I am doing a seminar based on the main topic "Pyrexia of Unknown Origin", in which I am supposed to focus on meningitis for my part. Give me details on what meningitis is, its epidemiology, aetiology, pathophysiology, clinical manifestations, investigations with expected outcomes, and detailed management plan according to latest guidelines followed by Malaysia and Internal Medicine textbooks.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
bacterial meningitis CSF findings cerebrospinal fluid analysis
Here is your comprehensive seminar resource on Meningitis within the context of Pyrexia of Unknown Origin, drawn from Goldman-Cecil Medicine, Rosen's Emergency Medicine, Robbins & Kumar Pathology, and Textbook of Family Medicine.
Meningitis — Seminar Notes
Context: Pyrexia of Unknown Origin
1. DEFINITION
Meningitis is an inflammatory process involving the leptomeninges (arachnoid and pia mater) within the subarachnoid space. If infection extends into the underlying brain parenchyma, it is termed meningoencephalitis. The inflammatory process extends throughout the subarachnoid space and involves the ventricles.
Classification:
- Acute pyogenic (usually bacterial) — polymorphonuclear (neutrophilic) CSF response
- Aseptic (usually viral) — lymphocytic CSF response
- Chronic (tuberculous, fungal, spirochetal) — subacute, developing over weeks to months
Non-infectious causes include chemical meningitis (e.g., ruptured epidermoid cyst) and carcinomatous meningitis (malignant subarachnoid spread).
2. EPIDEMIOLOGY
Global Burden
- Incidence of bacterial meningitis in developed countries: 0.5–1.5 per 100,000 adults — dramatically reduced by vaccination
- Despite diagnostic advances, mortality remains ~15%; survivors carry significant neurological sequelae (highest in pneumococcal meningitis)
- Post-Hib vaccine era: S. pneumoniae now accounts for ~70% of adult bacterial meningitis; disease has shifted toward older adults
- Viral meningitis is now the most common overall form owing to the decline in bacterial disease
Meningococcal Epidemiology
- N. meningitidis predominates in children and young adults in close-contact settings (dormitories, military barracks)
- Serogroup distribution: Group B — Europe; Group C — USA; Group A — sub-Saharan Africa (meningitis belt)
- Malaysian relevance: Meningococcal vaccine (MenACWY) is mandatory for Hajj/Umrah pilgrims per Ministry of Health Malaysia
Malaysian Context
Malaysia follows IDSA and WHO guidelines, supplemented by the Malaysian Ministry of Health Clinical Practice Guidelines (CPGs). The national immunisation programme includes PCV-13, Hib (pentavalent vaccine), and meningococcal vaccines for high-risk groups.
3. AETIOLOGY
By Age Group
| Age | Common Pathogens |
|---|---|
| 0–1 month | Group B Streptococcus, E. coli, L. monocytogenes, S. pneumoniae |
| 1–3 months | Group B Strep, L. monocytogenes, S. pneumoniae, N. meningitidis, H. influenzae, E. coli |
| 3 months–18 years | S. pneumoniae, N. meningitidis, H. influenzae |
| 18–50 years | S. pneumoniae, N. meningitidis |
| >50 years | S. pneumoniae, L. monocytogenes, gram-negative bacilli |
| Post-neurosurgery/trauma | Coagulase-negative Staphylococci, S. aureus, Cutibacterium acnes, Pseudomonas aeruginosa |
Viral Causes (Aseptic Meningitis)
- Enteroviruses (Enterovirus B species) — dominant; account for ~50% of all meningitis/encephalitis; fever, headache, meningism; usually self-limiting
- Herpesviruses: HSV-1/2, VZV, CMV, EBV
- HIV (acute seroconversion)
- Arboviruses: Japanese Encephalitis Virus — endemic in Southeast Asia including Malaysia
- Mumps — in unvaccinated populations
Fungal (Immunocompromised)
- Cryptococcus neoformans — HIV/AIDS, organ transplant; subacute presentation
- Candida, Histoplasma, Coccidioides — less common
Chronic / TB
- Mycobacterium tuberculosis — highly relevant in Malaysia (high TB burden); subacute/chronic onset; basal meningitis
- Treponema pallidum (neurosyphilis)
- Borrelia burgdorferi (Lyme — also causes facial palsy, radiculopathy)
Predisposing Risk Factors
- Otitis media (most common)
- Sinusitis, mastoiditis, CSF leak (post-traumatic/surgical)
- Alcoholism, asplenia, immunocompromised state
- Unvaccinated status
- Close-contact settings; pilgrims (Hajj/Umrah)
- Dural breach (neurosurgery, lumbar puncture)
4. PATHOPHYSIOLOGY
Step 1 — Nasopharyngeal Colonisation & Mucosal Invasion
Bacterial meningitis typically begins with colonisation of the nasopharynx. Organisms penetrate the respiratory mucosa aided by IgA proteases and antiphagocytic capsular polysaccharides.
Step 2 — Bacteraemia & BBB Penetration
Bacteria enter the bloodstream and cross the blood-brain barrier (BBB) via:
- Transcytosis through cerebral capillary endothelial cells
- Infected monocytes ("Trojan horse")
- Choroid plexus epithelium
Step 3 — Subarachnoid Proliferation
The CSF is an immunologically poor environment — low Ig levels, minimal complement activity, and virtually no phagocytes in normal CSF. Bacteria proliferate rapidly once they cross the BBB.
Step 4 — Inflammatory Cascade
Bacterial cell wall components (LPS, teichoic acid, peptidoglycan) trigger release of TNF-α, IL-1β, IL-6 → neutrophilic recruitment → pleocytosis:
| Consequence | Mechanism |
|---|---|
| Vasogenic oedema | ↑ BBB permeability |
| Cytotoxic oedema | Cerebral vasculitis → ischaemia |
| Interstitial oedema | Impaired CSF reabsorption |
| ↑ Intracranial pressure | All three oedema types combined |
| ↓ Cerebral blood flow | → Cerebral hypoxia and infarction |
| Venous sinus thrombosis | ~1% of cases → seizures, focal deficits |
Step 5 — Systemic Complications
- Waterhouse-Friderichsen syndrome (meningococcal): bilateral adrenal haemorrhage + DIC + purpura fulminans
- Endotoxic shock → cardiovascular collapse in fulminant disease
- SIADH → hyponatraemia
5. CLINICAL MANIFESTATIONS
Classic Triad
Fever + Severe Headache + Neck Stiffness — present in ~85% of adults
Key Signs & Symptoms
| Feature | Frequency |
|---|---|
| Classic triad (all three) | ~44% |
| Headache (severe, often needing opioids) | Near universal |
| Photophobia | >66% |
| Nausea/vomiting | ~35% |
| Seizures | ~30% adults; 40% neonates |
| Altered consciousness (confusion → coma) | Common |
| Cranial nerve palsies | 10–20% |
| Petechial/purpuric rash | Suggests N. meningitidis |
| Papilledema | <1% early — if present, consider abscess/mass |
Meningeal Signs
- Kernig's sign: Inability to fully extend the knee when hip is flexed to 90°
- Brudzinski's sign: Passive neck flexion causes involuntary hip/knee flexion
- Sensitivity <12% (low) but high specificity — presence strongly confirms meningitis
- Unreliable in infants <1 year
Age-Specific Presentations
| Age | Distinctive Features |
|---|---|
| Neonates | Poor feeding, irritability, temperature instability, apnoea, seizures (40%), bulging fontanelle (late) |
| Children <1 yr | Meningismus unreliable; maculopapular → petechial rash (meningococcal) |
| Adults | Classic triad; severe headache relieved temporarily by LP |
| Elderly (>65 yr) | Insidious, variable meningeal signs, confusion/obtundation; fever may be absent |
| Immunocompromised | Atypical, subtle presentations |
Meningococcal-Specific
- Petechial/purpuric rash on extremities (anywhere)
- Rapid progression → endotoxic shock, DIC
- Waterhouse-Friderichsen syndrome: bilateral adrenal haemorrhage
TB Meningitis (Subacute–Chronic)
- Cranial nerve palsies (CN VI most common, then CN III)
- Symptoms over weeks to months
- Basal meningitis pattern; CSF with markedly low glucose
6. INVESTIGATIONS & EXPECTED OUTCOMES
A. Pre-LP Assessment
Before LP, always check for signs of raised ICP:
- Bedside optic nerve sheath USS: diameter >5 mm → raised ICP
- If any of the following → CT brain first:
- Papilledema
- New seizures / focal neurological deficit
- Altered GCS
- Signs of mass lesion
⚠️ Never delay empirical antibiotics pending CT/LP if high clinical suspicion exists. CSF can be sterilised within 1 hour of antibiotics, so LP should be as expeditious as possible.
B. CSF Analysis — Expected Findings
| Parameter | Normal | Bacterial | Viral | TB / Fungal |
|---|---|---|---|---|
| Opening pressure | <20 cmH₂O | ↑↑ >30 | N or ↑ | ↑ |
| Appearance | Clear | Turbid/purulent | Clear | Clear or turbid |
| WBC (cells/μL) | <5 | 100–50,000 (neutrophils) | 10–1,000 (lymphocytes) | 100–500 (lymphocytes) |
| Protein | 15–45 mg/dL | ↑↑ (100–500+) | N or mildly ↑ | ↑ |
| Glucose | ≥60% serum | ↓↓ (<45; ratio <0.4) | Normal | ↓ |
| Gram stain | — | +ve 60–90% (untreated) | Negative | Negative |
| Culture | Sterile | +ve (gold standard) | Negative | TB culture (slow) |
| Lactate | 0.88–2.7 mmol/L | ↑ (>2.7) | Normal | Variable |
Additional CSF tests:
- PCR (multiplex): H. influenzae (67–100%), S. pneumoniae (79–100%), N. meningitidis (91–100%); sensitivity 70% even after 1 week of antibiotics
- HSV PCR: 96% sensitivity, 99% specificity — avoids need for brain biopsy
- Cryptococcal antigen: gold standard for cryptococcal meningitis (serum + CSF)
- India ink stain: quick but low sensitivity (~30%) for Cryptococcus
- AFB stain/TB culture + adenosine deaminase (ADA): for TB meningitis (AFB sensitivity <60%)
C. Blood Investigations
| Test | Purpose |
|---|---|
| Blood cultures ×2 | Before antibiotics; positive in ~50% bacterial meningitis |
| FBC | Leukocytosis + neutrophilia (bacterial); lymphocytosis (viral) |
| CRP / Procalcitonin | Elevated in bacterial; useful differentiation tool |
| Serum glucose | Required for CSF:serum glucose ratio |
| Electrolytes + renal function | SIADH → hyponatraemia |
| Coagulation (PT, APTT, platelet) | DIC screen (meningococcal) |
| HIV serology | If cryptococcal/TB meningitis suspected |
D. Imaging
CT brain (contrast): before LP if contraindications; shows meningeal enhancement, hydrocephalus, cerebral abscess.
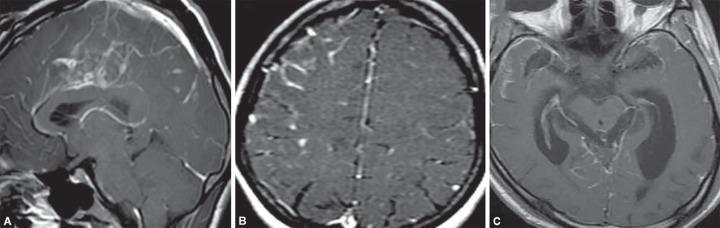
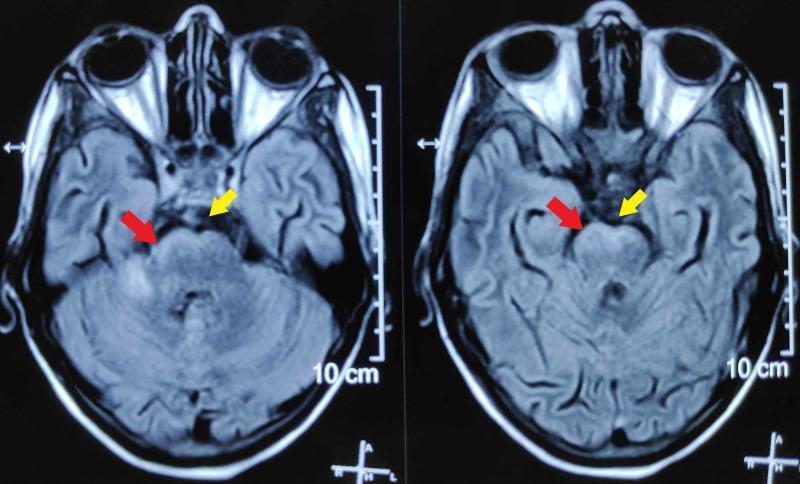
MRI brain with gadolinium (superior):
- Diffuse leptomeningeal/pachymeningeal enhancement along cerebral convexities and basal cisterns
- Basilar cisternal exudates → TB meningitis
- Temporal lobe signal changes → HSV encephalitis
7. MANAGEMENT
A. Immediate Stabilisation (First Hour)
- ABCs: Airway, breathing, circulation; O₂, IV access
- Blood cultures ×2 — before antibiotics, without delaying treatment
- Empirical IV antibiotics IMMEDIATELY
- Dexamethasone IV — first dose given before or with first antibiotic dose
- CT brain only if LP is contraindicated (avoid delaying treatment)
- LP as soon as it is safe
B. Empirical Antibiotic Therapy
(IDSA Guidelines; WHO; Malaysian MOH CPG)
| Patient Group | Likely Organisms | Empirical Regimen |
|---|---|---|
| Neonates (0–4 wk) | S. agalactiae, E. coli, L. monocytogenes | Ampicillin + Cefotaxime |
| Infants & children | S. pneumoniae, N. meningitidis | Ceftriaxone 100 mg/kg/day OR Cefotaxime 75 mg/kg/6h |
| Adults 18–50 yr | S. pneumoniae, N. meningitidis | Ceftriaxone 2g IV q12h ± Vancomycin |
| Adults >50 yr / immunocompromised | + L. monocytogenes, gram-negatives | Ceftriaxone + Ampicillin + Vancomycin |
| Post-surgery / nosocomial | Staphylococci, Pseudomonas | Vancomycin + Cefepime (or Meropenem) |
Add Vancomycin where drug-resistant S. pneumoniae (DRSP) incidence is >2% — relevant in Malaysia.Add Ampicillin 2g IV q4h if Listeria suspected (age >50, alcoholism, immunosuppression).Add Acyclovir 10 mg/kg IV q8h if HSV encephalitis cannot be excluded.
C. Adjunctive Corticosteroids — Grade A Recommendation
Dexamethasone 0.15 mg/kg IV q6h × 4 days
- Start before or with the first antibiotic dose
- Reduces mortality and neurological sequelae (especially sensorineural hearing loss)
- Grade A evidence in:
- Adults with suspected/proven pneumococcal meningitis (IDSA)
- Children with Hib meningitis (IDSA)
⚠️ If S. pneumoniae not confirmed on culture, consider stopping dexamethasone — it may reduce CSF penetration of vancomycin.
D. Targeted Therapy (After Culture/Sensitivity)
| Organism | Drug of Choice | Alternative |
|---|---|---|
| S. pneumoniae (penicillin-sensitive) | Penicillin G 4 MU IV q4h | Ceftriaxone |
| S. pneumoniae (resistant) | Ceftriaxone + Vancomycin | Meropenem |
| N. meningitidis | Penicillin G or Ceftriaxone | Chloramphenicol |
| H. influenzae | Ceftriaxone | Chloramphenicol |
| L. monocytogenes | Ampicillin ± Gentamicin | TMP-SMX |
| E. coli / gram-negatives | Ceftriaxone | Meropenem |
| S. aureus (MRSA) | Vancomycin | Linezolid |
| TB meningitis | RHEZ × 2 months → RH × 7–10 months + Dexamethasone | |
| Cryptococcal meningitis | Amphotericin B (induction) → Fluconazole (consolidation/maintenance) | |
| HSV encephalitis | Acyclovir 10 mg/kg IV q8h × 14–21 days |
E. Supportive Care
- Head of bed elevated 30°, neutral neck position (reduce ICP)
- Maintain euvolaemia (avoid both hypovolaemia and fluid overload)
- Treat SIADH/hyponatraemia (fluid restrict if Na <130 mEq/L)
- Seizure management: benzodiazepines acutely; AEDs in recurrent seizures
- Analgesia (opioids for severe headache), antipyretics (paracetamol)
- Monitor for complications: DIC, septic shock, herniation
F. Raised ICP Management
- Dexamethasone (see above)
- Mannitol 0.25–1 g/kg IV for acute ICP elevation
- Controlled hyperventilation (PaCO₂ 30–35 mmHg) as temporising measure
- EVD (external ventricular drain) if obstructive hydrocephalus develops
G. Chemoprophylaxis (Meningococcal Close Contacts)
Within 7 days of symptom onset for household/intimate contacts:
| Agent | Dose | Notes |
|---|---|---|
| Rifampicin 600 mg PO q12h × 2 days | Adult | First-line |
| Ciprofloxacin 500 mg PO single dose | Non-pregnant adults | Alternative |
| Ceftriaxone 250 mg IM single dose | Pregnant women | Safe in pregnancy |
Also administer meningococcal vaccine to close contacts where applicable.
H. Vaccination (Prevention)
| Vaccine | Target | Malaysian Schedule |
|---|---|---|
| PCV-13 | S. pneumoniae 13 serotypes | Childhood primary series + adults with risk factors |
| Hib (pentavalent) | H. influenzae type b | 2, 3, 5 months + booster |
| MenACWY | N. meningitidis A, C, W, Y | High-risk groups; mandatory for Hajj/Umrah pilgrims |
| MenB | N. meningitidis B | Not in standard NIP; selected high-risk groups |
8. COMPLICATIONS
| Complication | Key Points |
|---|---|
| Sensorineural hearing loss | Most common neurological sequela; dexamethasone reduces risk |
| Epilepsy | Acute seizures and long-term |
| Cerebral infarction/stroke | Vasculitis or venous sinus thrombosis |
| Hydrocephalus | Obstructive; may require EVD or shunting |
| Cerebral herniation | Most immediately fatal complication of raised ICP |
| SIADH/Hyponatraemia | Monitor electrolytes closely |
| DIC | Meningococcemia; check coagulation screen |
| Waterhouse-Friderichsen syndrome | Meningococcal bilateral adrenal haemorrhage |
| Cognitive impairment | Long-term, especially in paediatric cases |
| Death | ~15% overall; up to 27% in Listeria meningitis |
9. MENINGITIS IN THE CONTEXT OF PUO
Meningitis should enter the differential of any PUO when:
- Fever + headache/neck stiffness/altered consciousness — classical presentation
- Subacute fever + cranial nerve palsy → TB meningitis (especially in Malaysia)
- HIV+ patient with unexplained fever and any CNS symptom → cryptococcal meningitis
- Prolonged fever in immunocompromised patient without obvious source → low threshold for LP
- Fever + purpuric rash → meningococcal disease — a medical emergency
Diagnostic differentiation summary:
| Type | Onset | CSF Cells | CSF Glucose | Key Test |
|---|---|---|---|---|
| Bacterial | Acute (hours) | Neutrophils ↑↑ | ↓↓ | Gram stain, culture, PCR |
| Viral | Acute (days) | Lymphocytes | Normal | Viral PCR |
| TB | Subacute (weeks) | Lymphocytes | ↓ (marked) | AFB, ADA, TB PCR |
| Fungal | Subacute–chronic | Lymphocytes | ↓ | CrAg, India ink |
Sources: Goldman-Cecil Medicine 26th Ed. — Bacterial Meningitis; Rosen's Emergency Medicine 9th Ed. — Chapter 95; Robbins & Kumar Basic Pathology 10th Ed. — Chapter 21; Textbook of Family Medicine 9th Ed. — Chapter 41; IDSA Guidelines (Tunkel et al.); Malaysian MOH CPG.
In which step of pathophysiology does Pia-arachnoid membrane get congested and infiltrated with inflammatory cells, and pus forming in layers which eventually organise to form adhesions? Order the steps again and give me the pathophysiology.
Reading File
You've run out of free credits. Sign up for a free account to continue using Orris.
This is a shared conversation. Sign in to Orris to start your own chat.