Clinical anatomy. physiology and methods of larynx research. Acute diseases of the larynx. Laryngeal edema. 1.aryngeal stenosis. Diphtheria of the larynx
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Clinical anatomy, physiology, and methods of larynx research
Acute diseases of the larynx: laryngeal edema, laryngeal stenosis, laryngeal diphtheria
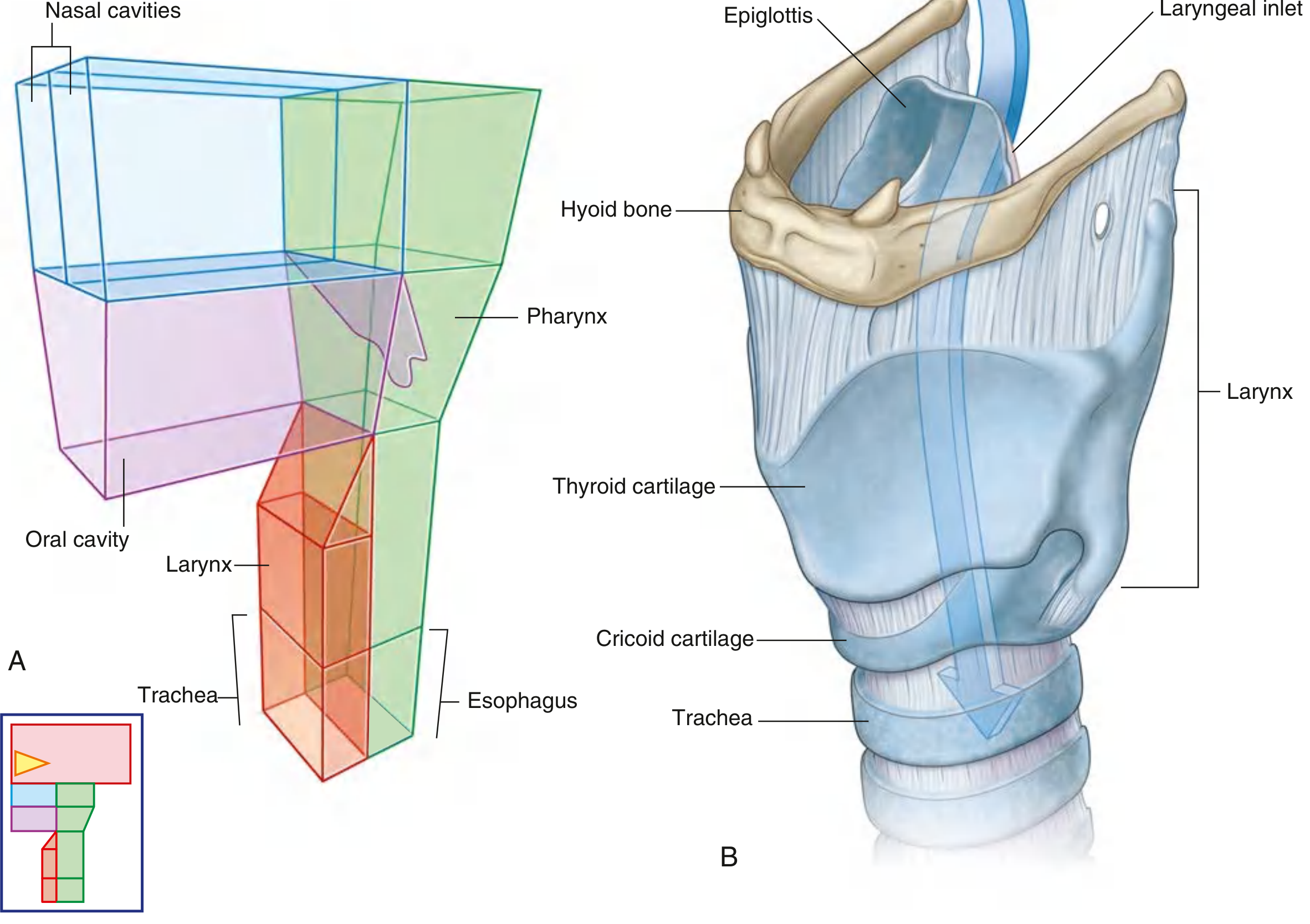
1) Clinical anatomy of the larynx
- The larynx is a hollow musculoligamentous organ connecting pharynx to trachea, acting as:
- airway sphincter/protector
- phonatory organ (voice production)
(Gray’s Anatomy for Students, p. 1192)
- Framework:
- Unpaired cartilages: thyroid, cricoid, epiglottis
- Paired cartilages: arytenoid, corniculate, cuneiform
(Gray’s Anatomy for Students, p. 1192 to 1193)
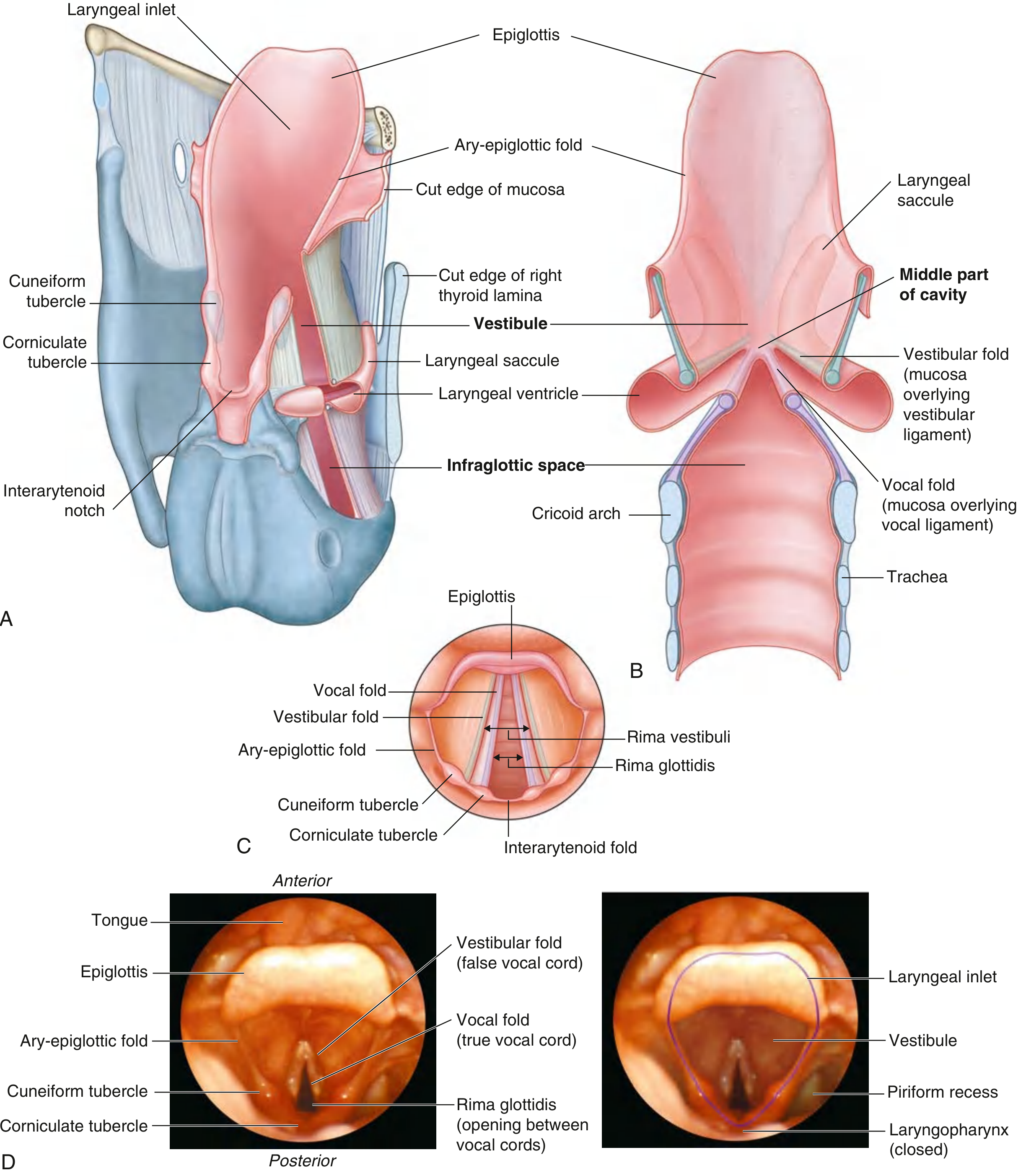
- Cavity is divided into:
- vestibule
- middle compartment (with ventricles/saccules)
- infraglottic space
- with rima vestibuli and rima glottidis as key airway openings
(Gray’s Anatomy for Students, p. 1199 to 1200)
- Key innervation:
- Vagus (X) provides motor and sensory innervation
- Recurrent laryngeal nerve supplies most intrinsic muscles
(Gray’s Anatomy for Students, p. 1192, 1203)
2) Physiology of the larynx
- Respiration: vocal folds abduct, glottic opening widens (especially in forced inspiration via posterior cricoarytenoid action).
- Phonation: vocal folds adduct; airflow induces vibration; tension is adjusted by vocalis/cricothyroid activity.
- Airway protection/swallowing: larynx elevates and moves anteriorly; epiglottis tilts toward arytenoids; inlet narrows/closes to prevent aspiration.
- Effort closure (Valsalva-related): complete closure of glottis and vestibule for trunk stabilization/intra-abdominal pressure generation.
(Gray’s Anatomy for Students, p. 1203 to 1204)
3) Methods of larynx research/examination (clinical)
Core modern methods include:
- Flexible fiberoptic laryngoscopy
- first-line dynamic visualization of supraglottis/glottis/subglottis
- gold standard in suspected epiglottitis/supraglottitis
(Rosen’s Emergency Medicine, p. 959)
- Imaging (CT/MRI)
- CT useful for trauma, fractures, deep spread, airway compromise
- MRI/contrast CT for deep tissue invasion and staging when tumors suspected
(Cummings Otolaryngology Head and Neck Surgery, p. 180)
- Plain lateral neck radiograph
- supportive signs like enlarged epiglottis (“thumb sign”) in epiglottitis; moderate sensitivity only
(Rosen’s Emergency Medicine, p. 959)
- supportive signs like enlarged epiglottis (“thumb sign”) in epiglottitis; moderate sensitivity only
- Functional voice studies (in routine ENT practice): stroboscopy, acoustic analysis, aerodynamic measures
- Histopathology/microbiology when indicated for infectious or neoplastic differentials
Acute diseases of the larynx
A) Acute laryngitis and laryngeal edema
- Acute diffuse inflammation is commonly viral; can also be bacterial, allergic, chemical, thermal, traumatic, reflux-related.
- Clinical features: sore throat, hoarseness, barking cough, inspiratory stridor, fever.
- Edema in the supraglottic/glottic region can acutely narrow airway, especially in children (small-caliber airway).
(Rosen’s Emergency Medicine, p. 958 to 959; Robbins Pathologic Basis of Disease, p. 691 to 692) - Management principles:
- airway assessment first
- many mild cases self-limited
- steroids may reduce symptom severity in selected cases
- urgent escalation if signs of obstruction/supraglottitis coexist
(Rosen’s Emergency Medicine, p. 959)
B) Laryngeal edema (focused)
Definition: pathologic swelling of laryngeal soft tissues (often supraglottic and aryepiglottic structures) causing variable obstruction.
Causes:
- infectious (laryngitis, epiglottitis)
- allergic/angioedema
- inhalational/thermal injury
- trauma/instrumentation
- toxin-related inflammation, reflux, systemic reactions
Danger signs (threatened airway):
- stridor at rest
- drooling/inability to handle secretions
- tripod/sniffing posture
- tachypnea, hypoxia, voice change with progressive dyspnea
Management priorities:
- immediate airway risk stratification
- oxygen + monitored setting
- early ENT/anesthesia involvement
- pharmacologic edema control (steroids ± nebulized epinephrine in selected protocols)
- early controlled intubation if deterioration is likely; surgical airway backup
(Rosen’s Emergency Medicine, p. 959)
C) Laryngeal stenosis
Definition: fixed narrowing of the laryngeal lumen (supraglottic, glottic, or subglottic), acute or chronic.
Etiologic categories:
- congenital
- post-intubation/post-tracheostomy scar
- inflammatory/infectious
- autoimmune
- traumatic/iatrogenic
- neoplastic
Clinical clues:
- biphasic stridor, exertional dyspnea
- persistent hoarseness
- recurrent “asthma-like” symptoms not responding to bronchodilators
Evaluation:
- endoscopic grading (site/length/severity)
- cross-sectional imaging when complex/combined airway lesions are suspected
Treatment:
- acute critical narrowing: secure airway first
- endoscopic options: dilation, scar incision, steroid/adjunctive therapy
- open reconstruction or segmental surgery for severe/refractory disease
- tracheostomy in selected unstable or non-reconstructible settings
D) Diphtheria of the larynx
- Respiratory diphtheria classically forms an adherent pseudomembrane that bleeds on attempted removal.
- Laryngeal involvement presents with hoarseness, stridor, cough, and may progress to respiratory compromise.
- “Bull neck” reflects cervical lymphadenopathy plus soft tissue edema.
- Airway obstruction risk is high; toxin-related systemic complications (myocarditis, neuropathy) are major mortality drivers.
(Goldman-Cecil Medicine, p. 3067)
Management essentials:
- isolation and airway monitoring
- early diphtheria antitoxin (do not delay if strongly suspected)
- antibiotics (e.g., erythromycin or penicillin per protocol)
- airway intervention if obstruction evolves
- contact management and vaccination/public health action
High-yield differential points (exam style)
- Croup: barking cough, usually viral, subglottic predominance, pediatric
- Epiglottitis/supraglottitis: severe sore throat, dysphagia, drooling, toxic appearance, rapid airway risk
- Diphtheria: adherent gray pseudomembrane + toxin-mediated complications
- Laryngeal edema (noninfectious): consider angioedema/anaphylaxis/thermal injury urgently
Useful anatomy figures
If you want, I can convert this into a concise oral-exam answer format (2 to 3 minutes) or a comparison table (acute laryngitis vs epiglottitis vs diphtheritic laryngeal involvement vs stenosis).
Clinical anatomy. physiology and methods of larynx research. Acute diseases of the larynx. Laryngeal edema. 1.aryngeal stenosis. Diphtheria of the larynx
Clinical anatomy. physiology and methods of larynx research. Acute diseases of the larynx. Laryngeal edema. 1.aryngeal stenosis. Diphtheria of the larynx. Detail explanation
1) Clinical anatomy of the larynx
The larynx is a mobile, musculocartilaginous organ between the pharynx and trachea (approximately C3 to C6 in adults). It has 3 core functions: airway patency, airway protection, and phonation.
A. Cartilaginous skeleton
Unpaired cartilages
- Thyroid cartilage
- Largest; two laminae fused anteriorly (laryngeal prominence).
- Superior/inferior horns articulate with hyoid/cricoid-related structures.
- Cricoid cartilage
- Signet-ring shape; only complete cartilaginous ring of upper airway.
- Critical in subglottic framework and stenosis.
- Epiglottis
- Elastic cartilage leaf; contributes to laryngeal inlet closure during swallowing.
Paired cartilages
- Arytenoid (vocal process + muscular process; key for fold movement)
- Corniculate
- Cuneiform
B. Joints
- Cricothyroid joint: tilting/gliding of thyroid on cricoid, changes vocal fold tension (pitch).
- Cricoarytenoid joints: arytenoid rotation/gliding for abduction/adduction of vocal folds.
C. Ligaments and membranes
- Thyrohyoid membrane
- Cricotracheal ligament
- Fibroelastic membrane with:
- Conus elasticus (upper free edge forms vocal ligament)
- Quadrangular membrane (forms vestibular ligament)
D. Cavities/regions
- Supraglottis: epiglottis, aryepiglottic folds, false cords, ventricles
- Glottis: true vocal folds + anterior/posterior commissures
- Subglottis: below true cords to lower cricoid border
Important openings:
- Rima glottidis between true cords
- Rima vestibuli between vestibular folds
E. Muscles
Intrinsic muscles (control laryngeal airway and voice)
- Posterior cricoarytenoid: only abductor of vocal folds (opens glottis)
- Lateral cricoarytenoid + interarytenoids: adductors
- Cricothyroid: tenses/elongates folds (raises pitch)
- Thyroarytenoid/vocalis: relax/fine-tune folds
Extrinsic muscles move larynx as a unit during swallowing/phonation.
F. Innervation and blood supply
- Vagus (X)
- Superior laryngeal nerve
- Internal branch: supraglottic sensation
- External branch: motor to cricothyroid
- Recurrent laryngeal nerve: motor to all other intrinsic muscles + sensation below cords
- Superior laryngeal nerve
- Blood: superior/inferior laryngeal arteries (from superior/inferior thyroid systems)
2) Physiology of the larynx
A. Respiration
- During quiet breathing, vocal folds are partially abducted.
- During inspiration, especially forced inspiration, posterior cricoarytenoids widen glottis.
B. Phonation
- Adducted folds vibrate with expiratory airflow (myoelastic-aerodynamic mechanism).
- Frequency (pitch): mainly fold tension/length/mass.
- Intensity: subglottic pressure.
- Resonance/articulation modified by pharynx, oral and nasal cavities.
C. Airway protection/swallowing
- Larynx elevates and moves anteriorly.
- Epiglottis and aryepiglottic structures redirect bolus.
- Reflex adduction closes glottis.
- Cough reflex clears aspirate.
D. Effort closure
- Tight closure of glottis for Valsalva-type maneuvers (lifting, defecation, childbirth).
3) Methods of larynx research (examination/investigation)
A. Clinical assessment
- Voice change, stridor, dyspnea, dysphagia, odynophagia, cough, aspiration history.
- Red flags: stridor at rest, drooling, tripod posture, cyanosis, rapidly progressive symptoms.
B. Endoscopic methods
- Indirect mirror laryngoscopy (basic)
- Flexible nasolaryngoscopy (office gold standard for dynamic evaluation)
- Rigid laryngoscopy (high-definition view)
- Microlaryngoscopy under GA (diagnostic + therapeutic)
- Stroboscopy (mucosal wave and subtle vibratory pathology)
C. Imaging
- Lateral neck radiograph (e.g., epiglottic “thumb sign,” subglottic narrowing)
- CT neck (airway caliber, abscess, trauma, stenosis length, tumor extension)
- MRI (soft tissue and cartilage invasion when indicated)
- Ultrasound (limited but useful in selected neck/airway contexts)
D. Functional/lab studies
- Acoustic voice analysis, aerodynamic tests, laryngeal EMG (neuromuscular disorders)
- Microbiology (throat swab/culture/PCR where relevant)
- Biopsy/histopathology for suspicious lesions
4) Acute diseases of the larynx (overview)
- Acute viral/bacterial laryngitis
- Supraglottitis/epiglottitis
- Croup (acute laryngotracheobronchitis, mostly pediatric)
- Laryngeal edema (infectious, allergic, traumatic, thermal, toxic)
- Acute laryngeal trauma/inhalational injury
- Acute airway obstruction from foreign body, abscess extension, diphtheria membrane
- Decompensated laryngeal stenosis
Common symptom cluster: hoarseness + stridor + cough + dyspnea.
Management priority is always airway first.
Management priority is always airway first.
5) Laryngeal edema (detailed)
A. Definition
Excess fluid/inflammatory swelling in laryngeal tissues (often supraglottic and/or glottic), causing variable airway narrowing.
B. Causes
- Infectious: laryngitis, epiglottitis
- Allergic/immunologic: angioedema, anaphylaxis
- Traumatic/iatrogenic: intubation injury, surgery
- Thermal/chemical: smoke, caustic inhalation
- Systemic: severe reflux-related inflammation, renal/cardiac causes (less direct but contributory)
- Neoplastic/radiation-associated
C. Pathophysiology
- Increased vascular permeability + venous/lymphatic congestion
- Loose supraglottic tissue swells rapidly
- Even small edema causes major resistance increase, especially in children
D. Clinical features
- Hoarseness, muffled voice
- Inspiratory stridor
- Dyspnea, tachypnea
- Dysphagia/odynophagia, drooling
- Retractions, anxiety, hypoxemia in severe cases
E. Diagnosis
- Primarily clinical + flexible laryngoscopy if safe
- Avoid provoking airway collapse in unstable patients
- Imaging only when stable and it will change management
F. Emergency management
- High-flow oxygen, continuous monitoring
- Early airway team (ENT + anesthesia)
- Dexamethasone commonly used
- Nebulized epinephrine in selected obstructive edema
- Treat cause:
- anaphylaxis: IM epinephrine + protocol-based care
- infection: antibiotics
- trauma/burn: airway protection + critical care
- Controlled intubation early if deterioration risk; surgical airway backup ready
Complications: complete obstruction, hypoxic injury, arrest.
6) Laryngeal stenosis (detailed)
(You wrote “1.aryngeal stenosis,” interpreted as laryngeal stenosis.)
A. Definition
Fixed narrowing of laryngeal lumen (supraglottic, glottic, subglottic; sometimes combined laryngotracheal stenosis).
B. Classification
- By site: supraglottic, glottic, subglottic
- By cause: congenital vs acquired
- By severity: percent obstruction (endoscopic grading systems)
- By length and maturity: short/long segment, soft/inflammatory vs mature scar
C. Etiology
- Prolonged intubation (most common acquired cause)
- Tracheostomy-related injury
- External laryngeal trauma
- Infection/inflammation (including historic diphtheritic scarring)
- Autoimmune disease (e.g., GPA-related airway stenosis)
- Reflux-associated chronic injury
- Radiation, caustic injury
- Tumor/postoperative scarring
D. Pathogenesis
Mucosal ischemia/ulceration → chondritis/perichondritis → granulation → fibrosis/cicatrix → fixed narrowing.
E. Clinical picture
- Progressive exertional dyspnea
- Biphasic stridor (often fixed lesion)
- Voice change (if glottic involvement)
- Chronic cough, recurrent “asthma” not responding to bronchodilators
F. Workup
- Flexible and direct laryngoscopy
- Bronchoscopy to define distal extent
- CT neck/chest for length, wall involvement, associated pathology
- Pulmonary function loop may show fixed upper airway obstruction pattern
G. Treatment
Acute decompensation
- Airway stabilization first (intubation/tracheostomy depending on anatomy and urgency)
Definitive
- Endoscopic dilation (balloon/bougie)
- Laser or cold incision of scar webs
- Adjuncts (intralesional steroid, selected anti-fibrotic approaches)
- Open reconstruction for complex disease:
- laryngotracheal reconstruction
- cricotracheal resection/anastomosis
- Decannulation strategy after lumen stabilization and functional assessment
7) Diphtheria of the larynx (detailed)
A. Etiology
- Toxigenic Corynebacterium diphtheriae (less commonly related Corynebacterium species)
- Disease severity is toxin-dependent
B. Transmission/incubation
- Respiratory droplets, close contact
- Incubation usually 2 to 5 days (range around 1 to 10)
C. Local pathology
- Adherent gray-white pseudomembrane on inflamed mucosa
- Membrane bleeds on forced removal
- Can extend from pharynx to larynx and tracheobronchial tree
D. Laryngeal involvement
- Hoarseness, barking cough, stridor, dyspnea
- Cervical adenopathy and edema may produce “bull neck”
- Major risk: progressive upper airway obstruction
E. Systemic toxicity
- Myocarditis: arrhythmia, conduction block, heart failure
- Neuropathy: cranial/peripheral motor deficits, palatal/pharyngeal/laryngeal weakness
- Toxic effects may appear even as local throat findings begin to improve
F. Diagnosis
- Clinical suspicion is critical; do not wait for lab confirmation to start antitoxin
- Throat/nasopharyngeal swab for culture/PCR and toxigenicity testing
- ECG and cardiac monitoring for toxin effects
G. Treatment
- Airway first
- Immediate diphtheria antitoxin (after sensitivity/risk protocol per local guidance)
- Antibiotics: penicillin or erythromycin-class regimens per guideline
- Droplet/contact isolation
- ICU-level monitoring if airway or systemic toxicity risk
- Public health notification, contact tracing, prophylaxis, and vaccination update
H. Prevention
- Full immunization (DTP/DTaP/Tdap schedules + boosters) is the key preventive measure.
8) Practical emergency algorithm for acute laryngeal pathology
- Assess airway severity immediately (stridor at rest, SpO2, work of breathing, secretions).
- Call airway team early if any concern.
- Keep patient calm/upright; avoid unnecessary throat manipulation.
- Give cause-directed early therapy (steroid, epinephrine nebulization, antibiotics, antitoxin, anaphylaxis protocol).
- Secure airway in controlled setting before exhaustion/crash obstruction.
- After stabilization, complete etiologic workup and definitive treatment plan.
If you want, I can next provide:
- a one-page exam note version,
- a comparison table (laryngitis vs epiglottitis vs croup vs diphtheria vs stenosis),
- or MCQ-style viva questions with answers on this topic.
This is a shared conversation. Sign in to Orris to start your own chat.