Clinical anatomy. physiology and methods of larynx research. Acute diseases of the larynx. Laryngeal edema. Laryngeal stenosis. Diphtheria of the larynx.
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Now I have comprehensive information from multiple authoritative sources. Let me compile a thorough, well-structured response.
Clinical Anatomy, Physiology, and Diseases of the Larynx
1. Clinical Anatomy of the Larynx
Regions
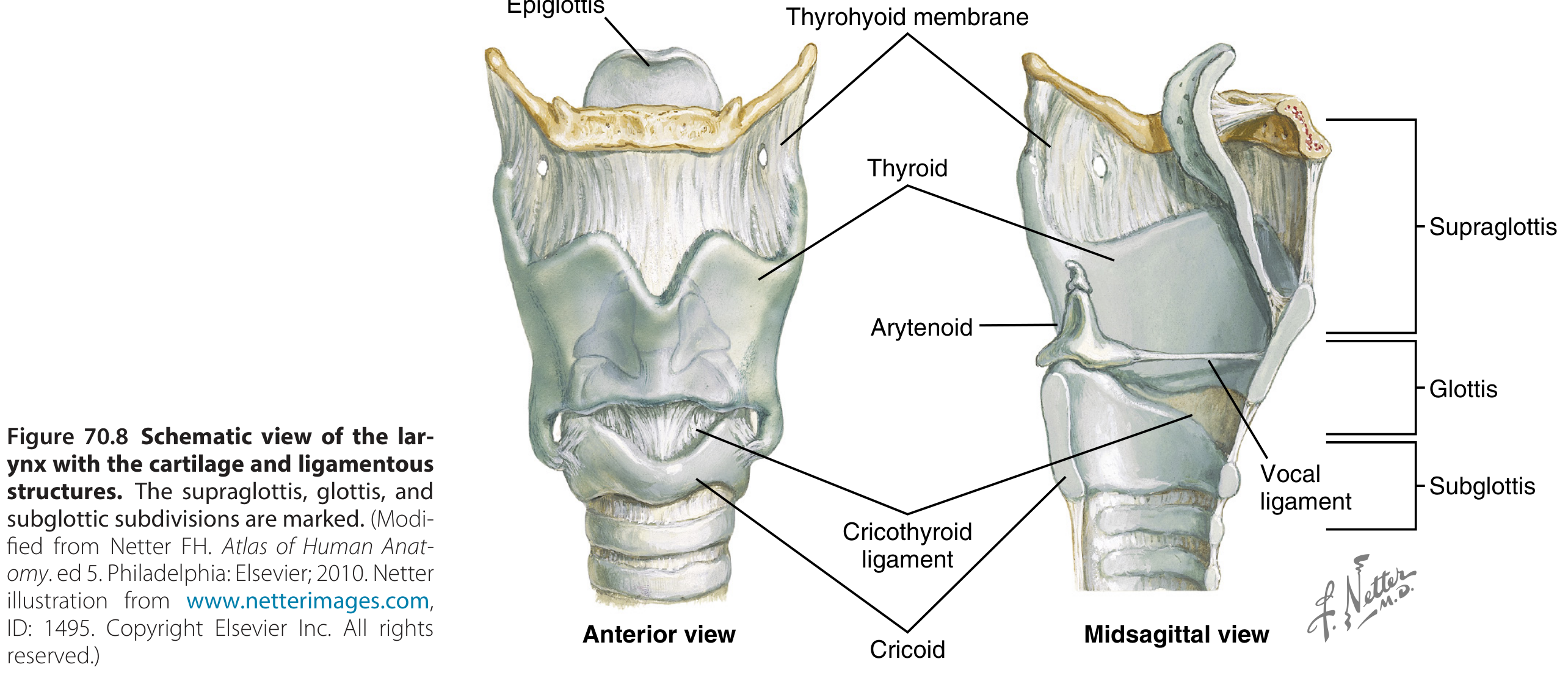
The larynx extends from the epiglottis to the bottom of the cricoid ring and is divided into three regions based on lymphatic drainage:
- Supraglottis — from the tip of the epiglottis to the top of the vocal folds, including the upper arytenoids
- Glottis — from the top of the vocal folds to 1 cm below their top edge (the "true" glottic level)
- Subglottis — below the vocal folds to the first tracheal ring
The subglottis is the narrowest part of the pediatric airway — a clinically critical fact for pediatric intubation and croup.
Skeletal Framework
- Hyoid bone — attached to the skull base and mandible via styloglossus and geniohyoid muscles; attached to the thyroid cartilage by the thyrohyoid ligament
- Thyroid cartilage — paired laminae joined anteriorly; connected to the cricoid by the cricothyroid joint and membrane
- Cricoid cartilage — the only complete ring in the respiratory tract; attached to the trachea below and the thyroid above
- Arytenoid cartilages (paired) — sit on the cricoid ring via synovial cricoarytenoid joints; each bears a vocal process (anteriorly) and a muscular process (posteriorly)
- Corniculate and cuneiform cartilages — small sesamoid structures within the aryepiglottic folds
- Epiglottic cartilage — leaf-shaped, attached inferiorly to the thyroid cartilage; the free upper margin projects into the hypopharynx and closes over the airway during swallowing
Mucosal and Muscular Structures
- Aryepiglottic folds — connect the arytenoid complex to the epiglottis; form the lateral borders of the supraglottis
- False (vestibular) vocal folds — from the body of the arytenoid to the base of the epiglottis
- True vocal folds — membranous, suspended between the thyroid cartilage (anterior commissure) and the arytenoid vocal processes
- Laryngeal ventricle — cleft between the true and false folds; contains mucus-producing cells that lubricate during breathing and speech
Intrinsic Muscles and Their Actions
| Muscle | Action |
|---|---|
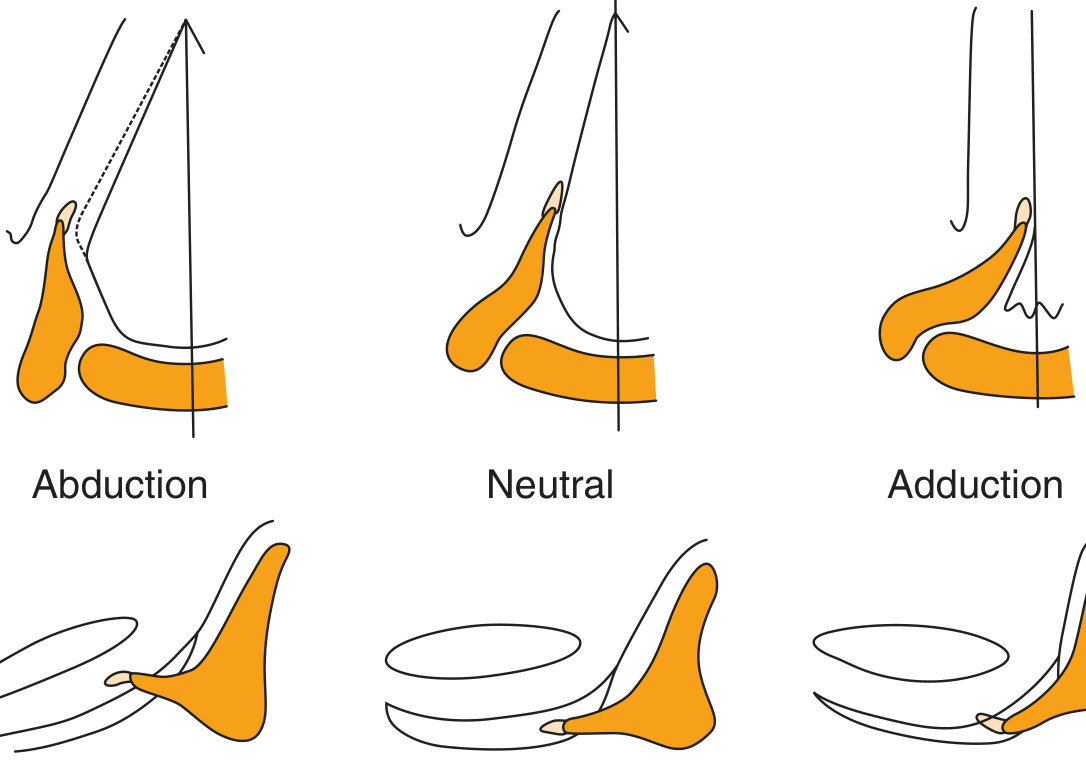
| Posterior cricoarytenoid (PCA) | Only abductor of the vocal fold; pulls the muscular process posteriorly/caudally, rotating the vocal process laterally |
| Lateral cricoarytenoid (LCA) | Primary adductor; rocks the arytenoid to move the vocal process medially |
| Thyroarytenoid (TA) — TAm (lateral) / TAv (vocalis) | Adducts + closes the anterior glottis; shortens and thickens the vocal fold |
| Interarytenoid (IA) | Contributes to adduction (though 3D models suggest isolated contraction may actually abduct) |
| Cricothyroid (CT) | Stretches the vocal folds by tilting the thyroid toward the cricoid; raises pitch; does not adduct or abduct |

Innervation
The larynx is supplied by the vagus nerve (CN X) via two branches:
- Superior laryngeal nerve (SLN) — sensory to the supraglottis + motor to the cricothyroid
- Recurrent laryngeal nerve (RLN) — motor to all other intrinsic muscles; sensory below the glottis
2. Physiology of the Larynx
Three Primary Functions
a) Airway protection during swallowing
The larynx closes at three levels during deglutition: (1) aryepiglottic fold constriction, (2) false vocal fold adduction, and (3) true vocal fold adduction. The epiglottis deflects the bolus laterally over the closed larynx.
b) Respiration and ventilation control
The larynx actively regulates airflow — it is better adapted than any other part of the respiratory tract for this function.
- The PCA begins to contract with each inspiration before the diaphragm activates, widening the glottis to reduce resistance
- With increasing respiratory drive, PCA activity increases proportionally with diaphragmatic activity
- During partial airway obstruction, negative airway pressure is a potent stimulus to the PCA (dilating the airway), while the diaphragm paradoxically decreases force — a protective divergence
- Expiratory adduction by the TA prolongs expiratory duration and modulates airflow resistance
- During sleep, laryngeal closure during expiration is passive (abductor relaxation)
c) Phonation (voice production)
Vocal fold vibration is produced by the myoelastic-aerodynamic theory: subglottal air pressure forces the adducted folds apart; mucosal wave propagation and elastic recoil close them cyclically. The CT muscle controls pitch by lengthening the folds; the TA (vocalis) controls stiffness and thickness. The laryngeal ventricle shape creates turbulence important for vocal fold vibration.
Sensory Function
The larynx contains sensory receptors far more densely than the lungs relative to surface area. These receptors respond to touch, pressure, chemical stimuli, and airflow, exerting powerful influences on breathing, cough, and cardiovascular reflexes via the SLN.
3. Methods of Laryngeal Examination
| Method | Details |
|---|---|
| Indirect laryngoscopy | Mirror examination; classic clinical bedside method |
| Flexible nasopharyngolaryngoscopy | Fiberoptic or chip-tip; allows dynamic vocal fold assessment during speech, breathing, swallowing |
| Rigid videolaryngoscopy / stroboscopy | Gold standard for vocal fold mucosal wave assessment; uses 70° or 90° rigid scope with stroboscopic light |
| Direct laryngoscopy | Under general anesthesia; allows microlaryngeal surgery |
| CT / MRI | For deep tissue invasion, subglottic extension, nodal staging |
| EMG (laryngeal electromyography) | Assesses neuromuscular integrity; helps prognosticate vocal fold paralysis |
| Acoustic analysis | Objective voice parameters (jitter, shimmer, fundamental frequency) |
| Videofluoroscopy (swallowing study) | Dynamic assessment of laryngeal protection during deglutition |
4. Acute Diseases of the Larynx
Acute Laryngitis
The most common laryngeal disorder. May occur as the sole manifestation of allergic, viral, bacterial, or chemical insult, or as part of generalized upper respiratory tract infection. Heavy environmental toxin exposure (tobacco smoke) and gastroesophageal reflux are common triggers. The larynx may also be affected in systemic infections such as tuberculosis and diphtheria.
Clinical features: Hoarseness, dysphonia, odynophonia, sore throat, low-grade fever. Usually self-limited.
Serious sequelae in children: Mucosal congestion, exudation, or edema may cause laryngeal obstruction — a medical emergency in infants because of smaller airway caliber and weaker accessory respiratory muscles. Effective vaccines against H. influenzae and RSV have substantially reduced this risk.
Croup (Viral Laryngotracheobronchitis)
- Caused by respiratory syncytial virus, parainfluenza virus
- Characteristic inspiratory stridor due to subglottic airway narrowing
- "Steeple sign" on AP neck radiograph
- Treatment: humidified air, nebulized epinephrine, dexamethasone
Acute Epiglottitis (Laryngoepiglottitis)
- Caused by H. influenzae type b (now rare with vaccination), β-hemolytic streptococci, RSV
- Sudden swelling of the epiglottis and vocal cords — medical emergency
- "Thumbprint sign" on lateral neck radiograph
- Management: secure airway first (do not examine oropharynx before airway is secured); IV antibiotics; may require intubation or tracheotomy
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Cummings Otolaryngology Head and Neck Surgery
5. Laryngeal Edema
Laryngeal edema is accumulation of fluid in the loose submucosal tissue of the larynx, especially the supraglottis (epiglottis, aryepiglottic folds, arytenoids) — the subglottis is relatively tightly bound.
Causes
| Category | Examples |
|---|---|
| Allergic/anaphylactic | Angioedema (hereditary or acquired), food/drug allergy — most acute |
| Infectious | Epiglottitis, diphtheria, croup |
| Traumatic/iatrogenic | Post-intubation, caustic ingestion, inhalation burns |
| Inflammatory | Autoimmune (e.g., relapsing polychondritis, mucous membrane pemphigoid) |
| Neoplastic | Tumor obstruction with secondary edema |
| Cardiovascular/hepatic | Right heart failure, hypoalbuminemia |
| Radiation | Post-radiation supraglottic edema |
In burn patients, the presence of facial burns, soot in the oral cavity, and endoscopic finding of laryngeal edema predict the need for airway intervention. Endotracheal intubation should be performed early before edema progresses and makes intubation impossible. — Cummings Otolaryngology
Clinical Features
- Inspiratory stridor (partial obstruction) or complete aphonia/apnea
- Muffled "hot-potato" voice, dysphagia, drooling
- Respiratory distress, use of accessory muscles
Management
| Severity | Treatment |
|---|---|
| Mild | Monitor, corticosteroids (IV dexamethasone), antihistamines, treat underlying cause |
| Moderate | IV corticosteroids, nebulized adrenaline (1:1000), supplemental oxygen |
| Severe / imminent obstruction | Immediate intubation (prefer awake fiberoptic if time permits) or emergency surgical airway (cricothyrotomy/tracheotomy) |
| Anaphylaxis | IM epinephrine 0.5 mg (1:1000) as first priority |
6. Laryngeal Stenosis
Laryngeal stenosis is narrowing of the laryngeal lumen resulting in partial or complete airway obstruction. It is distinct from tracheal stenosis in that it involves voice, airway, and swallowing simultaneously — gains in one function often compromise another.
Classification
| Type | Location | Common Cause |
|---|---|---|
| Glottic stenosis (anterior) | Anterior commissure | Trauma, caustic injury |
| Posterior glottic / interarytenoid stenosis | Posterior commissure | Post-intubation (most common in adults) |
| Subglottic stenosis | Below the folds | Post-intubation, tracheotomy, congenital |
| Supraglottic stenosis | Supraglottis | Autoimmune (pemphigoid), radiation, burns |
Etiology
Post-intubation injury is by far the most common cause:
- ~10% of patients show laryngeal pathology 1 day after short-term intubation for surgery
- After prolonged mechanical ventilation, laryngotracheal injuries approach 90%; long-term sequelae in 11%
- The incidence of post-intubation stenosis requiring surgery: 1 in 204,000 adults; 4.9 in 100,000 children
Mechanism: The tube rests on the posterior commissure → pressure necrosis → perichondritis → granulation tissue → interarytenoid scarring → bilateral vocal cord immobility. Poorly sited tracheotomy through or adjacent to the cricoid also causes subglottic stenosis.
Other causes: Laryngeal trauma (blunt/penetrating), caustic/thermal injury, autoimmune disease (GPA/Wegener's — a significant proportion of patients with subglottic stenosis carry autoimmune diagnoses), congenital webs.
Grading (Cotton-Myer Scale for subglottic stenosis)
- Grade I: <50% obstruction
- Grade II: 51–70%
- Grade III: 71–99%
- Grade IV: No detectable lumen
Management
Prevention is the most effective approach:
- Early tracheotomy (<48 hours) in patients on prolonged mechanical ventilation has shown a 30% absolute risk reduction in mortality and fivefold reduction in pneumonia in an RCT, while preventing posterior commissure stenosis almost entirely (which occurs almost exclusively with translaryngeal intubation)
Endoscopic options:
- CO₂ laser incision of webs/scars
- Balloon dilation
- Mitomycin-C application (anti-fibrotic)
Open surgical options:
- Laryngotracheal reconstruction (LTR) — anterior and/or posterior cartilage grafting
- Cricotracheal resection — for severe subglottic stenosis; offers higher decannulation rates
Key principle: Unlike tracheal stenosis (which can often be cured), treating laryngeal stenosis is a compromise between voice, airway, and swallowing — this must be discussed with the patient before surgery. — Cummings Otolaryngology Head and Neck Surgery
7. Diphtheria of the Larynx
Etiology and Pathogenesis
Caused by Corynebacterium diphtheriae, a Gram-positive bacillus. Virulent strains carry the tox gene (encoded by a bacteriophage) producing diphtheria exotoxin, a potent inhibitor of cellular protein synthesis (ADP-ribosylation of EF-2 → blocks translation).
Toxin effects:
- Local: Pseudomembrane formation (coagulative necrosis + fibrin + bacteria + inflammatory cells)
- Systemic: Polyneuritis (5% of respiratory cases; 75% of severe cases), myocarditis (ECG changes in 2/3; clinical myocarditis in 10–25%), renal tubular damage
Epidemiology
- Incubation period: 2–4 days (range 1–8 days)
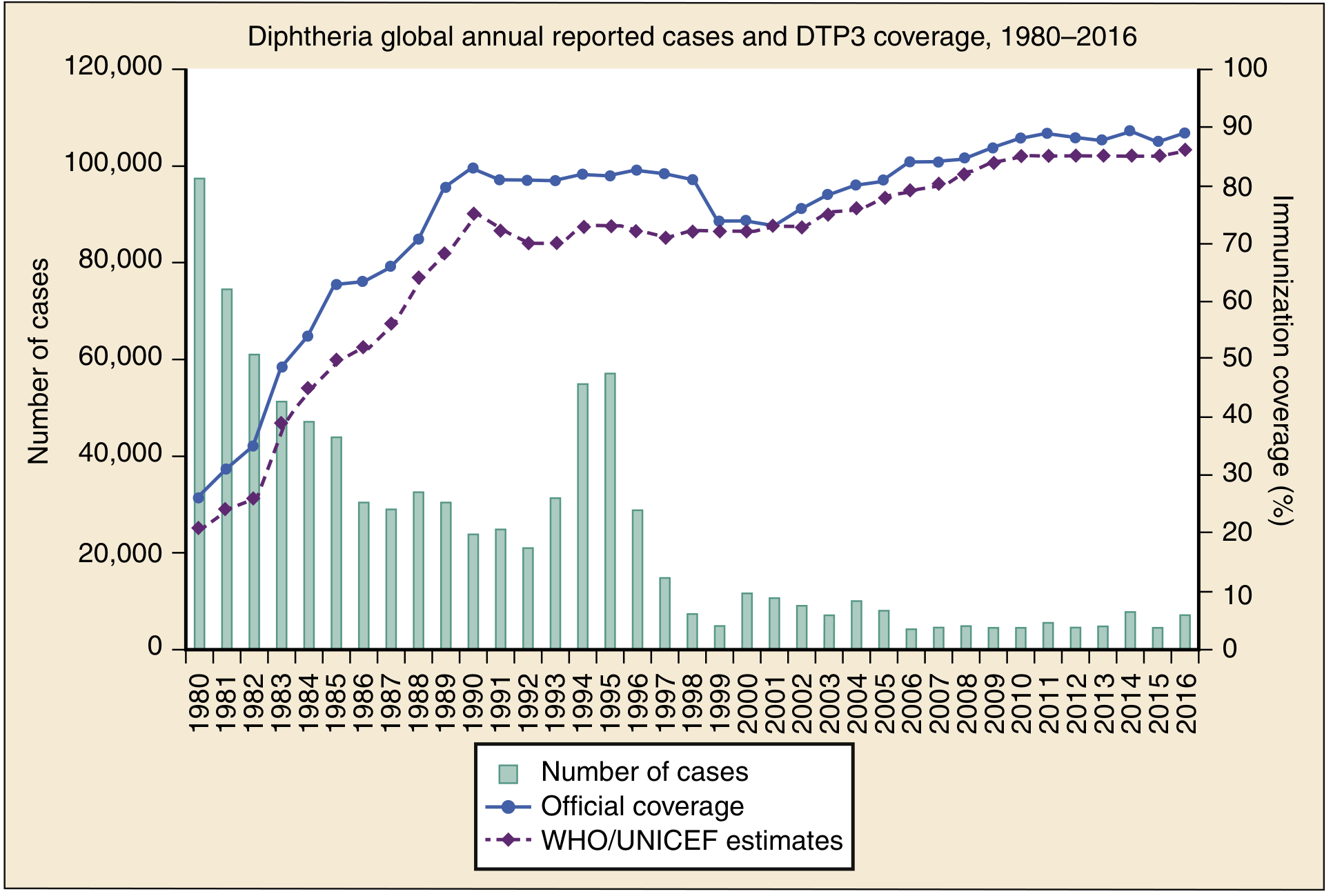
- Primarily affects unvaccinated or incompletely vaccinated populations
- Vaccination (DTaP/DT/Tdap) has dramatically reduced global incidence
Clinical Forms and Features
| Form | Features |
|---|---|
| Faucial (pharyngeal/tonsillar) | Most common and most toxic; membrane on tonsils/pharynx; "bull-neck" (massive cervical lymphadenopathy + tissue infiltration) in malignant form |
| Laryngeal | May begin in the larynx or spread downward from the pharynx; respiratory tract edema → upper airway obstruction; inspiratory stridor, hoarseness, brassy cough ("croup-like") |
| Nasal | Serous or serosanguineous nasal discharge; mild constitutional symptoms; persistent carrier risk |
| Cutaneous | No systemic toxicity; important reservoir |
Clinical diagnosis checklist:
- Pharyngitis/laryngitis with low-grade fever
- Grayish adherent pseudomembrane that bleeds when manipulated (highly characteristic)
- Stridor
- "Bull-neck" cervical edema
- Toxic circulatory collapse
Laboratory Confirmation
- Culture of C. diphtheriae
- Positive Elek test (immunodiffusion for toxin) OR
- PCR for tox gene (subunit A and B)
Treatment
Priority 1 — Airway protection:
Early intubation should be considered for all patients with laryngeal involvement. The degree of membrane formation parallels clinical toxicity.
Priority 2 — Antitoxin (Diphtheria Antitoxin, DAT):
Equine serum antitoxin neutralizes free toxin; must be administered before laboratory confirmation if clinical suspicion is high. Dose depends on membrane location and duration:
| Situation | DAT Dose |
|---|---|
| Pharyngeal/laryngeal involvement ≤2 days | 20,000–40,000 units IV |
| Nasopharyngeal lesions | 40,000–60,000 units IV |
| Systemic disease ≥3 days or diffuse neck swelling | 80,000–100,000 units IV |
Pre-test for equine serum sensitivity (conjunctival or intradermal) before administration; desensitize if positive.
Priority 3 — Antibiotics (stop toxin production):
- Penicillin G or erythromycin for 14 days
- Eliminates the organism; does not neutralize already-released toxin
Priority 4 — Supportive care:
- Respiratory isolation
- IV fluids with assessment for fluid responsiveness (myocarditis may cause heart failure)
- Cardiac monitoring (ECG changes in 2/3 of patients)
- Neurologic surveillance (palatal weakness earliest sign of neuropathy)
Priority 5 — Active immunization:
Infection does not reliably confer immunity; vaccine should be administered after recovery.
Summary Table: Acute Laryngeal Conditions
| Condition | Key Pathogen / Cause | Hallmark Finding | Emergency Management |
|---|---|---|---|
| Acute laryngitis | Viral, smoke, GERD | Hoarseness | Supportive; steroids if severe |
| Croup | Parainfluenza, RSV | Inspiratory stridor, steeple sign | Dexamethasone, nebulized epinephrine |
| Epiglottitis | H. influenzae b | Thumbprint sign, tripod posture | Secure airway first; IV antibiotics |
| Laryngeal edema | Anaphylaxis, intubation, burns | Rapid onset stridor | Epinephrine, airway control |
| Laryngeal stenosis | Post-intubation (most common) | Progressive stridor | Endoscopic/surgical dilation or reconstruction |
| Diphtheria | C. diphtheriae | Adherent gray membrane; bull-neck | DAT + early intubation + penicillin |
Sources: Cummings Otolaryngology Head and Neck Surgery; Murray & Nadel's Textbook of Respiratory Medicine; Rosen's Emergency Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22e
Clinical anatomy. physiology and methods of larynx research. Acute diseases of the larynx. Laryngeal edema. Laryngeal stenosis. Diphtheria of the larynx.
I already provided a comprehensive answer to this exact question in our previous exchange. Here is the full content again for your reference:
Clinical Anatomy, Physiology, and Diseases of the Larynx
1. Clinical Anatomy of the Larynx
Regions
The larynx extends from the epiglottis to the bottom of the cricoid ring and is divided into three regions based on lymphatic drainage:
- Supraglottis — from the tip of the epiglottis to the top of the vocal folds, including the upper arytenoids
- Glottis — from the top of the vocal folds to 1 cm below their top edge
- Subglottis — below the vocal folds to the first tracheal ring (the narrowest part of the pediatric airway — critical for croup and intubation)
Skeletal Framework
- Hyoid bone — suspended by muscles/ligaments; attached to the thyroid cartilage via the thyrohyoid ligament
- Thyroid cartilage — paired laminae joined anteriorly; connected to the cricoid by the cricothyroid joint and membrane
- Cricoid cartilage — the only complete ring in the respiratory tract; attached to the trachea below
- Arytenoid cartilages (paired) — sit on the cricoid via synovial cricoarytenoid joints; bear a vocal process (anterior) and muscular process (posterior)
- Corniculate and cuneiform cartilages — sesamoid structures within the aryepiglottic folds
- Epiglottic cartilage — leaf-shaped; deflects the bolus during swallowing
Mucosal and Muscular Structures
- Aryepiglottic folds — lateral borders of the supraglottis
- False (vestibular) vocal folds — from arytenoid body to epiglottis base
- True vocal folds — suspended between the anterior commissure (thyroid) and vocal processes (arytenoids)
- Laryngeal ventricle — cleft between true and false folds; contains mucus-producing glands
Intrinsic Muscles
| Muscle | Action |
|---|---|
| Posterior cricoarytenoid (PCA) | Only abductor of the vocal fold |
| Lateral cricoarytenoid (LCA) | Primary adductor |
| Thyroarytenoid (TA) — TAm / TAv (vocalis) | Adduction + vocal fold shortening/thickening |
| Interarytenoid (IA) | Contributes to adduction |
| Cricothyroid (CT) | Stretches vocal folds → raises pitch; does not adduct/abduct |
Innervation (CN X — Vagus)
- Superior laryngeal nerve (SLN) — sensory to supraglottis; motor to cricothyroid
- Recurrent laryngeal nerve (RLN) — motor to all other intrinsic muscles; sensory below the glottis
2. Physiology of the Larynx
Three Primary Functions
a) Airway protection during swallowing
Closure occurs at three levels simultaneously: aryepiglottic fold constriction → false vocal fold adduction → true vocal fold adduction. The epiglottis deflects the bolus laterally.
b) Respiration and ventilation control
The larynx is better adapted for regulating airflow than any other part of the respiratory tract:
- The PCA begins contracting with each inspiration before the diaphragm activates, widening the glottis
- During partial airway obstruction, negative airway pressure strongly drives PCA activity (dilating the airway) while the diaphragm paradoxically decreases force — a protective divergence
- Expiratory TA adduction prolongs expiratory duration and modulates airflow resistance
- During sleep, laryngeal closure on expiration is passive (abductor relaxation)
- Laryngeal regulation is not essential for life (patients ventilate through tracheotomy), but optimal quality of life requires normal function
c) Phonation
Based on the myoelastic-aerodynamic theory: subglottal air pressure forces the adducted folds apart; mucosal wave propagation and elastic recoil close them cyclically. The CT stretches the folds (raises pitch); the vocalis (TAv) controls stiffness/thickness (voice quality).
Sensory Function
The larynx is densely supplied with sensory receptors — far more than the lungs relative to surface area. They respond to touch, chemical stimuli, and airflow, exerting powerful influences on breathing, cough, and cardiovascular reflexes via the SLN. — Cummings Otolaryngology Head and Neck Surgery
3. Methods of Laryngeal Examination
| Method | Key Points |
|---|---|
| Indirect laryngoscopy | Mirror exam; classic bedside method |
| Flexible nasopharyngolaryngoscopy | Fiberoptic/chip-tip; dynamic assessment during speech, breathing, swallowing |
| Rigid videolaryngoscopy + stroboscopy | Gold standard for mucosal wave assessment (vocal fold vibration); 70°/90° scope |
| Direct microlaryngoscopy | Under general anesthesia; allows biopsy and microsurgery |
| CT / MRI | Deep tissue invasion, subglottic extension, cervical nodal staging |
| Laryngeal EMG | Neuromuscular integrity; prognostication of vocal fold paralysis |
| Acoustic voice analysis | Objective parameters: jitter, shimmer, fundamental frequency |
| Videofluoroscopy (modified barium swallow) | Dynamic assessment of laryngeal protection during deglutition |
4. Acute Diseases of the Larynx
Acute Laryngitis
May occur in isolation (allergic, viral, bacterial, chemical) or with systemic infections (tuberculosis, diphtheria). Also triggered by tobacco smoke and gastroesophageal reflux. Usually self-limited; most sequelae occur in children where edema causes obstruction due to small airway caliber.
Croup (viral laryngotracheobronchitis)
- Parainfluenza virus, RSV; children
- Subglottic narrowing → characteristic barking cough + inspiratory stridor
- "Steeple sign" on AP neck X-ray
- Treatment: dexamethasone, nebulized epinephrine, humidified air
Acute Epiglottitis (Supraglottitis)
- H. influenzae type b (now rare with vaccination), β-hemolytic streptococci
- Sudden swelling of epiglottis + aryepiglottic folds — medical emergency
- "Thumbprint sign" on lateral neck X-ray; tripod posture; drooling
- Secure the airway first (intubation/tracheotomy) before oropharyngeal examination; then IV antibiotics (ceftriaxone, ampicillin-sulbactam)
— Robbins, Cotran & Kumar Pathologic Basis of Disease
5. Laryngeal Edema
Accumulation of fluid in the loose submucosal tissue of the larynx, predominantly in the supraglottis (epiglottis, aryepiglottic folds, arytenoids); the subglottic submucosa is tightly adherent and less susceptible.
Causes
| Category | Examples |
|---|---|
| Allergic / anaphylactic | Angioedema (hereditary C1-inhibitor deficiency or acquired), food/drug allergy |
| Infectious | Epiglottitis, diphtheria, croup |
| Traumatic / iatrogenic | Post-intubation, inhalation burns, caustic ingestion |
| Inflammatory / autoimmune | Relapsing polychondritis, mucous membrane pemphigoid |
| Cardiovascular / hepatic | Right heart failure, hypoalbuminemia |
| Post-radiation | Supraglottic edema following radiotherapy |
In burn patients, the triad of facial burns + oral soot + endoscopic laryngeal edema predicts the need for airway intervention. Early intubation is mandatory before edema progresses and makes intubation impossible. — Cummings Otolaryngology
Clinical Features
- Inspiratory stridor (partial) or complete apnea
- Muffled "hot-potato" voice, dysphagia, drooling
- Respiratory distress with accessory muscle use
- Rapid progression possible in anaphylaxis
Management
| Severity | Treatment |
|---|---|
| Mild | Corticosteroids (IV dexamethasone 0.15 mg/kg), antihistamines, treat cause |
| Moderate | IV steroids + nebulized adrenaline (1:1000, 5 mL), O₂ |
| Severe / imminent obstruction | Awake fiberoptic intubation if feasible; emergency cricothyrotomy or tracheotomy |
| Anaphylaxis | IM epinephrine 0.5 mg (1:1000) — first priority |
6. Laryngeal Stenosis
Narrowing of the laryngeal lumen causing partial or complete airway obstruction. Unlike tracheal stenosis, treatment is a compromise between voice, airway, and swallowing — gains in one domain often compromise another. Prevention is the most effective strategy.
Classification by Location
| Type | Location | Typical Cause |
|---|---|---|
| Anterior glottic | Anterior commissure web | Trauma, caustic injury, surgery |
| Posterior glottic / interarytenoid | Posterior commissure | Post-intubation (most common in adults) |
| Subglottic | Below vocal folds | Post-intubation, tracheotomy-related, congenital |
| Supraglottic | Supraglottis | Autoimmune, radiation, burns, pemphigoid |
Etiology and Pathogenesis
Post-intubation is the dominant cause:
- ~10% of patients show laryngeal pathology 1 day after even short-term intubation
- After prolonged mechanical ventilation, laryngotracheal injuries approach 90%; long-term sequelae in 11%
- Post-intubation stenosis requiring surgery: 1 in 204,000 adults; 4.9 in 100,000 children annually
Mechanism: The endotracheal tube rests on the posterior commissure → pressure necrosis of the mucosa → perichondritis → granulation tissue → interarytenoid scarring → bilateral vocal cord immobility and airway compromise.
Other causes: Blunt/penetrating laryngeal trauma, caustic/thermal injury, autoimmune disease (GPA/Wegener's — a significant proportion of idiopathic subglottic stenosis patients have autoimmune diagnoses), congenital webs.
Grading (Cotton-Myer Scale)
| Grade | Lumen Obstruction |
|---|---|
| I | < 50% |
| II | 51–70% |
| III | 71–99% |
| IV | No detectable lumen |
Management
Prevention:
- Early tracheotomy (<48 hours) in patients on prolonged mechanical ventilation demonstrated a 30% absolute risk reduction in mortality and fivefold reduction in pneumonia in a RCT, virtually eliminating posterior commissure stenosis (which occurs almost exclusively with translaryngeal intubation)
Endoscopic (minimally invasive):
- CO₂ laser lysis of webs/scar
- Balloon dilation
- Mitomycin-C (anti-fibrotic agent; topical application after lysis)
Open surgical:
- Laryngotracheal reconstruction (LTR) — anterior ± posterior cartilage grafting; favored in children
- Cricotracheal resection (CTR) — resection of the stenotic segment with end-to-end anastomosis; higher decannulation rates in severe stenosis
— Cummings Otolaryngology Head and Neck Surgery
7. Diphtheria of the Larynx
Etiology and Pathogenesis
Caused by Corynebacterium diphtheriae (rarely C. ulcerans). The tox gene (bacteriophage-encoded) produces diphtheria exotoxin, which inhibits protein synthesis via ADP-ribosylation of elongation factor-2 (EF-2), blocking cellular translation.
Local effect: Pseudomembrane — coagulative necrosis + fibrin exudate + bacteria + inflammatory cells; bleeds when forcibly removed (pathognomonic).
Systemic effects:
- Polyneuritis (5% of respiratory cases; 75% of severe cases) — palate affected first, then other cranial nerves, peripheral nerves, spinal cord; usually resolves but may last up to 3 months
- Myocarditis — ECG changes in up to 2/3 of patients; clinical myocarditis in 10–25%; may appear 1–2 weeks after onset
- Renal tubular damage
Epidemiology
- Incubation: 2–4 days (range 1–8 days)
- Degree of toxicity depends on location (pharyngeal > laryngeal > nasal > cutaneous) and extent of membrane formation
- Vaccination (DTaP/DT/Tdap) has dramatically reduced global incidence
Clinical Forms
| Form | Key Features |
|---|---|
| Pharyngeal / faucial | Most common and most toxic; gray membrane on tonsils extending to pharynx; "bull-neck" in malignant form |
| Laryngeal | Begins in larynx or spreads down from pharynx; inspiratory stridor, hoarse/brassy cough; respiratory tract edema → upper airway obstruction |
| Nasal | Serous/serosanguineous discharge; mild systemic illness; persistent carrier risk |
| Cutaneous | Ulcerative skin lesions; minimal systemic toxicity; important reservoir |
Diagnosis Checklist
Suspect case:
- Pharyngitis/laryngitis with low-grade fever
- Grayish adherent pseudomembrane that bleeds when manipulated
Probable case (suspect + any of):
- Stridor
- Bull-neck (cervical edema + tissue infiltration)
- Toxic circulatory collapse
- Myocarditis or acute renal insufficiency
- Recent travel to endemic area or contact with confirmed case
Laboratory confirmed:
- Positive culture of C. diphtheriae
- Positive Elek test (immunodiffusion for toxin) OR PCR for tox gene (subunit A and B)
Treatment
Step 1 — Protect the airway:
Early intubation for all patients with laryngeal involvement (membrane can cause sudden, complete obstruction). Respiratory isolation.
Step 2 — Diphtheria Antitoxin (DAT) — equine serum:
Administer before laboratory confirmation in probable cases; neutralizes free toxin only.
| Clinical Situation | DAT Dose (IV) |
|---|---|
| Pharyngeal/laryngeal — ≤2 days duration | 20,000–40,000 units |
| Nasopharyngeal lesions | 40,000–60,000 units |
| Systemic disease / diffuse neck swelling / ≥3 days | 80,000–100,000 units |
Perform conjunctival or intradermal sensitivity test before administration; desensitize if positive.
Step 3 — Antibiotics (eradicate organism, stop toxin production):
- Penicillin G or erythromycin × 14 days
- Does not neutralize already-circulating toxin — antitoxin is the definitive neutralizing agent
Step 4 — Supportive care:
- IV fluid resuscitation with assessment for fluid responsiveness (toxin may cause myocarditis → heart failure)
- Continuous ECG monitoring
- Neurologic surveillance (palatal weakness is the earliest sign)
Step 5 — Active immunization:
Infection does not reliably confer immunity; vaccinate after recovery. — Rosen's Emergency Medicine; Harrison's Principles of Internal Medicine 22e
Summary: Key Distinguishing Features
| Condition | Pathognomonic Feature | Immediate Priority |
|---|---|---|
| Croup | Barking cough, steeple sign | Dexamethasone + nebulized epinephrine |
| Epiglottitis | Thumbprint sign, drooling, tripod | Secure airway before examination |
| Laryngeal edema (anaphylaxis) | Rapid-onset stridor, urticaria | IM epinephrine 0.5 mg immediately |
| Post-intubation stenosis | Biphasic stridor weeks–months later | Endoscopic dilation/laser; consider CTR |
| Laryngeal diphtheria | Adherent gray membrane that bleeds | DAT + early intubation + penicillin |
Sources: Cummings Otolaryngology Head and Neck Surgery; Murray & Nadel's Textbook of Respiratory Medicine; Rosen's Emergency Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.