Give me 40 ECG cases practice (ICU level and OPD) ECG all details according to disease ECG kaise dekhe with photos case and uses treatment
Reading File
Finding Sources
Searching Images
ECG interpretation 12 lead electrocardiogram cases
Searching Images
STEMI myocardial infarction ECG ST elevation VF ventricular fibrillation cardiac arrest
Searching Images
complete heart block third degree AV block atrial flutter ECG pacemaker
Searching Images
hyperkalemia hypokalemia ECG changes peaked T waves WPW syndrome Wolff-Parkinson-White delta wave
Searching Images
pulmonary embolism ECG S1Q3T3 right heart strain ventricular tachycardia torsades de pointes
Now I have rich image resources. Let me compile the comprehensive 40 ECG cases guide.
🫀 40 ECG Cases — ICU + OPD Practice Guide
ECG Kaise Dekhe: Systematic Approach + Disease Patterns + Photos + Treatment
📋 ECG DEKHNE KA SYSTEMATIC APPROACH (7-Step Method)
Har ECG ko is order mein dekho:
- Rate — 300 ÷ R-R squares (normal: 60–100 bpm)
- Rhythm — Regular ya irregular? P waves hain?
- P waves — Shape, axis, har QRS ke aage?
- PR interval — Normal: 120–200 ms (3–5 small squares)
- QRS — Normal: <120 ms (<3 small squares)
- ST segment — Elevation ya depression?
- T waves — Upright, inverted, peaked?
🔴 ICU EMERGENCIES (Cases 1–20)
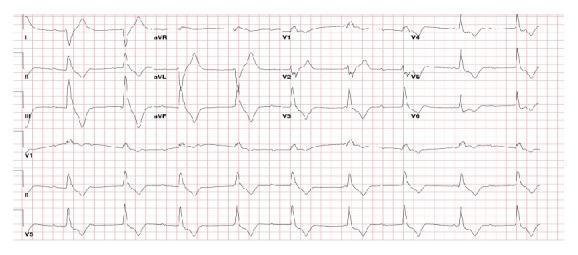
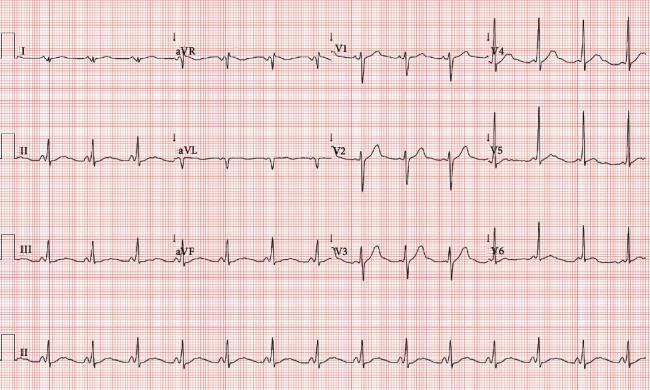
CASE 1 — Anterior STEMI (LAD Occlusion)
Clinical scenario: 55M, sudden chest pain, diaphoresis, BP 90/60
ECG:
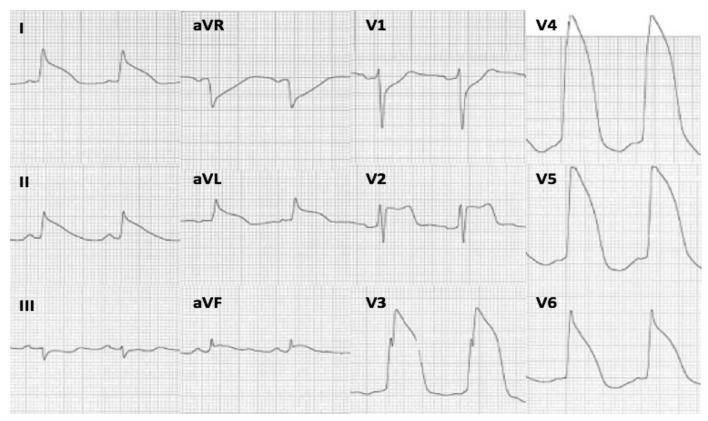
| ECG Feature | Finding |
|---|---|
| ST elevation | V1–V6, I, aVL (tombstone pattern) |
| Reciprocal changes | ST depression in aVR, III, aVF |
| QRS morphology | Lambda waves / QS pattern V1–V3 |
| Artery involved | LAD proximal occlusion |
Kaise pehchano: V1–V4 mein ST elevation = anterior STEMI. "Tombstone" = QRS aur T wave ek saath upar → very large MI.
Treatment:
- 🚨 Activate cath lab immediately — door-to-balloon <90 min
- Aspirin 325 mg + Clopidogrel/Ticagrelor loading
- Heparin UFH 60 IU/kg bolus
- Primary PCI (preferred) or thrombolysis (Streptokinase/Alteplase) if PCI unavailable
- Morphine, O₂, Nitrates (no nitrates if RV infarct)
- ICCU monitoring, echo
CASE 2 — Inferior STEMI (RCA Occlusion)
Clinical scenario: 60M, chest pain radiating to jaw, bradycardia HR 45
ECG:
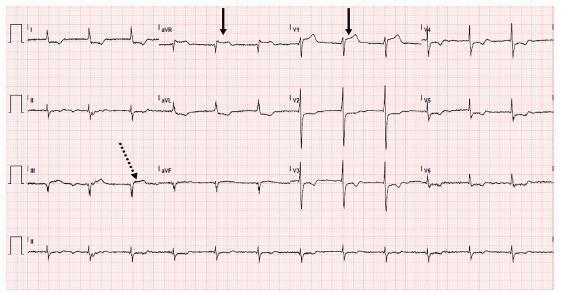
| ECG Feature | Finding |
|---|---|
| ST elevation | II, III, aVF |
| Reciprocal depression | I, aVL |
| V1/aVR elevation | Suggests proximal RCA or RV involvement |
| Key clue | III > II elevation → RCA territory |
RV infarction pehchanein: Right-sided leads lagao (V4R mein ST elevation ≥1 mm = RV infarct)
Treatment:
- Primary PCI for RCA
- ⚠️ NO nitrates if RV infarct (preload-dependent!)
- IV fluid challenge (NS 250–500 mL) for hypotension
- Atropine for bradycardia
- Temporary pacemaker if needed
CASE 3 — Inferior STEMI + Atrial Fibrillation
Clinical scenario: 65F, palpitations + chest pain, irregular pulse
ECG:
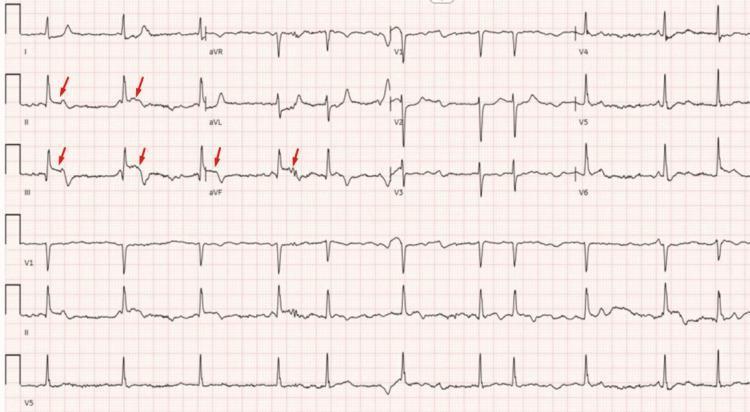
| Feature | Finding |
|---|---|
| Rhythm | Irregularly irregular, no P waves |
| ST changes | Tombstone elevation in II, III, aVF |
| Reciprocal | Depression in aVL |
Kaise pehchano: Irregular rhythm + inferior ST elevation = AF + acute MI. Emergency!
Treatment:
- Primary PCI immediately
- Rate control with caution (avoid AV nodal blockers if hypotensive)
- Anticoagulation — unfractionated heparin
- DC cardioversion if hemodynamically unstable
CASE 4 — NSTEMI / Lateral Ischemia
Clinical scenario: 58M, exertional chest pain, troponin mildly elevated
ECG:
| ECG Feature | Finding |
|---|---|
| T wave inversions | V5, V6 (lateral wall) |
| ST depression | V5–V6 subendocardial ischemia |
| No ST elevation | → NSTEMI, not STEMI |
Kaise pehchano: No elevation + troponin rise = NSTEMI. T inversion in V5/V6 = lateral wall ischemia (LCx territory).
Treatment:
- Dual antiplatelet: Aspirin + Ticagrelor
- Anticoagulation: LMWH (Enoxaparin) or UFH
- High-intensity statin (Atorvastatin 80 mg)
- Beta-blocker, ACE inhibitor
- Coronary angiography within 24–72 hrs (GRACE score guided)
CASE 5 — Complete Heart Block (3rd Degree AV Block)
Clinical scenario: 70M, syncope, HR 35, post-inferior MI
ECG:
| ECG Feature | Finding |
|---|---|
| Atrial rate | ~70–80 bpm (P waves march through independently) |
| Ventricular rate | ~35–50 bpm (escape rhythm) |
| PR interval | No fixed relationship (AV dissociation) |
| QRS width | Wide if infranodal; Narrow if junctional |
Kaise pehchano: P waves aur QRS completely independent → complete AV dissociation = 3rd degree block.
Treatment:
- Atropine 0.5–1 mg IV (junctional block mein kaam karta hai)
- Transcutaneous pacing (temporary emergency)
- Dopamine/Epinephrine infusion if unstable
- Permanent pacemaker implantation — definitive treatment
- Identify cause: inferior MI (RCA), Lyme disease, medications
CASE 6 — Complete Heart Block (Narrow Escape)
Clinical scenario: 65F, dizzy spells, HR 36 bpm
ECG:
| Feature | Finding |
|---|---|
| Escape rate | ~36 bpm (junctional) |
| QRS | Narrow — supraHisian escape |
| P waves | Present, march independently |
Kaise pehchano: Narrow QRS escape = junctional (better prognosis than ventricular escape). Still needs pacemaker!
Treatment: Same as Case 5. Narrow QRS = may respond to Atropine briefly.
CASE 7 — 3rd Degree Block (Ventricular Escape, Wide QRS)
ECG:
| Feature | Finding |
|---|---|
| QRS morphology | Widened, notched (ventricular escape) |
| Rate | Very slow |
| Risk | High — Stokes-Adams attacks, sudden death |
Treatment: Emergency temporary pacing → permanent pacemaker.
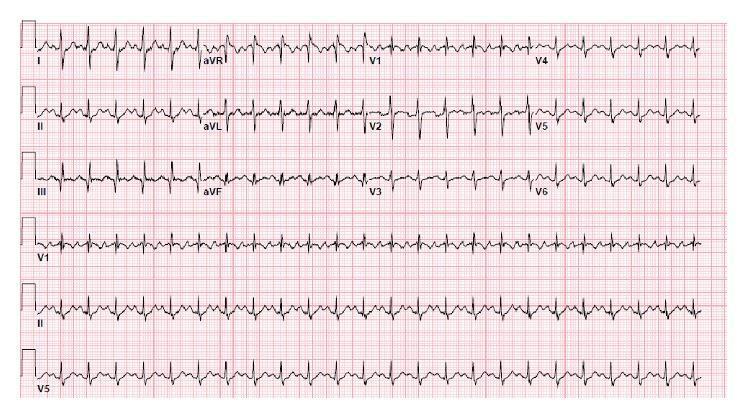
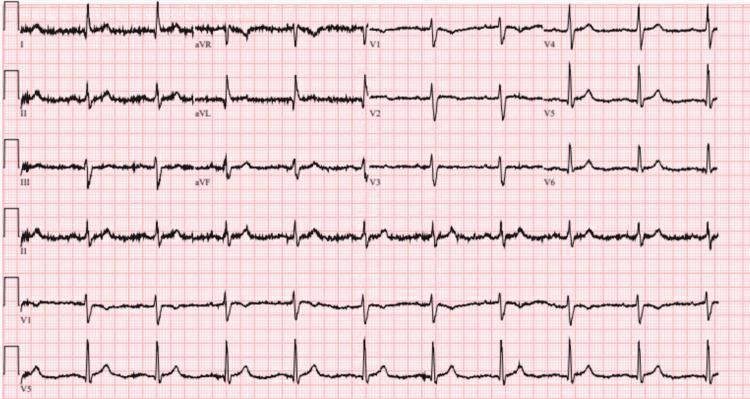
CASE 8 — Atrial Fibrillation (Rapid Ventricular Response)
Clinical scenario: 55F, palpitations, HR 140 irregular
ECG:
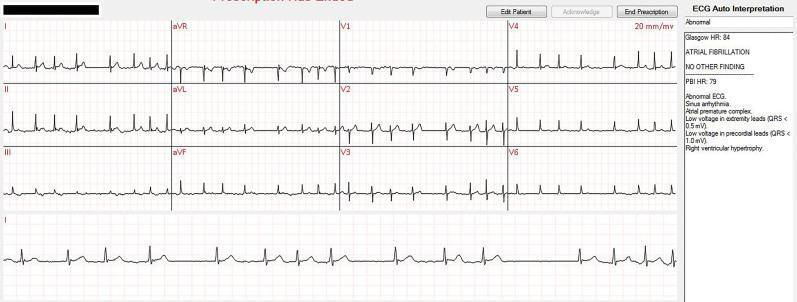
| Feature | Finding |
|---|---|
| P waves | Absent — fibrillatory baseline |
| Rhythm | Irregularly irregular |
| Ventricular rate | Rapid (>100 bpm = rapid ventricular response) |
Kaise pehchano: No P waves + totally irregular RR intervals = AF. Fibrillatory waves at 350–600/min.
Treatment (ICU/Emergency):
- If hemodynamically unstable → DC cardioversion (synchronized, 200J biphasic)
- If stable → Rate control: Metoprolol IV or Diltiazem IV or Digoxin
- Anticoagulation: Heparin → NOAC (Rivaroxaban/Apixaban) or Warfarin
- Treat precipitating cause: sepsis, thyrotoxicosis, PE, post-surgery
CASE 9 — Acute Pulmonary Embolism (S1Q3T3)
Clinical scenario: 40F, sudden dyspnea, pleuritic chest pain, post-surgery (DVT risk)
ECG:

| Feature | Finding |
|---|---|
| Lead I | Deep S wave (S1) |
| Lead III | Q wave + T wave inversion (Q3T3) |
| V1–V4 | T wave inversions (RV strain) |
| Rate | Sinus tachycardia |
| QRS | Incomplete RBBB pattern |
Kaise pehchano: S1Q3T3 = classic PE sign. Sinus tachycardia is the most common ECG finding in PE.
Treatment:
- Massive PE: Alteplase (systemic thrombolysis) 100 mg IV over 2h + UFH
- Submassive PE: UFH anticoagulation ± catheter-directed thrombolysis
- Anticoagulation: LMWH or NOAC for stable PE
- O₂, hemodynamic support, ICU monitoring
CASE 10 — PE with RBBB Pattern
ECG:
| Feature | Finding |
|---|---|
| S1Q3T3 | Present |
| RBBB | rSR' in V1–V2 (right bundle branch block) |
| T inversions | V1–V4 |
| Axis | Right axis deviation |
Treatment: Same as Case 9 — severity determines treatment intensity.
CASE 11 — PE (Sinus Tachycardia + S1Q3T3)
ECG:
Remember: ECG alone cannot rule out PE. Always combine with D-Dimer, CTPA, Wells score.
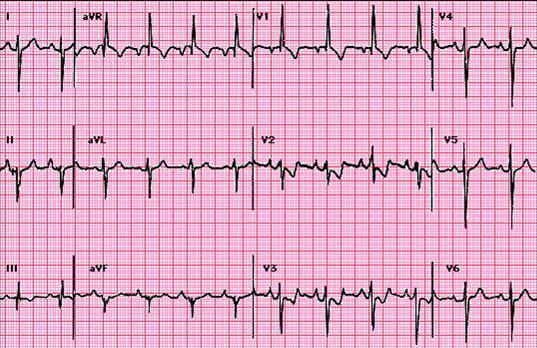
CASE 12 — Wolff-Parkinson-White (WPW) Syndrome
Clinical scenario: 25M, episodes of sudden palpitations, near-syncope
ECG:
| Feature | Finding |
|---|---|
| PR interval | SHORT (<120 ms) |
| QRS | WIDE (>120 ms) |
| Delta wave | Slurred upstroke of QRS (most visible V3–V6) |
| ST-T changes | Secondary repolarization changes |
Kaise pehchano: Short PR + Wide QRS + Delta wave = WPW triad. Bundle of Kent bypasses AV node.
Treatment:
- Symptomatic/SVT → Adenosine (if orthodromic), Procainamide
- ⚠️ NEVER give Digoxin, Verapamil, Adenosine in AF+WPW (can cause VF!)
- Radiofrequency catheter ablation — definitive cure
- Risk stratify with electrophysiology study
CASE 13 — WPW (Mid-Septal Pathway)
ECG:
Pathway localization:
- Negative delta in III + positive V4–V6 → mid-septal
- V1 positive delta → left lateral pathway
- V1 negative delta → right-sided pathway
CASE 14 — WPW + PACs (Pediatric Cardiomyopathy)
ECG:

Note: Delta waves + irregular baseline (PACs) + wide QRS. T inversions across multiple leads suggest secondary cardiomyopathy from incessant tachycardia.
CASE 15 — WPW (Right Midseptal Pathway)
ECG:
PR = 112 ms, QRS = 122 ms. Delta waves in I, II, aVL, aVF, V4–V6. R/S transition V4–V5 → right midseptal pathway.
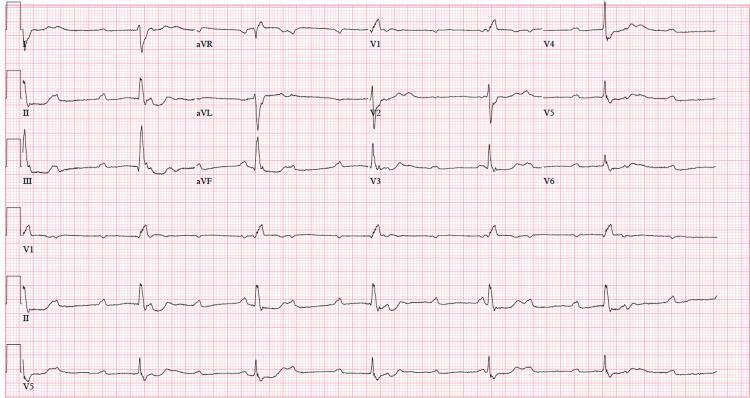
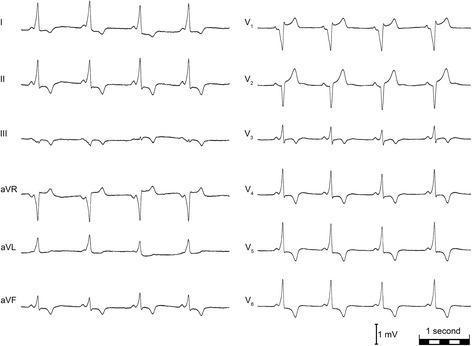
CASE 16 — Left Anterior Fascicular Block (LAFB)
Clinical scenario: 67M, preoperative ECG, no symptoms
ECG:
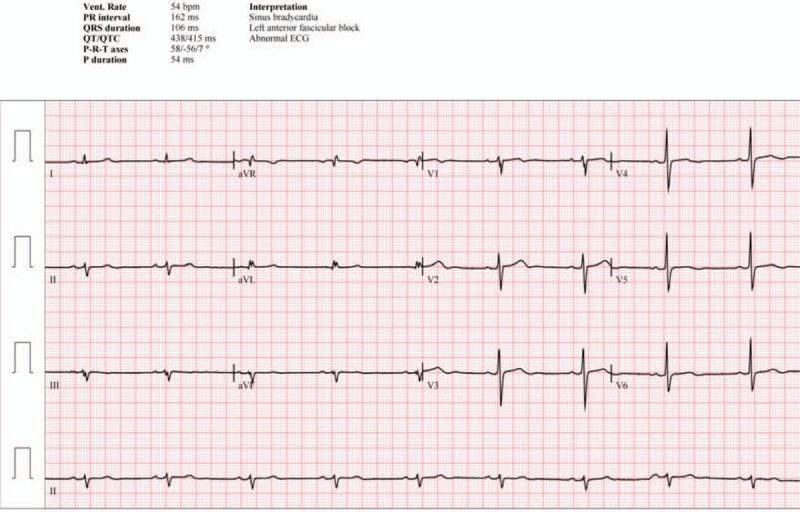
| Feature | Finding |
|---|---|
| Heart rate | 54 bpm (sinus bradycardia) |
| PR interval | 162 ms |
| QRS | 106 ms |
| Axis | Left axis deviation −56° |
| Lead I/aVL | Small q, tall R (qR pattern) |
| Lead II/III/aVF | Small r, deep S (rS pattern) |
Kaise pehchano: Left axis deviation more negative than −45° + rS in inferior leads + qR in I, aVL + no other cause = LAFB.
Treatment: LAFB alone is benign if no structural heart disease. Investigate for CAD, cardiomyopathy.
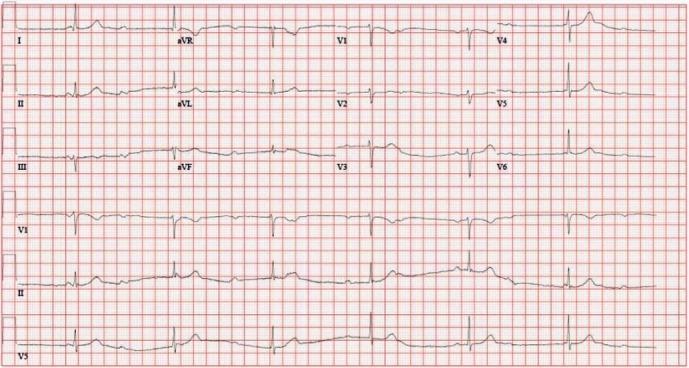
CASE 17 — Diffuse T Wave Inversions / Global Hypokinesis
ECG:
| Feature | Finding |
|---|---|
| T waves | Diffuse inversions I, aVL, V1–V6 |
| ST | Minimal deviation |
| Differential | Ischemia, cardiomyopathy, electrolyte imbalance |
Causes: Global ischemia, Takotsubo cardiomyopathy, severe LV dysfunction, hypokalemia, head injury (neurogenic).
Treatment: Echo urgently, troponin, electrolytes. Treat underlying cause.
CASE 18 — Ventricular Tachycardia (VT)
ECG features (classic VT):
| Feature | Description |
|---|---|
| Rate | 100–250 bpm |
| QRS | Wide (>120 ms), bizarre morphology |
| AV dissociation | P waves march independent of QRS |
| Fusion beats | QRS morphology changes briefly (pathognomonic) |
| Capture beats | Normal narrow complex amidst VT |
Kaise pehchano: Wide complex tachycardia + AV dissociation = VT until proven otherwise (use Brugada criteria).
Treatment:
- Unstable → Synchronized DC cardioversion 200J immediately
- Stable → Amiodarone 150 mg IV bolus, then 1 mg/min infusion
- Lidocaine 1–1.5 mg/kg IV (second line)
- Correct K⁺, Mg²⁺ levels
- ICD implantation if recurrent/structural heart disease
CASE 19 — Torsades de Pointes (Polymorphic VT)
ECG features:
| Feature | Description |
|---|---|
| Rhythm | Irregular wide-complex VT |
| Morphology | QRS axis twists around baseline (spindle pattern) |
| Preceding ECG | Prolonged QTc (>500 ms) |
| Triggers | Bradycardia, hypokalemia, drugs |
Kaise pehchano: "Twisting of points" — QRS complexes cyclically flip above/below baseline.
Causes: Hypokalemia, hypomagnesemia, QT-prolonging drugs (Amiodarone, Haloperidol, Methadone, antibiotics like Azithromycin, Moxifloxacin), congenital Long QT syndrome.
Treatment:
- ⚠️ IV Magnesium sulphate 2g over 5 min — FIRST LINE
- Temporary pacing (overdrive pacing at 90–100 bpm)
- Isoproterenol infusion (pause-dependent TdP)
- STOP QT-prolonging drugs
- Correct K⁺ (target >4.5 mEq/L)
- Defibrillation if degenerated to VF
CASE 20 — Ventricular Fibrillation (VF)
ECG features:
| Feature | Description |
|---|---|
| Rhythm | Chaotic, irregular |
| QRS/T | Not identifiable — only fibrillatory waves |
| Rate | 150–500/min (baseline undulation) |
| Clinical | Pulseless arrest |
Treatment:
- 🚨 CPR immediately
- Defibrillation: 200J biphasic (unsynchronized) — shock first
- Adrenaline 1 mg IV every 3–5 min
- Amiodarone 300 mg IV after 3rd shock
- Identify reversible causes: 4H + 4T (Hypoxia, Hypovolemia, Hypothermia, H⁺/acidosis; Tension pneumo, Tamponade, Toxins, Thrombosis)
🟡 OPD CASES (Cases 21–40)
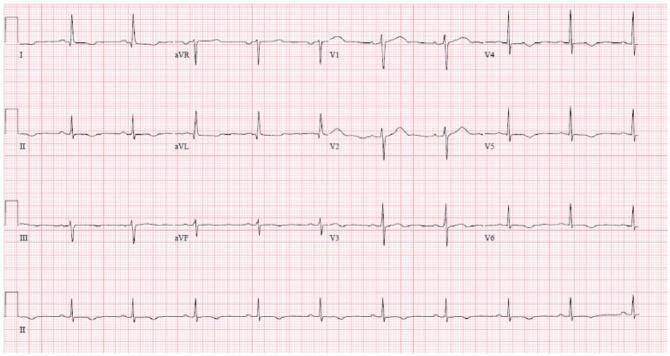
CASE 21 — Normal Sinus Rhythm
ECG:
| Feature | Normal Values |
|---|---|
| Rate | 60–100 bpm |
| P waves | Upright in II, inverted in aVR; before every QRS |
| PR interval | 120–200 ms |
| QRS | <120 ms, narrow |
| R-wave progression | Increases V1→V6 |
| T waves | Upright in I, II, V3–V6 |
Remember: aVR mein sab kuch ulta hoga (P, QRS, T — all negative normally).
CASE 22 — Sinus Bradycardia
ECG features:
| Feature | Finding |
|---|---|
| Rate | <60 bpm |
| P wave | Normal morphology, precedes QRS |
| Rhythm | Regular |
| PR interval | Normal |
Causes (OPD): Athletes (physiological), hypothyroidism, vasovagal, beta-blockers, digoxin toxicity, inferior MI.
Treatment:
- Asymptomatic → No treatment, monitor
- Symptomatic → Atropine 0.5–1 mg IV
- Beta-blocker/digoxin dose reduction
- Pacemaker if irreversible + symptomatic
CASE 23 — Sinus Tachycardia
ECG features:
| Feature | Finding |
|---|---|
| Rate | >100 bpm |
| P waves | Present before each QRS |
| Onset | Gradual (unlike paroxysmal SVT) |
Causes (OPD): Fever, anemia, anxiety, hyperthyroidism, dehydration, pain, PE, heart failure, pregnancy.
Treatment: Treat the CAUSE — not the tachycardia itself!
CASE 24 — First Degree AV Block
ECG features:
| Feature | Finding |
|---|---|
| PR interval | >200 ms (>5 small squares) |
| Conduction | All P waves conduct (every P → QRS) |
| QRS | Normal |
Causes: Vagal tone, inferior MI, rheumatic fever, digoxin, beta-blockers, hypothyroidism, Lyme disease.
Treatment: Usually benign, no treatment. Stop offending drugs if symptomatic. Monitor for progression.
CASE 25 — Second Degree AV Block Type I (Wenckebach / Mobitz I)
ECG features:
| Feature | Finding |
|---|---|
| PR interval | Progressively lengthens |
| QRS drop | Occurs after longest PR |
| Grouped beating | RR intervals get shorter before drop |
Kaise pehchano: "Longer, longer, longer, DROP — then you have a Wenckebach block!"
Causes: Inferior MI, increased vagal tone, digoxin, athletes.
Treatment: Usually benign, often reversible. Monitor, treat cause.
CASE 26 — Second Degree AV Block Type II (Mobitz II)
ECG features:
| Feature | Finding |
|---|---|
| PR interval | FIXED (no lengthening) |
| QRS drop | Sudden, unexpected |
| QRS | Often wide (infranodal disease) |
Kaise pehchano: PR fixed → sudden non-conducted P wave = Mobitz II. More dangerous than Mobitz I!
Treatment: Pacemaker often required — risk of progressing to complete block. Avoid AV nodal blocking drugs.
CASE 27 — Right Bundle Branch Block (RBBB)
ECG features:
| Feature | Finding |
|---|---|
| QRS duration | ≥120 ms |
| V1 | RSR' ("rabbit ears" / M-shaped) |
| V6, I | Wide S wave |
| T waves | Inverted V1–V3 (secondary changes) |
Kaise pehchano: "RsR' in V1 with wide S in V5/V6" = RBBB. Right bunny ears!
Causes: PE, ASD, RV strain, ischemia, age-related, post-cardiac surgery.
Treatment: Isolated RBBB — no treatment. Investigate cause. New RBBB in setting of chest pain = ischemia.
CASE 28 — Left Bundle Branch Block (LBBB)
ECG features:
| Feature | Finding |
|---|---|
| QRS | ≥120 ms |
| V5/V6, I, aVL | Broad notched R wave (M-shaped) |
| V1 | Deep QS or rS pattern |
| Concordance | ST/T always opposite QRS direction |
Kaise pehchano: "WiLLiaM" — W in V1, M in V5 = LBBB. Sgarbossa criteria for STEMI in LBBB.
Sgarbossa Criteria for MI in LBBB:
- ST elevation ≥1 mm concordant with QRS (+5 points)
- ST depression ≥1 mm in V1–V3 (+3 points)
- ST elevation ≥5 mm discordant (+2 points) Score ≥3 = STEMI
Treatment: New LBBB with chest pain = treat as STEMI!
CASE 29 — Left Ventricular Hypertrophy (LVH)
ECG features:
| Feature | Finding |
|---|---|
| Sokolow-Lyon | S(V1) + R(V5 or V6) ≥35 mm |
| Cornell | R(aVL) + S(V3) ≥28mm (M) / ≥20mm (F) |
| Strain pattern | ST depression + T inversion in I, aVL, V5, V6 |
Causes: Hypertension (#1), aortic stenosis, HCM, coarctation.
Treatment: Treat hypertension (ACE inhibitor/ARB preferred — cause LVH regression). Treat valvular disease.
CASE 30 — Right Ventricular Hypertrophy (RVH)
ECG features:
| Feature | Finding |
|---|---|
| Dominant R in V1 | R > S in V1 (R ≥7 mm) |
| S in V5/V6 | Persistent deep S |
| Axis | Right axis deviation (>+90°) |
| Strain | T inversion V1–V3 |
Causes: Pulmonary hypertension, mitral stenosis, COPD, ASD, VSD.
Treatment: Treat underlying cause (pulmonary hypertension: Sildenafil, Bosentan, prostacyclins).
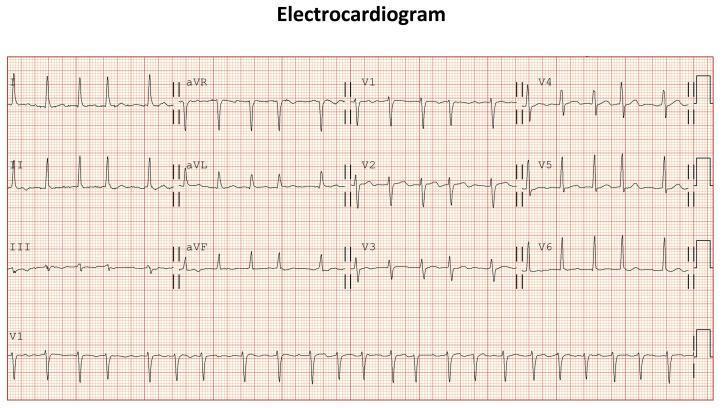
CASE 31 — Atrial Flutter
ECG features:
| Feature | Finding |
|---|---|
| Flutter waves | Sawtooth pattern in II, III, aVF |
| Atrial rate | ~300 bpm |
| AV conduction | Usually 2:1 → ventricular rate ~150 bpm |
| QRS | Narrow (if no aberrant conduction) |
Kaise pehchano: Regular rate of 150 bpm + sawtooth baseline = flutter until proven otherwise!
Treatment:
- Rate control: Beta-blocker, Diltiazem, Digoxin
- DC cardioversion: Low energy 50–100J biphasic (converts easily)
- Anticoagulation same as AF
- Radiofrequency ablation — curative (cavotricuspid isthmus ablation)
CASE 32 — SVT (Paroxysmal Supraventricular Tachycardia)
ECG features:
| Feature | Finding |
|---|---|
| Rate | 150–250 bpm |
| QRS | Narrow (usually) |
| P waves | Not visible or buried in QRS |
| Onset | Sudden ("paroxysmal") |
Types: AVNRT (most common), AVRT (WPW), atrial tachycardia.
Treatment:
- Vagal maneuvers (Valsalva, carotid sinus massage)
- Adenosine 6 mg rapid IV push (second dose 12 mg)
- Verapamil 5–10 mg IV (if no pre-excitation)
- DC cardioversion if unstable
- Long-term: Catheter ablation (curative >95%)
CASE 33 — Premature Ventricular Complexes (PVCs)
ECG features:
| Feature | Finding |
|---|---|
| QRS | Wide, bizarre, early |
| No P wave | Before premature beat |
| Compensatory pause | Full compensatory pause after PVC |
| T wave | Opposite direction to QRS |
Bigeminy = every other beat is PVC. Trigeminy = every 3rd beat.
Causes: Electrolyte imbalance, ischemia, stimulants (caffeine), anxiety, LV dysfunction.
Treatment:
- Benign PVCs, no structural heart disease → reassurance
- Frequent PVCs + symptoms → Beta-blocker, Flecainide
- PVC-induced cardiomyopathy (burden >20%) → ablation
- Correct K⁺, Mg²⁺
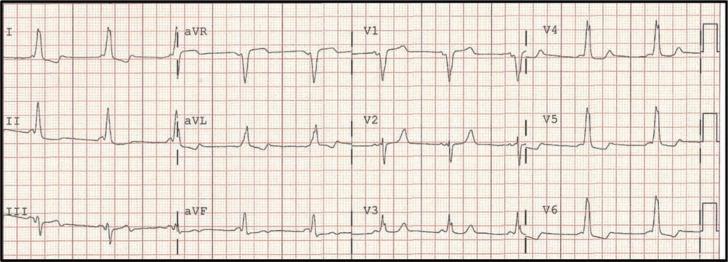
CASE 34 — Hyperkalemia (Peaked T waves → Sine Wave)
ECG progression with rising K⁺:
| K⁺ Level | ECG Change |
|---|---|
| 5.5–6.0 | Peaked, narrow, symmetric T waves (tent-like) |
| 6.0–7.0 | PR prolongation, P wave flattening |
| 7.0–8.0 | P wave disappears, wide QRS |
| >8.0 | Sine wave pattern → VF |
Kaise pehchano: Narrow-based, tall, symmetric T waves (like a tent) = hyperkalemia. V4 mein sabse prominent.
Treatment (ICU Emergency):
- IV Calcium gluconate 10 mL 10% — membrane stabilization (immediate)
- Sodium bicarbonate — shift K into cells
- Insulin 10U + Dextrose 50% — shift K into cells (most reliable)
- Salbutamol nebulization — K shift
- Kayexalate / Patiromer — GI elimination
- Dialysis — definitive if renal failure
CASE 35 — Hypokalemia
ECG features:
| K⁺ Level | ECG Change |
|---|---|
| 3.0–3.5 | T wave flattening |
| <3.0 | Prominent U waves (after T wave) |
| <2.5 | ST depression, T-U fusion |
| Severe | Torsades de Pointes risk! |
Kaise pehchano: U wave (small positive deflection after T wave, best seen in V2–V3) = hypokalemia.
Treatment:
- Mild (3.0–3.5): Oral KCl 40–80 mEq/day
- Severe (<3.0) or TdP risk: IV KCl (max 20 mEq/hr via central line)
- Replace Mg²⁺ simultaneously (hypomagnesemia causes refractory hypokalemia)
CASE 36 — Pericarditis
ECG features:
| Feature | Finding |
|---|---|
| ST elevation | Diffuse (I, II, aVL, aVF, V2–V6) — concave/saddle-shaped |
| PR depression | PR segment depressed (early finding) |
| Reciprocal changes | Absent (unlike MI) |
| Evolution | ST returns to normal, then T inversion |
Kaise pehchano: Diffuse ST elevation (multiple territories) + concave shape + PR depression = pericarditis. Unlike STEMI which is convex (domed) and territory-specific.
Treatment:
- Colchicine 0.5 mg BD (first-line, prevents recurrence)
- Ibuprofen 600 mg TDS or Aspirin 750 mg TDS
- Avoid steroids (increases recurrence)
- Restrict exercise for 3–6 months
CASE 37 — Hypothermia (Osborn/J Waves)
ECG features:
| Feature | Finding |
|---|---|
| J waves (Osborn waves) | Positive deflection at J-point, V2–V5 |
| Bradycardia | Sinus bradycardia |
| Artifact | Muscle tremor artifact (shivering) |
| Severe | Junctional rhythm, AF, VF risk |
Kaise pehchano: Patient cold (core temp <32°C) + J-waves (notch after QRS, before ST) = hypothermia.
Treatment:
- Passive rewarming (mild: >32°C)
- Active external warming (moderate: 28–32°C)
- Active internal warming: warm IV fluids, bladder/gastric lavage (severe: <28°C)
- ECMO for cardiac arrest + hypothermia
CASE 38 — Digoxin Toxicity
ECG features:
| Feature | Finding |
|---|---|
| ST-T changes | Scooped/shovelled ST depression (reverse tick sign) |
| PR prolongation | AV block (1st, 2nd, 3rd) |
| Arrhythmias | PVCs (bigeminy), VT, atrial tachycardia with AV block |
| Rate | Bradycardia or tachycardia |
Kaise pehchano: "Scooping" of ST segment (looks like the bottom of a shoe) + AV block + increased QRS + arrhythmias = digoxin effect/toxicity.
Treatment:
- Stop digoxin
- Digibind (Digoxin-specific antibody fragments) — definitive antidote
- Correct hypokalemia, hypomagnesemia (potentiate toxicity)
- Atropine for bradycardia; Lidocaine/Phenytoin for VT
- Avoid cardioversion in digoxin toxicity (causes VF)
CASE 39 — Brugada Syndrome
ECG features (Type 1 — diagnostic):
| Feature | Finding |
|---|---|
| ST elevation | Coved (downsloping) in V1–V2, ≥2 mm |
| T wave | Inverted in V1–V2 |
| Axis | Normal or right |
| QRS | Slight widening |
Type 2: Saddle-back pattern (less diagnostic). Unmasked by fever, sodium channel blockers, flecainide challenge.
Kaise pehchano: "Coved" ST elevation in V1–V2 in right precordial leads = Brugada pattern. Danger: SCD risk!
Treatment:
- ICD (implantable cardioverter-defibrillator) — only proven treatment
- Quinidine (reduces VF storms)
- ⚠️ Avoid: Sodium channel blockers (Flecainide, Propafenone), Tricyclic antidepressants, fever
CASE 40 — Long QT Syndrome (LQTS)
ECG features:
| Feature | Finding |
|---|---|
| QTc | Prolonged: >450 ms (male), >460 ms (female) |
| T wave morphology | Broad, notched, biphasic |
| Risk | Torsades de Pointes → VF → sudden death |
QTc calculation: QT ÷ √(RR interval in seconds) — Bazett formula
Causes:
- Congenital: LQT1, LQT2, LQT3 (ion channel mutations)
- Acquired: Hypokalemia, hypomagnesemia, drugs (Amiodarone, Haloperidol, Azithromycin, Moxifloxacin, Methadone, Chloroquine)
Treatment:
- Remove QT-prolonging drugs
- Beta-blockers (LQT1/LQT2) — Propranolol/Nadolol
- ICD if symptomatic or LQTS3
- Mexiletine (LQT3)
- IV Magnesium if TdP develops
📊 QUICK REFERENCE TABLE — All 40 Cases
| # | Condition | Key ECG Finding | Urgent Treatment |
|---|---|---|---|
| 1 | Anterior STEMI | ST ↑ V1–V6 tombstone | PCI/Thrombolysis |
| 2 | Inferior STEMI | ST ↑ II, III, aVF | PCI, no nitrates if RV |
| 3 | Inferior STEMI + AF | Irregular + inferior ST↑ | PCI + anticoag |
| 4 | NSTEMI | T inversion V5–V6, ST↓ | DAPT, angiogram |
| 5 | CHB wide QRS | AV dissociation, wide escape | Temp pacing → PPM |
| 6 | CHB narrow QRS | AV dissociation, narrow escape | Atropine → PPM |
| 7 | CHB ventricular escape | Wide notched escape | Emergency pacing |
| 8 | AF rapid response | Irregular, no P waves, fast | Cardioversion/rate control |
| 9 | PE (S1Q3T3) | S₁Q₃T₃, sinus tachy | Thrombolysis/LMWH |
| 10 | PE + RBBB | S1Q3T3 + rSR' V1 | Anticoagulation |
| 11 | PE sinus tachy | Sinus tach + S1Q3T3 | CTPA, anticoag |
| 12 | WPW | Short PR, delta wave | Ablation, avoid digoxin |
| 13 | WPW mid-septal | Delta wave localization | Ablation |
| 14 | WPW + PACs | Delta wave + ectopics | Ablation |
| 15 | WPW right septal | Delta V4–V6, short PR | Ablation |
| 16 | LAFB | LAD, qR in I/aVL, rS inf | Investigate CAD |
| 17 | Diffuse T inversions | T↓ across leads | Echo, troponin |
| 18 | VT | Wide QRS tachy, AV dissoc | Cardioversion/Amiodarone |
| 19 | Torsades de Pointes | Twisting QRS, long QT | IV MgSO₄, stop drugs |
| 20 | VF | Chaotic baseline | CPR + Defibrillation |
| 21 | Normal sinus | All normal | Reassure |
| 22 | Sinus bradycardia | Rate <60, normal P | Treat cause, Atropine |
| 23 | Sinus tachycardia | Rate >100, normal P | Treat cause |
| 24 | 1st degree AVB | PR >200ms | Monitor |
| 25 | Mobitz I (Wenckebach) | PR lengthens then drop | Monitor, treat cause |
| 26 | Mobitz II | Fixed PR, sudden drop | Pacemaker |
| 27 | RBBB | RSR' V1, wide S V6 | Investigate cause |
| 28 | LBBB | WiLLiaM pattern | New = treat as STEMI |
| 29 | LVH | Sokolow ≥35mm, strain | Treat HTN (ACEi/ARB) |
| 30 | RVH | Dominant R V1, RAD | Treat pulm HTN |
| 31 | Atrial flutter | Sawtooth 300bpm, 2:1 | Cardioversion/ablation |
| 32 | SVT/AVNRT | Narrow tachy 150–250 | Adenosine, ablation |
| 33 | PVCs | Wide early beats, comp pause | Beta-blocker/ablation |
| 34 | Hyperkalemia | Peaked T → sine wave | Ca²⁺, Insulin-dextrose |
| 35 | Hypokalemia | Flat T, U waves | K replacement |
| 36 | Pericarditis | Saddle ST↑ all leads, PR↓ | Colchicine + NSAID |
| 37 | Hypothermia | J/Osborn waves, bradycardia | Rewarming |
| 38 | Digoxin toxicity | Scooped ST, AV block | Digibind |
| 39 | Brugada | Coved ST V1–V2 | ICD, avoid Na-blockers |
| 40 | Long QT | QTc >450–460 ms | Stop drugs, BB, ICD |
🔑 KEY RULES FOR ECG READING
"See Wide → Think VT first" — Wide complex tachycardia = VT until proven otherwise
"See Irregular → Think AF" — Totally irregular rhythm with no P waves = AF
"See Short PR + Wide QRS → WPW" — Don't give Digoxin or Verapamil!
"See Tombstone → Cath Lab NOW" — No time to waste in STEMI
"See S1Q3T3 + Tachycardia → Think PE" — Especially post-op or immobile patient
"See Peaked T → Check K⁺" — Hyperkalemia kills silently
"See PR Depression + Diffuse ST↑ → Pericarditis" — NOT infarction
"See J-wave + Cold Patient → Hypothermia" — Rewarm before pronouncing dead
This is a shared conversation. Sign in to Orris to start your own chat.