Physiology of aiging
Reading File
Finding Sources
Finding Sources
Searching PubMed
physiology aging cellular molecular mechanisms
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Physiology of Aging
Aging (senescence) is the progressive, cumulative deterioration of physiological function during the adult period of life, resulting in increased vulnerability to disease and decreased ability to survive challenges. Below is a system-by-system overview grounded in authoritative textbook sources.
1. Defining Aging
Chronological vs. Biological Age: Chronological age is simply how long a person has lived; biological age reflects the actual rate of senescent deterioration and varies among individuals. No universally agreed panel of biomarkers currently quantifies biological age reliably.
Gompertz Law: After early adulthood, the age-specific death rate (fraction of a cohort dying in a given interval) rises exponentially - this is the foundation of population aging analysis, first described by Benjamin Gompertz in 1825.
Evolutionary perspective: Aging is not an adaptive program. It evolved by default because natural selection has no power over post-reproductive fitness - mutations promoting senescence are simply not eliminated.
- Medical Physiology (Boron & Boulpaep), pp. 1810-1811
2. Cellular & Molecular Mechanisms of Aging
These are the fundamental drivers of all organ-level changes:
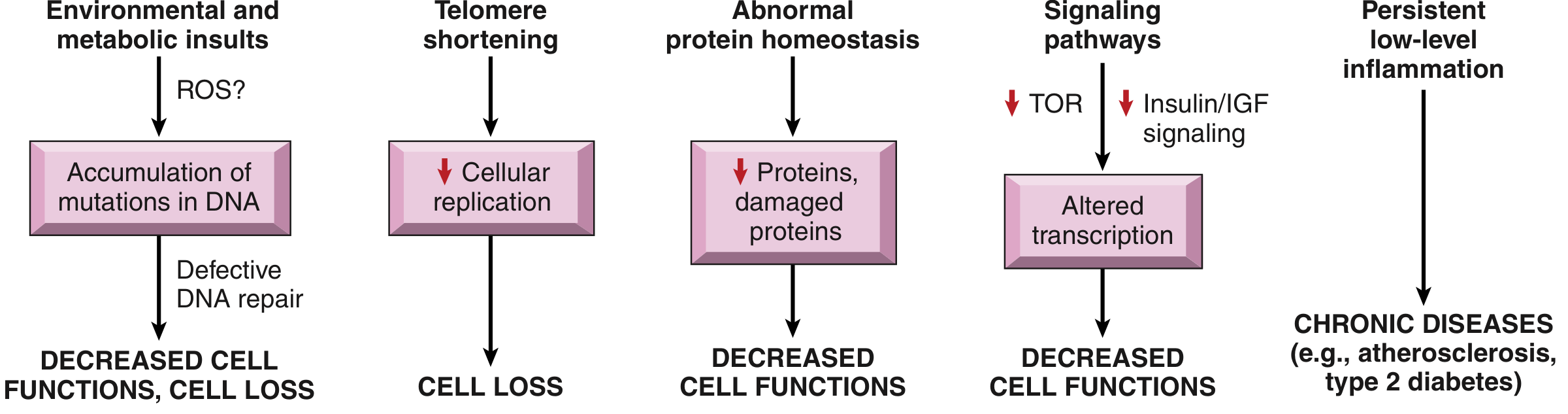
a. DNA Damage Accumulation
- Spontaneous deamination of cytosine, ROS-induced mutations, UV radiation, and chemotherapeutic agents all generate mutations that accumulate with time.
- Many inherited premature aging syndromes (e.g., Werner syndrome) involve mutations in DNA repair proteins, confirming the centrality of genomic maintenance.
- Consequences include: epigenetic alterations, defective protein synthesis, mitochondrial dysfunction, and cellular senescence.
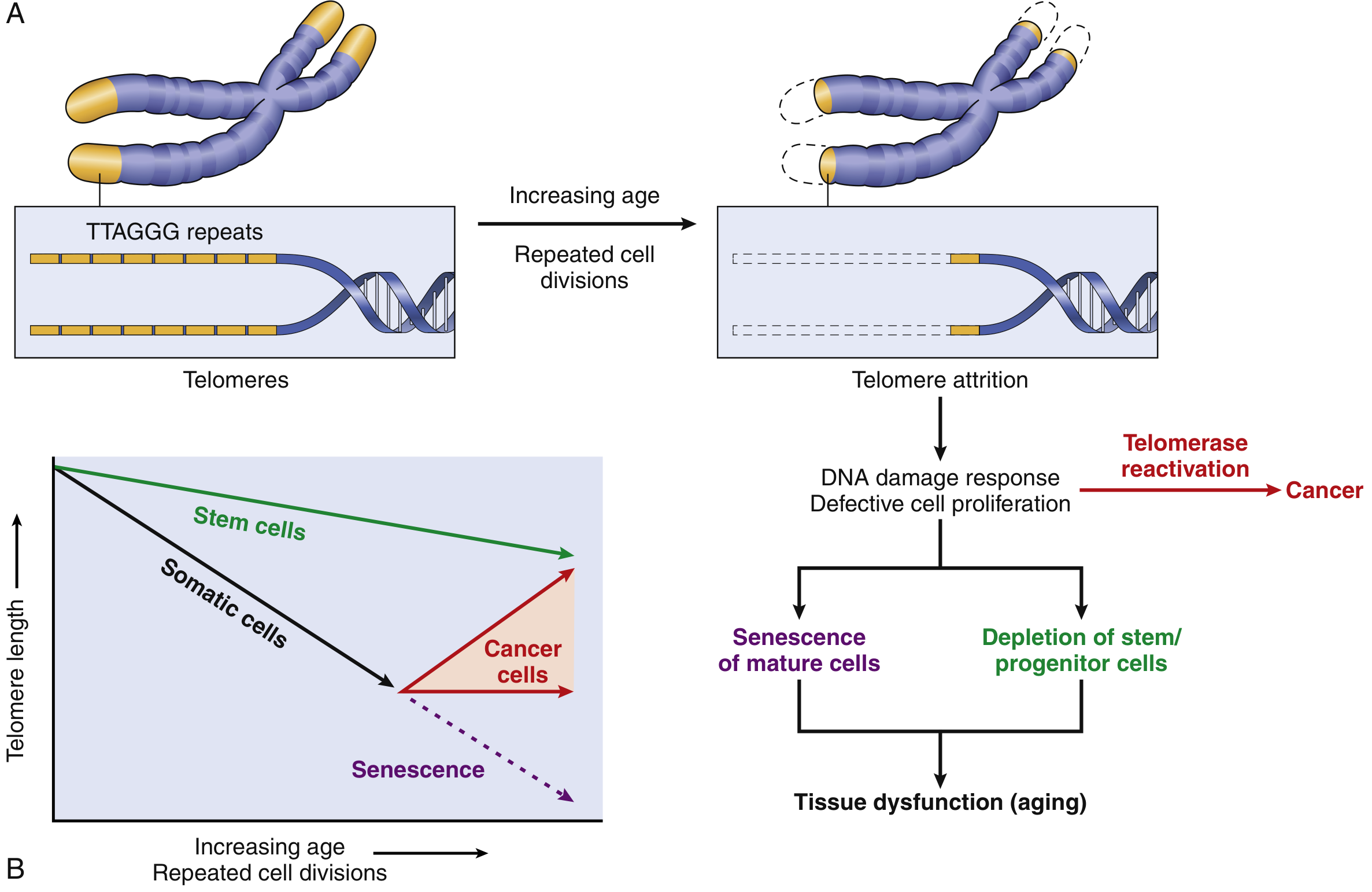
b. Telomere Shortening and Replicative Senescence
- With each cell division, a small segment of the telomere (protective DNA repeat sequences at chromosome ends) is not replicated. After enough divisions, critically short telomeres are sensed as "broken DNA," triggering irreversible cell cycle arrest - replicative senescence.
- Telomerase (an RNA-protein complex) normally maintains telomere length in germ cells and stem cells, but is absent in most somatic cells. In cancer cells, telomerase is reactivated, enabling indefinite proliferation.
- Inherited telomerase deficiencies cause "telomeropathies": aplastic anemia, pulmonary fibrosis, liver fibrosis, premature graying, nail and skin abnormalities.
c. Altered Protein Homeostasis (Proteostasis)
- Aged cells lose the capacity to degrade misfolded proteins (via autophagy and the ubiquitin-proteasome system). Accumulation of misfolded proteins disrupts cell survival, replication, and function, and may trigger apoptosis.
d. Dysregulated Nutrient Sensing and Signaling Pathways
- Calorie restriction (the most reproducibly lifespan-extending intervention in model organisms) alters IGF-1 and mTOR signaling, switching cells from growth/proliferation mode to damage-repair mode.
- Inhibitors of IGF-1 and mTOR have prolonged lifespan in experimental models, though translation to humans remains uncertain.
e. Persistent Inflammation ("Inflammaging")
- Accumulated damaged cells, lipids, and DNA activate the inflammasome, driving low-level chronic inflammation.
- This inflammaging contributes to atherosclerosis, type 2 diabetes, and other chronic diseases of aging. Inflammatory cytokines further accelerate cellular aging, creating a vicious cycle.
- Robbins & Kumar Basic Pathology, pp. 38-40
3. Body Composition Changes
- Sarcopenia: Progressive loss of skeletal muscle mass and strength (primary decline in type IIa fibers), beginning in the 4th decade. Accounts for most of the decline in basal metabolic rate.
- Increased adiposity: Body fat increases, particularly in women (who maintain total body mass as fat offsets bone and muscle loss). In men, total body mass actually declines because muscle loss outpaces fat gain.
- Reduced total body water: Reflects loss of intracellular (muscle) water and gain of adipose tissue.
- Changes in protein binding: Small decrease in plasma albumin (relevant for acidic, albumin-bound drugs); small increase in alpha-1-acid glycoprotein (relevant for basic drugs).
- Barash Clinical Anesthesia 9e, p. 2720
4. Cardiovascular System
Structural Changes
- Arterial stiffening: Loss of compliance in conduit arteries (aorta to arterioles). This is arguably the central cardiovascular event of aging.
- Systolic hypertension: Two mechanisms - (1) increased pressure needed to stretch the stiffened aorta during ejection, and (2) faster return of reflected pressure waves, which arrive before ejection is complete and increase afterload - causing LV hypertrophy.
- LV hypertrophy further stiffens the ventricle and slows diastolic relaxation.
- Venous stiffening: Impairs the venous reservoir function, making venous pressure (and thus cardiac filling) more labile in response to volume changes.
Diastolic Dysfunction
- Slowed LV relaxation impairs early diastolic filling; the ventricle becomes more dependent on the atrial kick. Left atrial pressure must rise to preserve filling - this is diastolic dysfunction, which becomes more prevalent with age.
- Most cases of CHF in very old patients are due to diastolic dysfunction, NOT systolic dysfunction.
Resting vs. Exercising Heart
- Resting cardiac output and ejection fraction are preserved in healthy aging.
- Beta-receptor responsiveness decreases (not due to receptor downregulation but a defect in intracellular coupling). Both heart rate and contractility respond less to catecholamines.
- Maximum heart rate falls (approximation: 220 minus age). Exercise cardiac output is maintained more by Frank-Starling (increased end-diastolic volume) than by heart rate increase - opposite of youth.
- Baroreflex blunting: Decreased heart rate response to blood pressure changes; postural hypotension becomes common.
Conduction System
- Fibrosis of the conduction system predisposes to heart block and sick sinus syndrome. Atrial fibrillation prevalence rises exponentially with age (partly due to atrial enlargement).
Ischemic Preconditioning
- The protective effect of "warm-up angina" diminishes from age 65, meaning prior ischemia no longer reduces infarct size in older adults.
- Barash Clinical Anesthesia 9e, pp. 2730-2846; Medical Physiology, p. 1828
5. Pulmonary System
- Chest wall stiffening: Thorax becomes more barrel-shaped; diaphragm flattens, reducing its mechanical advantage. Increased work of breathing.
- Lung compliance increases (opposite to rest of body): Loss of elastin in lung parenchyma makes lungs easier to inflate but removes the tethering that keeps small airways open.
- Small airway collapse: Without elastin support, small airways collapse at higher lung volumes, causing air trapping, ventilation-perfusion (V/Q) mismatch, and reduced resting arterial PaO2.
- Lung volumes: FEV1 and other static and forced expiratory volumes gradually decrease.
- Closing capacity rises above functional residual capacity in older patients, causing dependent airway closure during tidal breathing.
- Decreased respiratory drive: Blunted response to hypercapnia and (even more markedly) to hypoxia.
- Upper airway tone loss: Hypopharyngeal and genioglossal muscle tone decrease, predisposing to obstruction. Sleep-disordered breathing affects perhaps 75% of people over 65.
- Impaired cough and swallowing: Aspiration is a significant cause of community-acquired pneumonia.
- Pulmonary diffusing capacity (DL) decreases due to reduced alveolar capillary volume.
- Medical Physiology, p. 1828; Barash Clinical Anesthesia 9e, pp. 2738-2739
6. Renal System
- Renal cortical mass decreases 20-25% with age; up to half of glomeruli are lost by age 80.
- GFR declines approximately 1 mL/min/year after age 40 (though longitudinal data show this is not universal - one-third of people show no decline).
- Renal tubular transport, sodium conservation, and urinary dilution/concentration capacity all decrease. Thirst sensation also declines.
- Reduced aldosterone secretion contributes to impaired sodium conservation.
- Bladder changes: Decreased capacity and compliance; uninhibited detrusor contractions increase; decreased detrusor activity raises residual volume. Result: urgency, nocturia, frequency.
- Medical Physiology, p. 1828; Barash Clinical Anesthesia 9e, p. 2721
7. Central Nervous System
- Brain mass begins decreasing at ~age 50 and by age 80 has lost about 10% of its weight.
- Neurotransmitter decline: Dopamine, serotonin, GABA, and especially acetylcholine systems are affected. Acetylcholine loss underlies much of the susceptibility to Alzheimer disease.
- Sensory changes: Decreased touch, vibration, proprioception; high-frequency hearing loss (presbycusis, from cochlear hair cell loss); visual accommodation loss (presbyopia); reduced taste and olfaction.
- Motor slowing: Reaction time increases and becomes more pronounced with complex tasks. Postural stability deteriorates; falls are common.
- Cognitive function: Vocabulary and accumulated knowledge are preserved; processing speed and ability to solve novel problems decline. ~50% of those >85 years have significant cognitive impairment.
- Important: Aging does not prevent neurogenesis. The aged brain can still make new neurons and form new dendritic connections.
- Medical Physiology, pp. 4015-4031; Barash Clinical Anesthesia 9e, p. 2711
8. Endocrine System
- Insulin secretion in response to glucose load decreases; insulin resistance (particularly in skeletal muscle) increases - even healthy elderly may develop perioperative hyperglycemia.
- Testosterone, estrogen, and growth hormone all decline with age - contributing to sarcopenia, fat redistribution, and bone loss.
- Hormonal replacement therapies to prevent sarcopenia and cognitive decline remain controversial without proven clinical benefit.
- Barash Clinical Anesthesia 9e, p. 2700
9. Thermoregulation
- Elderly individuals are prone to hypothermia even in modestly cold environments that would not affect younger adults.
- Both vasoconstriction and shivering thresholds are elevated (impaired): core temperature must fall further before the body initiates protective responses.
- Lower basal metabolism (from sarcopenia) reduces heat production capacity.
- Barash Clinical Anesthesia 9e, p. 2877
10. Musculoskeletal System
- Sarcopenia: Progressive skeletal muscle loss driven by denervation, hormonal decline, and reduced anabolic signaling.
- Bone: Decreased density (especially trabecular bone), increasing osteoporosis risk, particularly postmenopausal women.
- Connective tissue: Collagen cross-linking increases, reducing flexibility. Glycosaminoglycan composition changes (reduced hyaluronic acid and versican; increased decorin) alter joint cartilage properties, promoting osteoarthritis.
- Medical Physiology, p. 4005
11. Gastrointestinal System
- GI function is relatively well preserved in healthy elderly. Minor decreases in gastric acid secretion (reduced parietal cell mass) and bile secretion occur.
- Liver mass and liver blood flow decrease by 20-40%, reducing phase I drug metabolism. Liver reserve remains adequate in the absence of disease.
- Medical Physiology, p. 4069; Barash Clinical Anesthesia 9e, p. 2690
Summary Table
| System | Key Age-Related Change |
|---|---|
| Cellular | Telomere shortening, DNA damage, inflammaging, proteostasis failure |
| Body composition | Sarcopenia, increased fat, reduced TBW |
| Cardiovascular | Arterial stiffness, diastolic dysfunction, blunted beta-response |
| Pulmonary | V/Q mismatch, loss of elastin, increased closing capacity |
| Renal | GFR decline 1 mL/min/yr after 40, impaired Na/water homeostasis |
| CNS | Processing slowing, neurotransmitter decline, brain atrophy |
| Endocrine | Insulin resistance, reduced sex hormones, reduced GH |
| Thermoregulation | Impaired vasoconstriction, shivering; lower heat production |
| Musculoskeletal | Bone loss, osteoarthritis, cartilage degeneration |
Key sources: Medical Physiology (Boron & Boulpaep), Chapter 62; Robbins & Kumar Basic Pathology, Chapter 1; Barash, Cullen & Stoelting's Clinical Anesthesia 9e, Chapter 34.
This is a shared conversation. Sign in to Orris to start your own chat.