Umblical hernia treatment options surgery bailey and love referance
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Bailey & Love is not available in the library, but I have excellent content from Schwartz's, Mulholland & Greenfield's, and Sabiston — all authoritative surgical textbooks. Let me compile the full answer.
Umbilical Hernia — Treatment Options & Surgery
Note: Bailey & Love's Short Practice of Surgery is not available in this textbook library. The information below is drawn from equivalent authoritative surgical references: Schwartz's Principles of Surgery (11e), Mulholland & Greenfield's Surgery (7e), and Sabiston Textbook of Surgery — all of which cover umbilical hernia in the same standard manner taught in Bailey & Love.
Anatomy & Pathogenesis
The umbilical ring normally closes after birth, reinforced by:
- Paired lateral umbilical ligaments (obliterated umbilical arteries)
- Round ligament (obliterated umbilical vein)
- Urachal remnant
- Transversalis fascia
Failure of the ring to close creates a central defect in the linea alba, covered by normal umbilical skin and subcutaneous tissue, allowing protrusion of abdominal contents.
— Mulholland & Greenfield's Surgery, p. 5458
Clinical Features
- Most common abdominal wall defect in infants/children
- Incidence: 25–50% in Black infants; 4–9% in white infants in first months of life
- Generally reducible and asymptomatic
- Incarceration is rare (~1:1,500 cases); more common with smaller defects (≤1 cm)
- Incarceration presents with: abdominal pain, bilious vomiting, tender hard umbilical mass → surgical emergency
Treatment
Conservative (Non-Operative)
| Scenario | Management |
|---|---|
| Children < 2 years, small defect | Observation — ~80% close spontaneously by age 2–3 years |
| Defect < 1 cm at birth | Likely to close by age 4–5 years; defer repair |
| Asymptomatic, no enlargement | Watchful waiting until age 5 years |
Indications to intervene earlier:
- Skin ulceration
- Episode of incarceration
- Defect enlarging or > 2 cm (risk of large skin proboscis if left untreated)
- Significant cosmetic concern to child/family
- Symptomatic hernia in any age
— Schwartz's Principles of Surgery, p. [block 19]; Sabiston Textbook of Surgery, p. [block 28]
In children, prosthetic mesh is never used — primary repair is always achievable.
Surgical Repair Options
1. Primary Open Repair (Standard / Mayo Repair)
The classic technique, suitable for defects < 3 cm:
- Incision: Subumbilical "smile" (semilunar) incision in the skin crease
- Dissection: Hernia sac dissected free circumferentially from overlying skin
- Sac: Excised or reduced
- Fascial closure: Mayo "waistcoat" (vest-over-pants) technique — the superior fascial edge is overlapped over the inferior edge with interrupted non-absorbable or long-acting absorbable sutures in a transverse plane
- Skin: Umbilical skin preserved and sutured to fascial closure for cosmesis; subcuticular skin closure
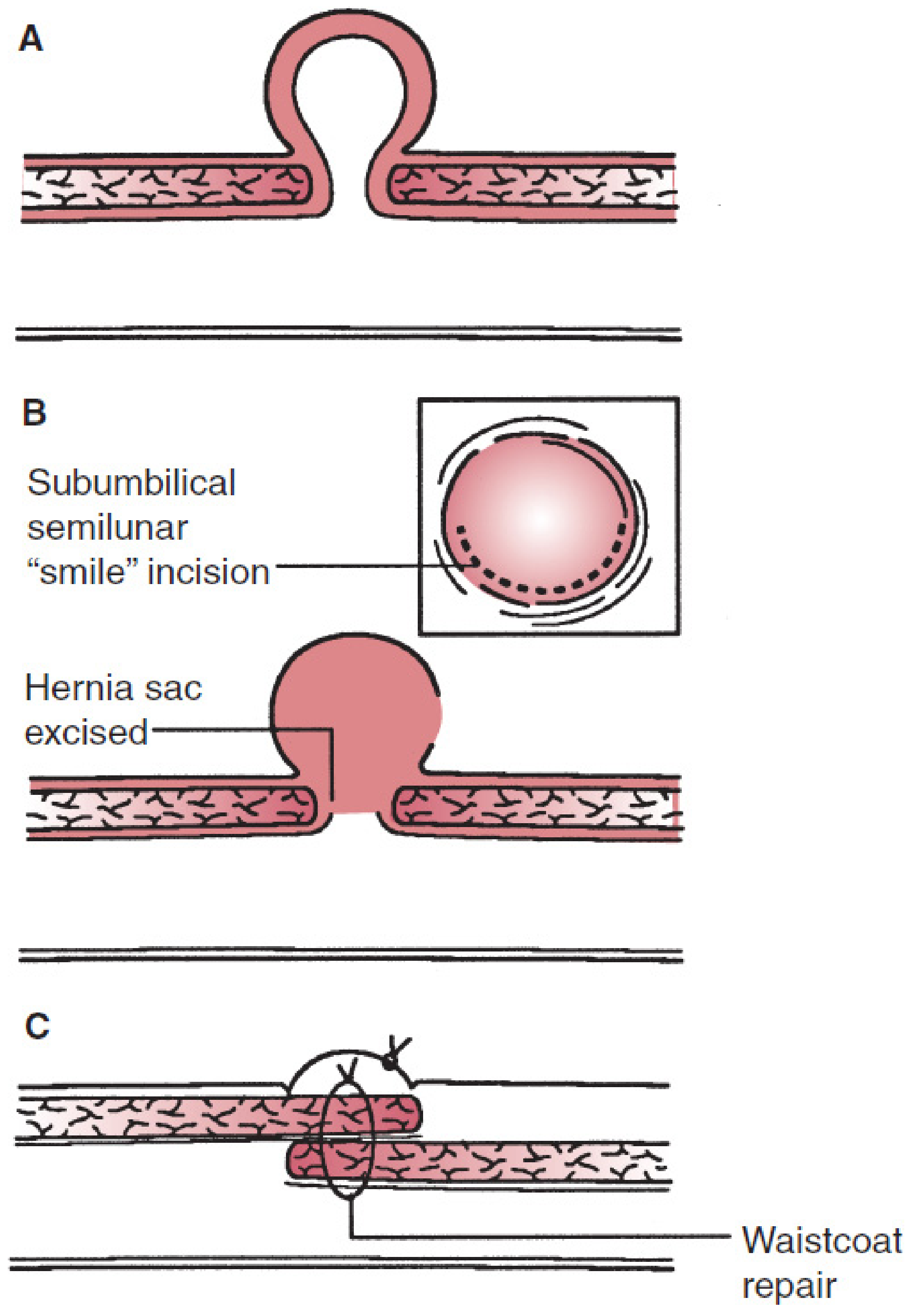
Figure: Mayo repair of an umbilical hernia — Mulholland & Greenfield's Surgery (7e)
Anaesthesia: General anaesthesia, outpatient/day-case procedure
Recurrence: Low; higher in patients with elevated intra-abdominal pressure (e.g., ventriculoperitoneal shunt, ascites)
2. Mesh Repair (Open Preperitoneal / Onlay)
Used for larger defects (> 2–3 cm) in adults:
- Preperitoneal mesh: The peritoneum is bluntly dissected from the undersurface of the posterior rectus sheath; mesh placed in the preperitoneal space, then fascial edges closed over it
- Intraperitoneal mesh: Barrier-coated (composite) mesh placed intraperitoneally — used when preperitoneal dissection is difficult or when defect is small; however, evidence suggests higher complication rates vs. preperitoneal placement
- Falciform and median umbilical ligament fat must be dissected to ensure mesh seats flush against the abdominal wall and prevent fat reherniation
A multicenter RCT showed higher complication rates for intraperitoneal vs. preperitoneal mesh — preperitoneal placement is preferred when feasible.
— Mulholland & Greenfield's Surgery, p. 3724–3725
3. Laparoscopic / Robotic Repair
Indications: Recurrent hernias, defects > 3 cm, or surgeon/patient preference
- Technique mirrors laparoscopic incisional hernia repair
- Options: TAPP (transabdominal preperitoneal) approach — increasingly performed robotically
- Robotic-assisted TAPP is gaining popularity as it facilitates more reliable defect closure
- Potential benefits: decreased operative time, faster return to activity
- Concurrent umbilical hernia repair is a convenient adjunct during TAPP inguinal hernia repair when umbilical access is used
Special Situations
Umbilical Hernia with Ascites / Cirrhosis
- High operative morbidity and mortality — repair undertaken with caution
- Liver transplant candidates: repair at time of transplantation (pre-transplant repair has high morbidity/mortality)
- Patients with incarcerated hernia, thinning or ruptured overlying skin → earlier repair required
- Topical fibrin sealant has been used for leaking umbilical hernias in ascitic patients as a temporizing measure
— Schwartz's Principles of Surgery; Sleisenger & Fordtran's GI & Liver Disease
Summary Table
| Feature | Children | Adults |
|---|---|---|
| Spontaneous closure | ~80% by age 2–3 y | Does not occur |
| Preferred repair | Primary suture (Mayo) | Primary suture or mesh (≥ 2–3 cm) |
| Mesh use | Never | Yes for larger/recurrent defects |
| Approach | Open | Open or laparoscopic/robotic |
| Anesthesia | General (day case) | General (day case) |
| Incarceration risk | Rare (1:1,500) | Slightly higher |
Sources: Schwartz's Principles of Surgery 11e | Mulholland & Greenfield's Surgery 7e | Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.