Everything about Haemorrhoid in detail classification
Reading File
Finding Sources
Finding Sources
Searching Images
haemorrhoid classification degrees internal external
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have comprehensive information from multiple surgical and emergency medicine textbooks. Here is a detailed overview of haemorrhoids:
Haemorrhoids — Comprehensive Overview
1. Definition & Normal Anatomy
Haemorrhoids are specialized vascular cushions in the anal canal composed of blood vessels (arteriovenous anastomoses), connective tissue, and smooth muscle fibres. They are a normal part of human anatomy, contributing 15–20% of anal resting pressure and aiding faecal continence by cushioning the anal canal during defaecation.
Three primary cushion groups exist in the anal canal, located at:
- Right anterior
- Right posterior
- Left lateral
They become pathological when the muscularis submucosa weakens, causing the cushions to engorge, dilate, and prolapse distally.
Haemorrhoids are not varicose veins — they are displaced, engorged anal cushions.
— Current Surgical Therapy 14e; Rosen's Emergency Medicine
2. Classification — By Anatomical Origin
The primary classification depends on origin relative to the dentate (pectinate) line, not where the distal portion lies.
| Type | Origin | Vascular Plexus | Epithelium | Sensation |
|---|---|---|---|---|
| Internal | Above the dentate line | Superior haemorrhoidal plexus | Transitional / columnar mucosa | No somatic pain fibres |
| External | Below the dentate line | Inferior haemorrhoidal plexus | Modified squamous epithelium (anoderm) | Extremely sensitive (somatic) |
| Mixed | At or spanning the dentate line | Both plexuses | Both mucosa and anoderm | Varies |
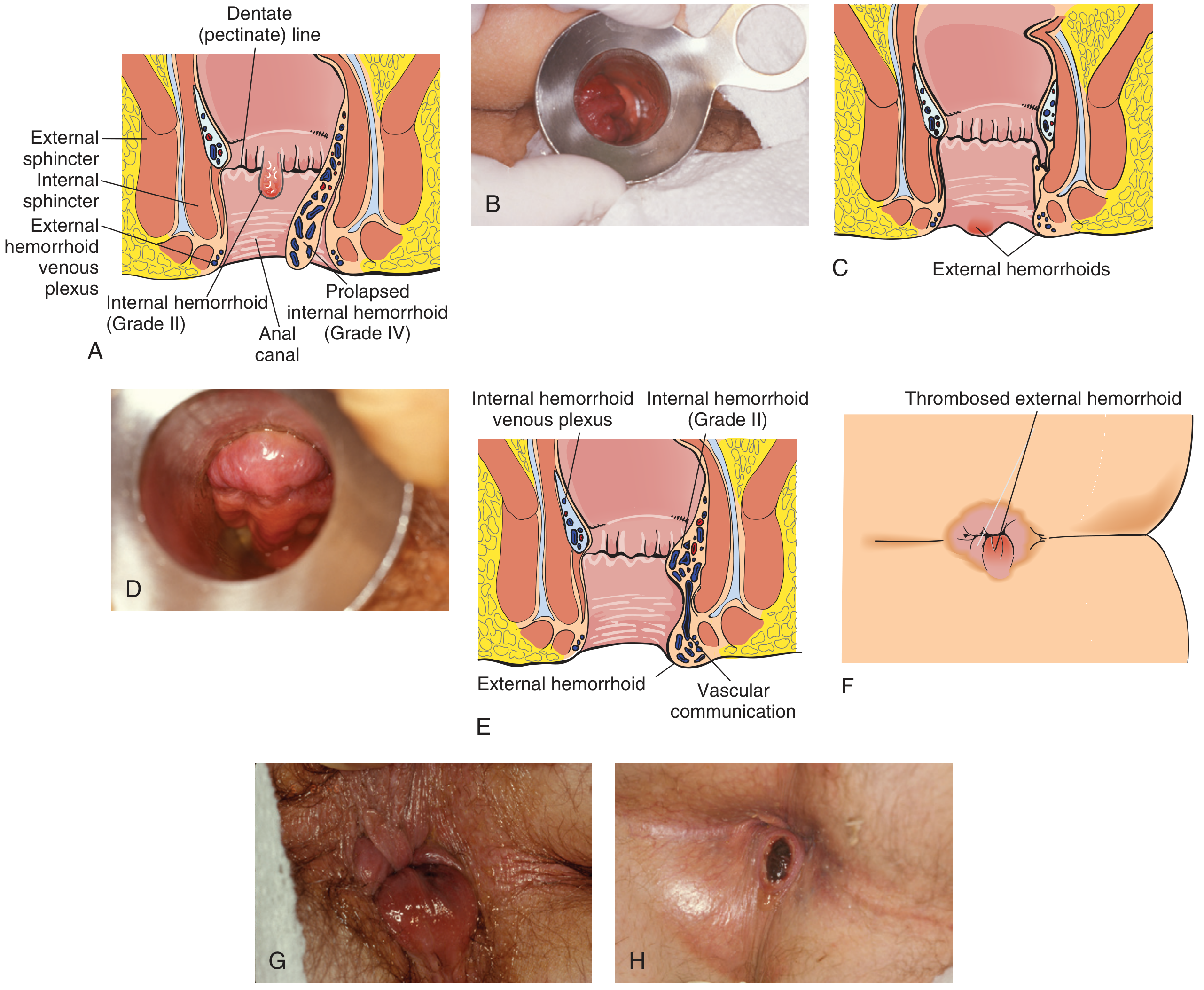
Various types of haemorrhoids: (A) Internal Grade II anatomy, (A) Prolapsed Grade IV internal, (C) External haemorrhoids, (E) Mixed haemorrhoid with vascular communication, (F) Thrombosed external haemorrhoid
— Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
3. Classification of Internal Haemorrhoids — By Degree of Prolapse (Grade I–IV)
Internal haemorrhoids are further graded by the degree of prolapse, assessed on anoscopy:
| Grade | Position / Prolapse | Key Symptoms |
|---|---|---|
| Grade I | Bulge into the anal canal; do not prolapse beyond the anal verge | Painless bright-red bleeding |
| Grade II | Prolapse beyond the anal verge on straining/defaecation; reduce spontaneously | Bleeding, pressure, itching |
| Grade III | Prolapse beyond the anal verge; require manual reduction | Bleeding, pressure, mucoid drainage |
| Grade IV | Permanently prolapsed; cannot be reduced | Pain, bleeding, pressure, mucoid drainage |
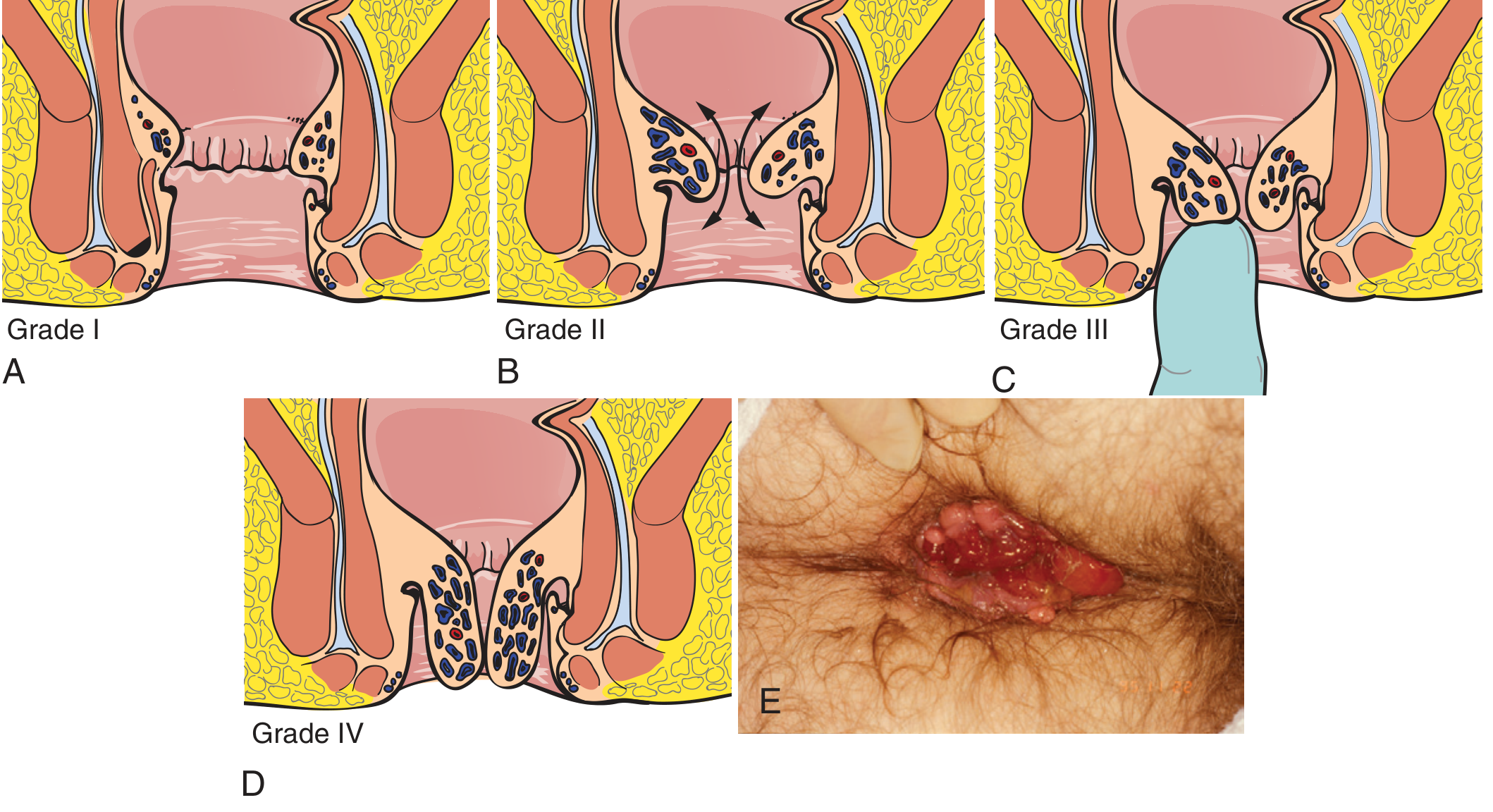
Grading of internal haemorrhoids: (A) Grade I — cushions present, no prolapse; (B) Grade II — prolapse with spontaneous reduction; (C) Grade III — prolapse requiring digital reduction; (D) Grade IV — permanently prolapsed; (E) Clinical photo of prolapsed/gangrenous haemorrhoids
— Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.
Key diagnostic step: Anoscopic examination is the cornerstone for diagnosis and grading of internal haemorrhoids.
4. Special Subtypes
Thrombosed External Haemorrhoid
- Clot forming in external haemorrhoidal plexus
- Presents as a sudden, acutely painful perianal lump
- Not involving mucosal prolapse
- Best treated by excision (not incision and drainage) within 72 hours of onset
Thrombosed/Gangrenous Internal Haemorrhoid (Grade IV)
- A surgical emergency
- Irreducible prolapse with vascular compromise → gangrene/necrosis
- Requires emergent haemorrhoidectomy
Skin Tags
- Residual fibrotic masses of stretched skin after thrombosis or surgery
- Asymptomatic except for hygiene issues and occasional pruritus
5. Aetiology & Pathophysiology
| Factor | Mechanism |
|---|---|
| Chronic straining / constipation | Increased intra-abdominal/venous pressure → cushion engorgement |
| Prolonged time on toilet | Sustained pelvic floor pressure |
| Diarrhoea | Repeated trauma to mucosa, sphincter hypertonia |
| Pregnancy / childbirth | Direct venous compression, straining in labour |
| COPD | Chronic raised intra-abdominal pressure |
| Portal hypertension | Rectal varices (via superior–middle haemorrhoidal communications); NOT a direct cause of classic haemorrhoids |
| Familial predisposition | Possible genetic component (vs. acquired dietary factors) |
— Current Surgical Therapy 14e; Rosen's Emergency Medicine
6. Clinical Features
| Symptom | Notes |
|---|---|
| Bright-red rectal bleeding | Most common; blood on paper or in bowl; painless unless thrombosed |
| Prolapse | Tissue protruding at anus, possibly requiring reduction |
| Mucoid/watery discharge | Grades III–IV; causes pruritus ani |
| Pain | Only with external/thrombosed haemorrhoids; internal haemorrhoids are painless (no somatic fibres above dentate line) |
| Perianal itch/moisture | Common with larger haemorrhoids |
| Anaemia | Rare; from chronic or heavy bleeding |
7. Management Summary by Classification
| Classification | Management |
|---|---|
| Grade I internal | Conservative (WASH regimen, dietary fibre, sitz baths) |
| Grade II internal | Conservative first; banding, infrared coagulation (IRC), or sclerotherapy if refractory |
| Grade III internal | Rubber band ligation (RBL), sclerotherapy, or elective haemorrhoidectomy |
| Grade IV (non-thrombosed) | Non-emergent haemorrhoidectomy |
| Thrombosed external | Excision in emergency department within 72 h |
| Thrombosed/gangrenous Grade IV | Emergent haemorrhoidectomy |
WASH regimen: Warm water sitz baths · Analgesics (paracetamol/NSAIDs) · Stool softeners · High-fibre diet (20–30 g/day)
— Rosen's Emergency Medicine; Current Surgical Therapy 14e; Pfenninger and Fowler's
8. Key Office/Surgical Procedures
| Procedure | Grade Indication | Notes |
|---|---|---|
| Rubber Band Ligation (RBL) | II–III | Band placed ≥2 cm above dentate line; >90% success; avoid anticoagulants |
| Infrared Photocoagulation (IRC) | I–II | No assistant needed; suitable for anticoagulated patients |
| Sclerotherapy | I–II | 5% phenol in almond oil; safe in anticoagulated patients |
| Haemorrhoidectomy | III–IV (failed conservative) | Requires general/regional anaesthesia |
| Haemorrhoidopexy (stapled) | III | Mucosectomy + stapling; faster recovery |
| Doppler-guided haemorrhoidal artery ligation (DGHAL/Mucopexy) | II–III | Minimally invasive; ligation of feeding arteries |
Summary Diagram
HAEMORRHOIDS
├── INTERNAL (above dentate line — mucosa — painless)
│ ├── Grade I → Bulge only, no prolapse, bleeding
│ ├── Grade II → Prolapse + spontaneous reduction
│ ├── Grade III → Prolapse + manual reduction required
│ └── Grade IV → Irreducible prolapse (± thrombosis/gangrene)
│
├── EXTERNAL (below dentate line — anoderm — painful)
│ └── Thrombosed external haemorrhoid → Painful lump
│
└── MIXED (spans dentate line — both plexuses)
Sources: Current Surgical Therapy 14e | Pfenninger and Fowler's Procedures for Primary Care, 3rd ed. | Rosen's Emergency Medicine: Concepts and Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.