Second gas effect details
Reading File
Finding Sources
Finding Sources
Searching the Web
second gas effect anesthesia mechanism nitrous oxide
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from both Barash and Miller's Anesthesia. Here is a detailed explanation:
Second Gas Effect
Definition
The second gas effect is a pharmacokinetic phenomenon that occurs when a high-concentration gas (the "first gas," almost always nitrous oxide - N2O) is administered simultaneously with a low-concentration potent volatile anesthetic (the "second gas"). The rapid, massive uptake of N2O from the alveoli concentrates the remaining alveolar gases - including the volatile agent - thereby accelerating the rise in alveolar partial pressure (FA) of that agent above what would occur with the volatile alone.
Relationship to the Concentration Effect
The second gas effect is a special case of the broader concentration effect. The concentration effect describes how a gas administered at high alveolar concentrations rises faster toward its inspired fraction (FA/FI) because:
- Concentrating effect: As large volumes of the gas are absorbed into blood, the remaining gas mixture is compressed into a smaller volume, so the gas represents a higher fraction of what remains.
- Augmented inflow: Fresh gas from the circuit (at the original FI) rushes in to replace the absorbed volume, topping up the alveolar concentration.
The second gas effect applies these same two mechanisms - but driven by N2O uptake - to a companion agent rather than to N2O itself.
Mechanism - Step by Step
Consider delivering 2% potent anesthetic + 70% N2O + 28% O2:
-
N2O is absorbed rapidly in large volumes - despite its low blood/gas solubility coefficient (~0.47), N2O is delivered in enormous quantities (70% of inspired gas). Its high partial pressure drives massive alveolar-to-blood transfer early in induction.
-
Alveolar volume contracts - the removal of so much N2O reduces total alveolar gas volume. The remaining gases (potent agent + O2 + residual N2O) are now in a smaller space, so each is more concentrated. Example from Barash: with 50% uptake of N2O, alveolar N2O concentration drops by only ~24% despite half the N2O being removed, because volume shrinks proportionally.
-
Potent agent is concentrated - using Barash's numeric example: start with 2% agent in 70% N2O + 28% O2. After 50% N2O uptake (35 parts absorbed), the remaining alveolar mixture has 35 parts N2O, 28 parts O2, and 2 parts agent. The agent is now 2/(2+35+28) = 3.1% - up from 2% with no change in actual delivery.
-
Augmented inflow adds more - as N2O exits, fresh gas at the original FI (still containing 2% agent) flows in to fill the void. This replenishes agent concentration further.
-
Net result: FA of the volatile anesthetic rises faster than it would without N2O, speeding induction.
Additionally, N2O uptake raises alveolar O2 partial pressure as well, augmenting O2 uptake - as noted in Miller's: "the rapid uptake of N2O and reduced gas volume increases alveolar P(iso) and P(O2), thereby augmenting uptake of these 'second' gases."
Graphical Illustration
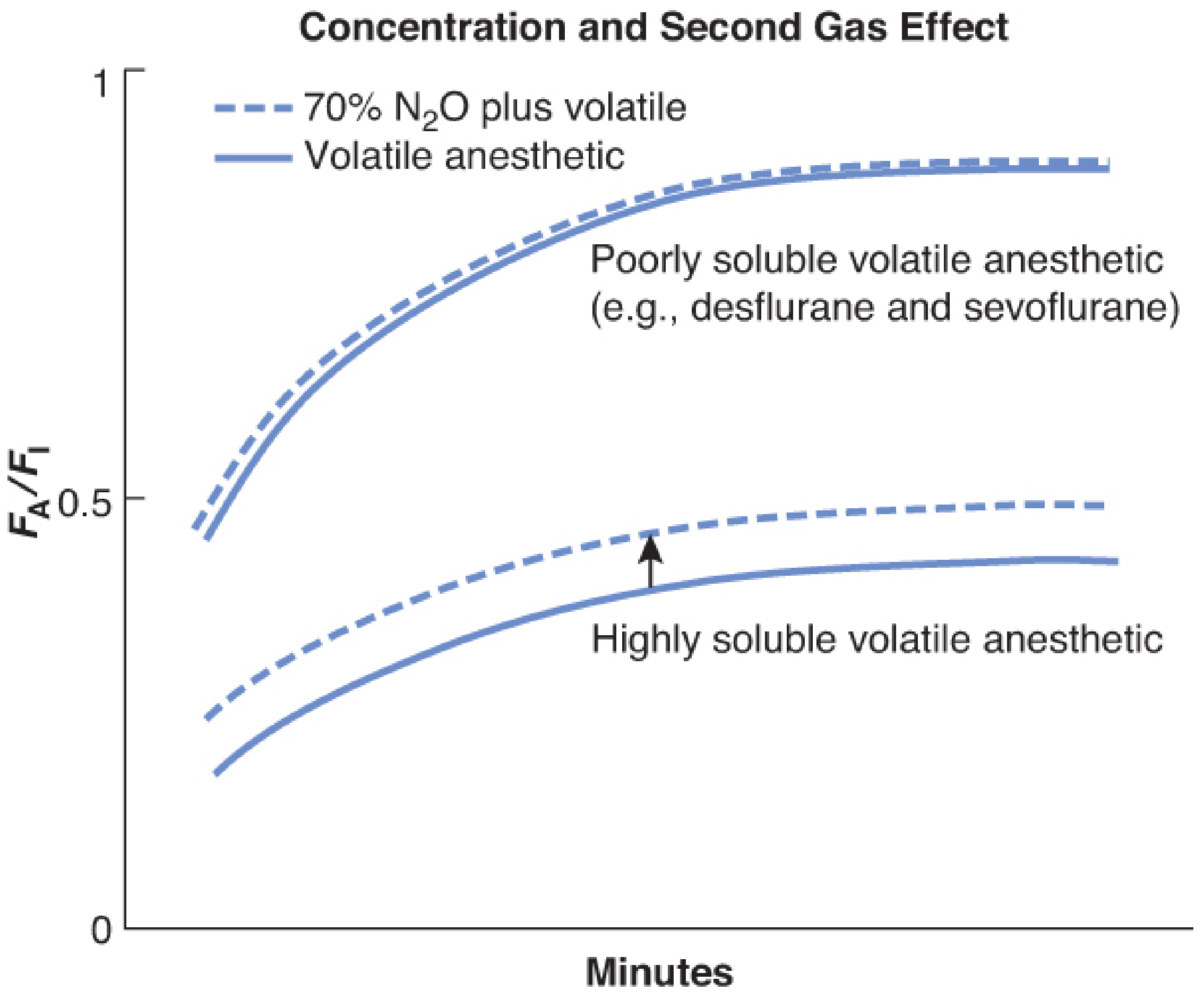
Figure 18-3 from Barash's Clinical Anesthesia, 9e: The FA/FI ratio rises faster when the volatile is given with 70% N2O (dashed) vs. alone (solid). The effect is more pronounced for highly soluble agents.
Which Agents Does It Affect Most?
The second gas effect is more pronounced for highly soluble volatile anesthetics (e.g., halothane, older agents). For poorly soluble agents like sevoflurane and desflurane, FA already rises very steeply on its own, so N2O's contribution - while present - is relatively small.
Clinical Significance
The clinical magnitude of the second gas effect is debated and considered minimal in modern practice:
- Barash states: "Clinically, the second gas effect acts minimally to speed induction."
- Goodman & Gilman notes: "The rapid uptake of N2O from alveolar gas serves to concentrate coadministered halogenated anesthetics; this effect speeds induction of anesthesia" but qualifies its real-world relevance.
- Morgan & Mikhail (7e) cites a reference arguing the second gas effect is "not a valid concept" (Anesth Analg, 1999).
- Miller's acknowledges the effect is real but small, especially with the low-solubility agents used today (sevoflurane, desflurane).
Reverse Second Gas Effect (Diffusion Hypoxia)
At emergence, when N2O administration is stopped, the process reverses:
- N2O diffuses back from blood into the alveoli in large volumes.
- This dilutes alveolar O2 and CO2, potentially causing diffusion hypoxia (Fink effect).
- It also washes out the volatile agent from alveoli, slightly speeding emergence.
- Prevention: administer 100% O2 at the end of N2O anesthesia for several minutes.
Summary Table
| Feature | Detail |
|---|---|
| "First gas" | N2O (high concentration, e.g. 70%) |
| "Second gas" | Potent volatile agent (low concentration) |
| Mechanism | Volume contraction + augmented inflow from massive N2O uptake |
| Direction of effect | Speeds rise of FA of second gas (faster induction) |
| Most affected by | Highly soluble volatiles > poorly soluble ones |
| Clinical magnitude | Small/minimal with modern low-solubility agents |
| Reverse phenomenon | Diffusion hypoxia at emergence |
Sources:
- Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e - p. 1394-1395
- Miller's Anesthesia, 10e - p. 1947-1948
- Goodman & Gilman's Pharmacological Basis of Therapeutics (Nitrous Oxide section)
This is a shared conversation. Sign in to Orris to start your own chat.