
IMG-20260706-WA0038(1).jpg
Diagnosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Diagnosis: Amebic Liver Abscess (Entamoeba histolytica)
Case Summary - Key Clues
| Clue | Significance |
|---|---|
| 48-year-old male Fijian soldier | Typical demographic - males <50, travel to endemic region (Pacific/tropics) |
| Fever + dyspnea + interstitial pattern initially | Misleading initial presentation; treated as CAP |
| Failed standard antibiotics (amoxicillin, azithromycin) | No response to bacterial coverage - atypical pathogen |
| CT showing multiple liver abscesses | Key radiological finding |
| Blood & abscess cultures negative for bacteria | Rules out pyogenic abscess |
| Parasite detected by PCR of abscess material | Diagnostic - nucleic acid amplification of E. histolytica |
| Responded to metronidazole (continued) | Drug of choice for invasive amebiasis |
| Discharged on paromomycin + metronidazole | Luminal agent added to eradicate intestinal cysts |
| Stool antigen & PCR negative after treatment | Confirms eradication of luminal infection |
Diagnosis
Amebic Liver Abscess (ALA) caused by the protozoan parasite Entamoeba histolytica
This is the most common extraintestinal form of invasive amebiasis, accounting for an estimated 100,000 deaths per year globally. - Maingot's Abdominal Operations, p. 929
Pathophysiology
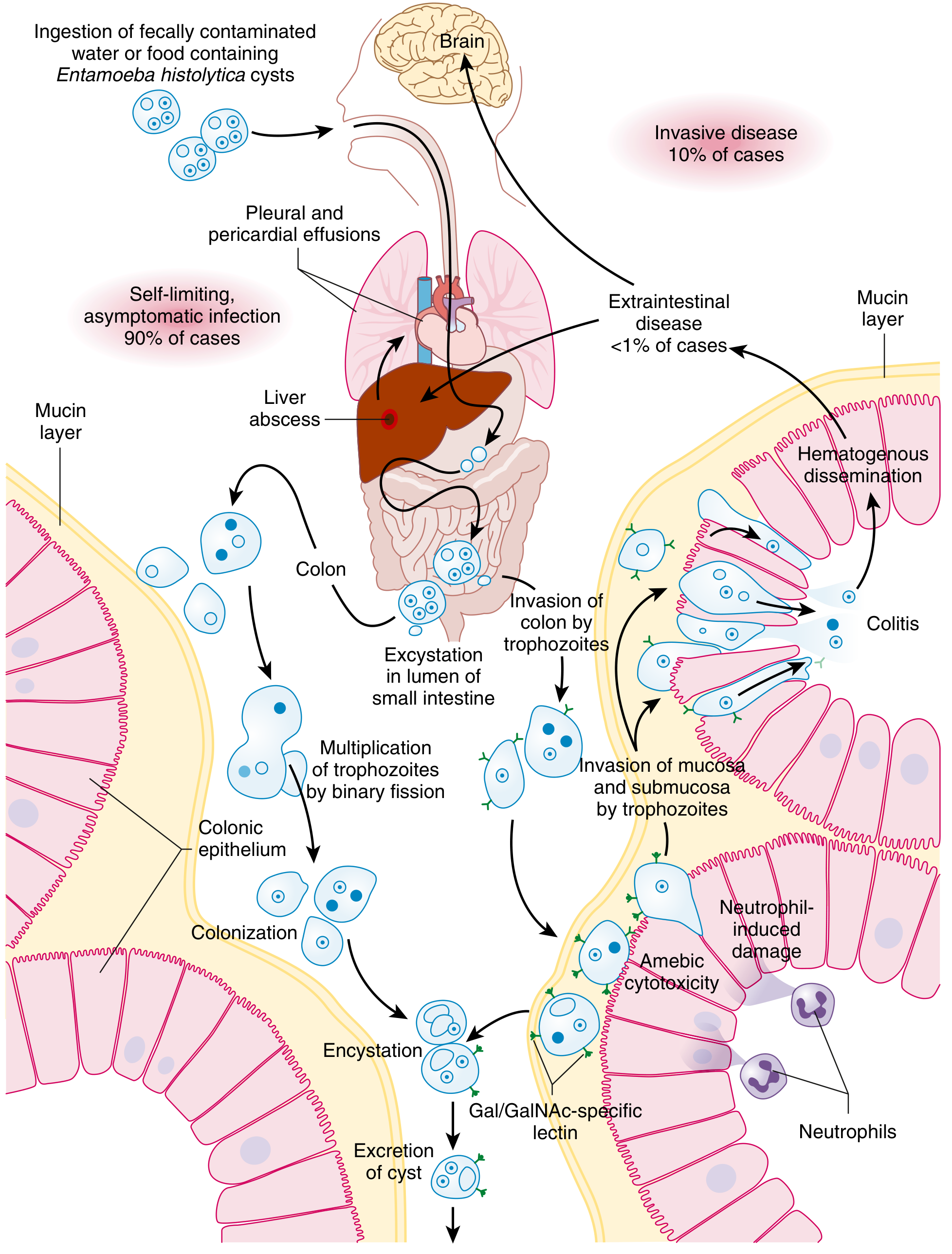
Infection follows fecal-oral transmission. E. histolytica cysts resist gastric acid and excyst in the bowel lumen. Trophozoites invade the intestinal mucosa, travel via mesenteric veins to the liver, and cause liquefactive necrosis - producing the classic "anchovy paste" appearance of abscess contents. - Maingot's Abdominal Operations, p. 929
Why NOT Pyogenic Abscess?
| Feature | Amebic | Pyogenic |
|---|---|---|
| Age | <50 years | >50 years |
| Sex ratio | 10:1 male | ~1:1 |
| Culture | Negative | Usually positive |
| Travel history | Endemic region | Local source (biliary, GI) |
| Diagnosis | PCR / serology | Culture |
| Response to metronidazole | Excellent | No response |
The negative bacterial cultures combined with a positive PCR for a parasite, and dramatic response to metronidazole clinch the amebic etiology. - Maingot's Abdominal Operations, p. 930
Treatment (as used in this case)
- Metronidazole 750 mg TID x 7-10 days - drug of choice, 95% success rate for tissue disease
- Paromomycin (or iodoquinol/diloxanide furoate) - luminal agent added to eliminate intestinal cyst carriage and prevent relapse
- Percutaneous drainage may be needed for large or complicated abscesses (drain placed here due to multiple abscesses)
- Schwartz's Principles of Surgery, p. 1541-1546; Goldman-Cecil Medicine
Why the Stool Tests Were Negative
This is common in ALA. Concurrent intestinal infection is present in only ~30-50% of patients with amebic liver abscess at the time of presentation. After completing treatment with both metronidazole (tissue amebicide) and paromomycin (luminal amebicide), the subsequent negative stool antigen and PCR confirm successful eradication. - Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.