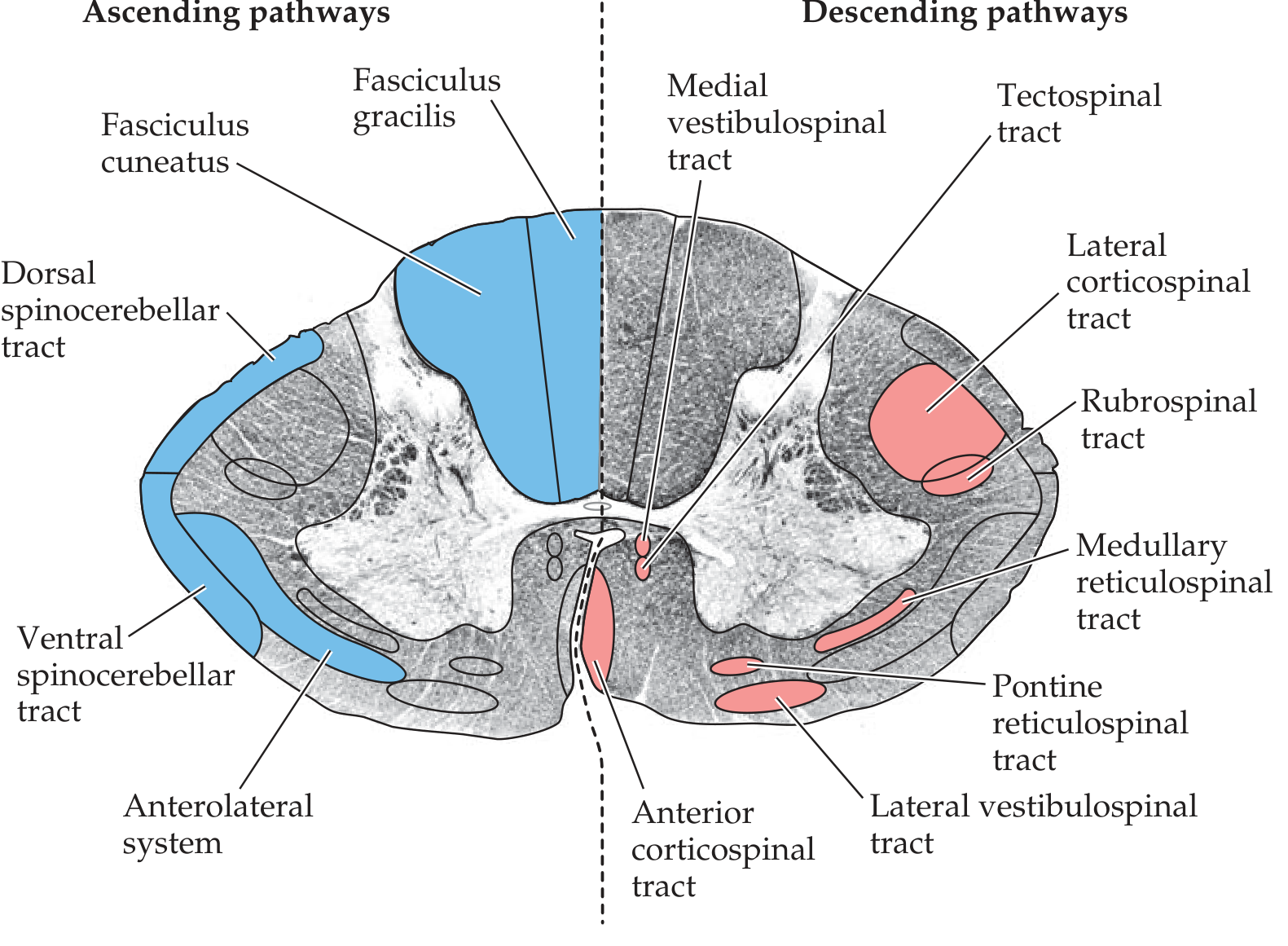
- Fasciculus gracilis (Goll's column): fibers from sacral, lumbar, and lower 6 thoracic levels - located medially in dorsal column
- Fasciculus cuneatus (Burdach's column): fibers from upper 6 thoracic and all cervical levels - located laterally in dorsal column
- Somatotopy in dorsal columns: sacral most medial, cervical most lateral (opposite of anterolateral system)
- The medial lemniscus rotates as it ascends: in the medulla it is vertical (leg medial), in the pons it rotates to horizontal (leg lateral), at VPL it terminates with leg lateral and arm medial
Face equivalent: Trigeminal lemniscus → VPM nucleus of thalamus (not VPL)
B. Anterolateral System (Spinothalamic + related tracts)
1. Lateral Spinothalamic Tract (Neospinothalamic)
Modalities: Pain (sharp, localized), temperature
| Neuron | Cell Body | Pathway | Decussation |
|---|---|---|---|
| 1st order | Dorsal root ganglion | Enters Lissauer's tract → dorsal horn (lamina I & V) | None |
| 2nd order | Dorsal horn (laminae I & V) | Crosses ventral white commissure (over 2-3 segments) → ascends in lateral funiculus | In spinal cord - at same level (2-3 segments above entry) |
| 3rd order | VPL nucleus of thalamus | → Postcentral gyrus (areas 3, 1, 2) | None |
Important: Because decussation occurs 2-3 segments above entry, a spinal cord lesion causes pain/temperature loss a few segments below the lesion on the contralateral side.
Somatotopy: Legs represented most laterally, arms medially (sacral fibers are most peripheral/lateral - "onion peel" arrangement)
2. Anterior (Ventral) Spinothalamic Tract
Modalities: Crude touch, pressure, light touch (also carried by dorsal columns - so rarely lost alone)
- Pathway: similar to lateral spinothalamic - 1st order synapses in dorsal horn → 2nd order crosses ventral commissure → ascends in anterior funiculus → VPL → somatosensory cortex
- Because light touch is also carried by dorsal columns, anterior spinothalamic lesions alone rarely cause detectable loss
3. Spinoreticular Tract (Paleospinothalamic System)
Modalities: Poorly localized, dull, aching pain; arousal and emotional aspects of pain
- 2nd order axons ascend bilaterally → synapse in brainstem reticular formation (medullary-pontine) → project to intralaminar thalamic nuclei (centromedian nucleus) → wide cortical projections
- This is the phylogenetically older pain pathway
- Explains why spinothalamic cordotomy (cutting lateral spinothalamic) may relieve sharp pain but not the emotional suffering of chronic pain
4. Spinomesencephalic Tract
- Projects to periaqueductal gray (PAG) and superior colliculus
- Involved in pain modulation (descending inhibitory pathways originate here), orientation responses, and reflexive responses to pain
II. UNCONSCIOUS SENSORY PATHWAYS (Spinocerebellar)
These carry proprioceptive information to the cerebellum for coordination of movement - information never reaches conscious perception.
A. Dorsal Spinocerebellar Tract (DSCT)
Modality: Proprioception from lower limbs (individual muscle spindle and tendon organ activity)
| Feature | Detail |
|---|---|
| 1st order | Dorsal root ganglion → synapse in nucleus dorsalis of Clarke (Clarke's column, C8-L3, lamina VII) |
| 2nd order | Ascends ipsilaterally in dorsal lateral funiculus |
| Destination | Inferior cerebellar peduncle → ipsilateral cerebellar cortex (vermis + intermediate zone) |
| Decussation | None - entirely ipsilateral |
B. Ventral Spinocerebellar Tract (VSCT)
Modality: Proprioception from lower limbs, but reflects activity of spinal cord interneurons (feedback about descending pathway activity)
| Feature | Detail |
|---|---|
| 1st order | Dorsal root ganglion → dorsal horn |
| 2nd order | Crosses ventral commissure → ascends contralaterally in lateral funiculus (ventral to DSCT) |
| Destination | Superior cerebellar peduncle → recrosses inside cerebellum → ipsilateral effect |
| Note | Crosses twice - net effect is ipsilateral |
C. Cuneocerebellar Tract
Modality: Proprioception from upper limbs and neck
- 1st order fibers ascend in fasciculus cuneatus → synapse in external (accessory) cuneate nucleus in medulla
- 2nd order fibers enter cerebellum via inferior cerebellar peduncle ipsilaterally
- Functional equivalent of DSCT for upper limbs
D. Rostral Spinocerebellar Tract
Modality: Proprioception from upper limb interneurons (equivalent of VSCT for upper limbs)
- Travels via superior and inferior cerebellar peduncles
Summary Table
| Tract | Column | Modality | 1st Order Synapse | Decussation | 2nd → 3rd Relay | Destination |
|---|---|---|---|---|---|---|
| Dorsal column (gracilis) | Dorsal (medial) | Fine touch, vibration, proprioception (leg) | Nucleus gracilis (medulla) | Medulla (sensory decussation) | VPL → postcentral gyrus | Conscious |
| Dorsal column (cuneatus) | Dorsal (lateral) | Fine touch, vibration, proprioception (arm) | Nucleus cuneatus (medulla) | Medulla | VPL → postcentral gyrus | Conscious |
| Lateral spinothalamic | Lateral | Pain, temperature | Dorsal horn (laminae I, V) | Spinal cord (2-3 segs above) | VPL → postcentral gyrus | Conscious |
| Anterior spinothalamic | Anterior | Crude touch, pressure | Dorsal horn (laminae VI-VII) | Spinal cord | VPL → postcentral gyrus | Conscious |
| Spinoreticular | Anterolateral | Dull pain, arousal | Dorsal horn | Bilateral | Reticular formation → intralaminar thalamus | Conscious (diffuse) |
| Dorsal spinocerebellar | Lateral (dorsal) | Proprioception (leg) | Clarke's column | None | Inferior cerebellar peduncle | Unconscious (cerebellum) |
| Ventral spinocerebellar | Lateral (ventral) | Interneuron activity (leg) | Dorsal horn | Crosses twice | Superior cerebellar peduncle | Unconscious (cerebellum) |
| Cuneocerebellar | - | Proprioception (arm) | External cuneate nucleus | None | Inferior cerebellar peduncle | Unconscious (cerebellum) |
Key Clinical Correlations
| Lesion | Deficit |
|---|---|
| Dorsal column lesion | Ipsilateral loss of fine touch, vibration, proprioception below the lesion; positive Romberg; sensory ataxia |
| Lateral spinothalamic lesion | Contralateral pain and temperature loss, starting 2-3 segments below the lesion |
| Brown-Séquard syndrome (hemicord) | Ipsilateral DCML loss + ipsilateral UMN weakness; contralateral spinothalamic loss |
| Syringomyelia | Bilateral pain/temperature loss at the affected segment (central cord lesion crossing ventral commissure) with preserved dorsal columns ("cape distribution") |
| Tabes dorsalis (syphilis) | Dorsal column degeneration - loss of proprioception, vibration; Romberg positive; lightning pains |
| Subacute combined degeneration (B12 deficiency) | Dorsal columns + lateral corticospinal tracts - sensory ataxia + UMN signs |
Sources: Localization in Clinical Neurology, 8e - Ascending Tracts, pp. 244-245; Neuroanatomy through Clinical Cases, 3rd Ed. - Spinothalamic Tract and Other Anterolateral Pathways, pp. 303-305; Neuroanatomy through Clinical Cases, 3rd Ed. - Cerebellar Input Pathways, p. 736
This is a shared conversation. Sign in to Orris to start your own chat.