Detail of condition Community Acquired Pneumonia
Reading File
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND "management"[MeSH Terms]
Searching the Web
community acquired pneumonia 2024 2025 guidelines IDSA ATS management
Reading File
Reading File
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Reading File
Reading File
Searching Images
community acquired pneumonia chest X-ray consolidation
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive data. Let me compile the complete, detailed answer.
Community-Acquired Pneumonia (CAP)
Definition
Community-acquired pneumonia (CAP) is an acute pulmonary infection occurring in a patient who is not hospitalized or residing in a long-term care facility for ≥14 days before presentation. It involves the alveolar (gas-exchanging) portion of the lung and is distinguished from hospital-acquired, ventilator-acquired, and healthcare-associated pneumonia based on acquisition environment.
Epidemiology
CAP is one of the most common serious health conditions and the most common infectious cause of hospitalization and death in the United States.
- ~3 million cases and 1.6 million hospitalizations annually in the US
- ~7 health care visits/1,000 per year in young adults vs. 96/1,000 in adults ≥85 years
- Hospitalization rate: 1–2/1,000 in young adults → 15–20/1,000 in ages 65–84 → ~40/1,000 in ≥85 years
- ~35% of CAP hospitalizations occur in patients with recent healthcare exposures
- ~25% occur in immunocompromised patients
- Mortality: ~6% during hospitalization; ~15% at 1 month for hospitalized CAP
- Seasonal peaks November–March (influenza, RSV, SARS-CoV-2)
— Goldman-Cecil Medicine, p. 990–992
Pathobiology
Routes of Infection
| Route | Pathogens |
|---|---|
| Microaspiration (primary mechanism) | Most bacterial pathogens (S. pneumoniae, H. influenzae, anaerobes) |
| Inhalation of aerosols | M. tuberculosis, Legionella, B. anthracis |
| Hematogenous spread | S. aureus, E. coli, right-sided endocarditis organisms |
| Viral transmission (fomites/aerosols) | Influenza, RSV, SARS-CoV-2, hMPV |
Host Defense Disruption
Pneumonia arises when one or more pathogens become dominant in the lung microbiome, overwhelming defenses:
- Mucociliary clearance (ciliated epithelium + mucous layer)
- Cough reflex
- Bacteriostatic surfactant lining the alveoli
- Innate and adaptive immune responses (alveolar macrophages, neutrophils)
- Lung microbiome homeostasis (Prevotella, Veillonella, Streptococcus species in healthy lung)
Factors increasing susceptibility:
- Increased oropharyngeal colonization (poor dental hygiene, alcohol use)
- Decreased cough/ciliary function (neurologic disease, COPD, cystic fibrosis)
- Immunosuppression (corticosteroids, chemotherapy, HIV, malnutrition)
- Structural lung disease (bronchiectasis)
- Aging (loss of stem cell reservoirs, mitochondrial dysfunction, upregulated bacterial adhesion receptors)
- Medications: opioids, PPIs, corticosteroids
— Goldman-Cecil Medicine, p. 993
Causative Pathogens
By Patient Setting (in order of decreasing frequency)
| Setting | Pathogens |
|---|---|
| Outpatient — no cardiopulmonary disease | S. pneumoniae, M. pneumoniae, C. pneumoniae, H. influenzae, respiratory viruses, Legionella |
| Outpatient — with cardiopulmonary disease | All above + DRSP, enteric Gram-negatives, anaerobes (aspiration) |
| Inpatient — with comorbidities/modifying factors | S. pneumoniae (incl. DRSP), H. influenzae, M. pneumoniae, C. pneumoniae, enteric GNRs (incl. P. aeruginosa), anaerobes, viruses, Legionella, Pneumocystis jirovecii, endemic fungi |
| Severe CAP — no Pseudomonas risk | S. pneumoniae (incl. DRSP), Legionella, H. influenzae, enteric GNRs, S. aureus, M. pneumoniae, respiratory viruses |
| Severe CAP — with Pseudomonas risk | All above + P. aeruginosa |
Overall: Pneumococcus, H. influenzae, S. aureus, and GNRs cause ~30% of cases; Mycoplasma, Chlamydia, Legionella <5%; respiratory viruses 20–30% (higher post-COVID); no pathogen identified in >50% of cases.
Risk Factors for Specific Pathogens
- DRSP: Age >65, β-lactam use within 3 months, alcoholism, corticosteroids, multiple comorbidities, child in daycare
- Enteric GNRs / P. aeruginosa: Nursing home, underlying cardiopulmonary disease, corticosteroids >10 mg/day prednisone, broad-spectrum antibiotics >7 days in past month, structural lung disease (bronchiectasis), malnutrition
- MRSA / MDR organisms: Hospitalization ≥2 days in past 90 days, broad-spectrum antibiotics in past 3 months, immunosuppression, poor functional status, prior respiratory isolation of MRSA or P. aeruginosa (key 2019 guideline update)
- Anaerobes: Poor dental hygiene (aspiration pneumonia)
— Fishman's Pulmonary Diseases and Disorders, p. 2202
Clinical Manifestations
Symptoms
- Cough (with or without purulent sputum)
- Fever, chills, rigors
- Pleuritic chest pain
- Dyspnea, tachypnea
- Fatigue, myalgias, headache (more common in atypical/viral)
Signs
- Tachypnea (RR >20), tachycardia
- Fever (may be absent in elderly)
- Decreased breath sounds, dullness to percussion
- Bronchial breath sounds, egophony, whispered pectoriloquy over consolidation
- Crackles (rales)
- Mental status changes (especially elderly — may be presenting feature)
"Typical" vs. "Atypical" Presentations
| Feature | Typical (bacterial) | Atypical (Mycoplasma, Chlamydia, viral) |
|---|---|---|
| Onset | Abrupt | Gradual |
| Sputum | Purulent | Scant, nonproductive |
| Fever | High, with rigors | Low-grade |
| Appearance | Acutely ill | May appear well |
| CXR | Lobar/segmental consolidation | Diffuse, patchy interstitial infiltrates |
— Goldman-Cecil Medicine, p. 993
Diagnosis
Clinical Diagnosis
Combination of:
- New pulmonary infiltrate on imaging
- Signs/symptoms of acute respiratory infection (fever, cough, sputum, dyspnea, pleuritic pain)
- Physical exam findings (crackles, bronchial sounds, dullness)
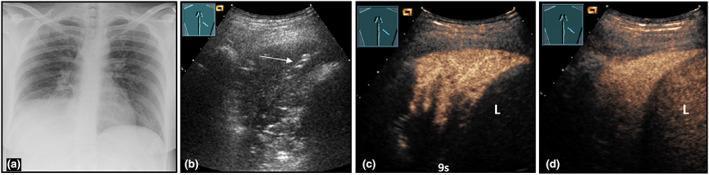
Chest Imaging
- Chest X-ray: First-line — lobar or segmental consolidation (bacterial), diffuse interstitial infiltrates (atypical/viral), or multilobar infiltrates (severe CAP)
- CT chest: Higher sensitivity, used when CXR equivocal or to evaluate complications (abscess, empyema)
Microbiologic Testing
- Sputum Gram stain and culture: Moderate yield; valuable if good-quality specimen obtained
- Blood cultures (×2): Recommended for hospitalized/severe CAP; positive in ~5–10%
- Urinary antigen tests: S. pneumoniae (sensitivity ~80%), Legionella pneumophila serogroup 1
- PCR / multiplex respiratory panels: Increasingly used for viral and atypical pathogens
- Procalcitonin (PCT): Helps guide antibiotic initiation/duration; low PCT argues against bacterial etiology
Severity Scoring
CURB-65 Score (1 point each):
| Criterion | |
|---|---|
| Confusion | New disorientation |
| Urea | BUN >19 mg/dL (>7 mmol/L) |
| Respiratory rate | ≥30 breaths/min |
| Blood pressure | SBP <90 or DBP ≤60 mmHg |
| 65 | Age ≥65 years |
- Score 0–1: Outpatient treatment
- Score 2: Inpatient observation
- Score ≥3: Hospitalize; consider ICU if score 4–5
Pneumonia Severity Index (PSI / PORT Score)
- More precise tool using 20 variables (age, sex, comorbidities, vitals, labs, radiography)
- Classes I–III → outpatient; Class IV → inpatient; Class V → ICU/intensive care
Treatment
Site of Care Decision
- Outpatient: CURB-65 0–1, PSI Class I–II
- Inpatient (non-ICU): CURB-65 ≥2, PSI Class III–IV
- ICU: Severe CAP — either 1 major criterion (septic shock requiring vasopressors, mechanical ventilation) or ≥3 minor criteria (RR ≥30, PaO₂/FiO₂ ≤250, multilobar infiltrates, confusion, BUN ≥20 mg/dL, leukopenia, thrombocytopenia, hypothermia, hypotension needing fluids)
Empiric Antibiotic Therapy
Outpatient Treatment
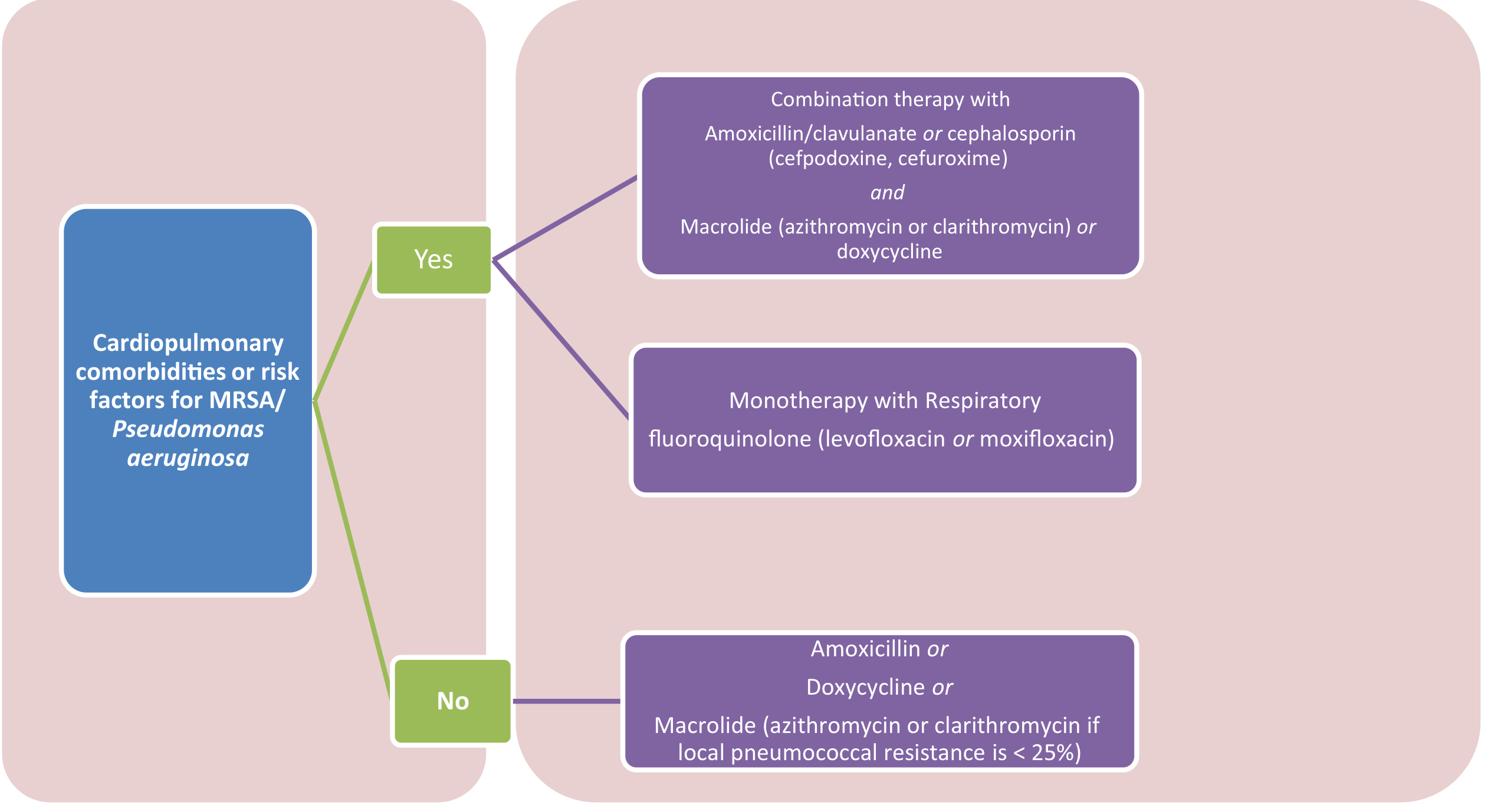
| Clinical Scenario | Preferred Regimen |
|---|---|
| No comorbidities, no MRSA/Pseudomonas risk | Amoxicillin 1 g TID or Doxycycline 100 mg BID or Macrolide (if local pneumococcal resistance <25%) |
| Cardiopulmonary disease or comorbidities | β-lactam (amox/clav, cefpodoxime, cefuroxime) + Macrolide or doxycycline or Respiratory fluoroquinolone (levofloxacin 750 mg/day or moxifloxacin 400 mg/day) |
Key update: Newer ATS/IDSA 2019 guidelines allow β-lactam monotherapy in low-risk outpatients (without comorbidities).
Inpatient, Non-ICU (Hemodynamically Stable)
Standard: β-lactam + macrolide OR respiratory fluoroquinolone
| Drug | Dose |
|---|---|
| Ceftriaxone | 1–2 g IV daily |
| Cefotaxime | 1–2 g IV q8h |
| Ampicillin-sulbactam | 1.5–3 g IV q6h |
| Azithromycin | 500 mg IV/PO daily |
| Levofloxacin | 750 mg IV/PO daily |
| Moxifloxacin | 400 mg IV/PO daily |
For MRSA coverage (if risk factors): Vancomycin 15 mg/kg q12h (targeting trough 15–20 µg/mL) OR Linezolid 600 mg q12h
For Pseudomonas coverage (if risk factors): Piperacillin-tazobactam 4.5 g q6h, Cefepime 2 g q8h, Imipenem 500 mg q6h, Meropenem 1 g q8h
ICU/Severe CAP
| No Pseudomonas risk | Pseudomonas risk |
|---|---|
| Anti-pneumococcal β-lactam + azithromycin or fluoroquinolone | Antipseudomonal β-lactam + antipseudomonal fluoroquinolone (or aminoglycoside + azithromycin) |
— Fishman's Pulmonary Diseases, p. 2202–2204
Antibiotic Duration
- Outpatient/mild: 5 days (if clinically improving)
- Inpatient: 5–7 days; longer if bacteremic, atypical organisms, or complications
- Use clinical stability criteria (defervescence, improving vitals, tolerating orals) to guide de-escalation
Adjunctive Therapy
- Corticosteroids: Increasingly supported in severe CAP — a 2025 Lancet Respiratory Medicine meta-analysis (PMID: 39892408) identified subgroups most likely to benefit; routine use not universally recommended but may reduce duration/severity in select patients
- IV fluids: Guided by hemodynamic status
- Oxygen therapy: Maintain SpO₂ ≥94% (or ≥88–92% in COPD patients)
- Antipyretics, analgesics for symptomatic relief
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | Most common pulmonary complication; 3–5% of hospitalized cases; requires drainage if exudative |
| Lung abscess | Suspect with anaerobic/aspiration pneumonia or post-obstructive pneumonia |
| Necrotizing pneumonia | MRSA-PVL strains, aggressive pathogens |
| Respiratory failure | Hypoxemic; may require HFNC, NIV, or mechanical ventilation |
| Septic shock | Especially with bacteremia (S. pneumoniae, Legionella, GNRs) |
| Acute cardiac events | Atrial fibrillation, new/worsening heart failure, myocardial ischemia — develop in 20–25% of hospitalized patients; major contributor to mortality |
Prevention
| Intervention | Target Population |
|---|---|
| Pneumococcal vaccine (PCV15/PCV20, PPSV23) | Age ≥65, high-risk adults, immunocompromised |
| Annual influenza vaccine | All persons ≥6 months |
| COVID-19 vaccine | All eligible individuals |
| Smoking cessation | All smokers |
| Aspiration precautions | Dysphagia, neurologic disease, head-of-bed elevation |
| Oral hygiene | Reduces oropharyngeal colonization |
Recent Evidence
Three high-quality studies (2025) are worth noting:
-
Drug-resistant pathogens in CAP — A systematic review and meta-analysis (PMID: 40107661) identified key risk factors for MDR organisms in CAP, refining who needs broader empirical coverage beyond standard regimens.
-
Empiric therapy for moderate-to-severe CAP — A network meta-analysis in Clinical Microbiology and Infection (PMID: 40602496) compared antibiotic regimens for hospitalized CAP, informing choice of combination vs. monotherapy.
-
Corticosteroids in CAP — A data-driven meta-analysis in Lancet Respiratory Medicine (PMID: 39892408) identified specific patient subgroups likely to benefit from adjuvant corticosteroids, moving toward individualized therapy.
A 2025 ATS/IDSA guideline update has been published (as noted by GuidelineCentral); consult the current ATS/IDSA 2025 guideline for the latest recommendations, as they may update the 2019 framework.
Key Takeaways
- CAP is defined by community acquisition and diagnosed by new infiltrate + clinical syndrome
- S. pneumoniae remains the leading bacterial cause; viral etiology (including COVID-19) accounts for up to 30%
- Severity scoring (CURB-65, PSI) drives site-of-care decisions
- Empirical therapy is stratified by comorbidities, risk factors, and severity — β-lactam monotherapy is now acceptable in truly low-risk outpatients
- Cardiac complications (AF, ischemia, heart failure) develop in 20–25% of hospitalized patients and are major drivers of morbidity
- Vaccination against pneumococcus, influenza, and COVID-19 is the cornerstone of prevention
Sources: Goldman-Cecil Medicine (9780323930345), Fishman's Pulmonary Diseases and Disorders (9781260473940), Tintinalli's Emergency Medicine (9781260019933)
This is a shared conversation. Sign in to Orris to start your own chat.