

History of abdominal pain and bulging of abdomen
Reading File
search_medical_text
complex ovarian cyst internal septations management workup
search_medical_text
left ovarian cyst abdominal pain bloating 42 year old female differential diagnosis
search_medical_image
complex ovarian cyst ultrasound internal septations
GradeResponse
GradeResponse
GradeResponse
USG Whole Abdomen — Interpretation & Clinical Correlation
Patient: Tej Rani | Female, 42 years | Date: 25/03/2026
Presenting complaints: Abdominal pain + abdominal bulging
Key Finding
Left ovarian complex cyst — a loculated fluid collection measuring 8.85 cm × 8.48 cm with internal septations.
This is a large adnexal mass. At 42 (perimenopausal age), this finding warrants urgent further evaluation.
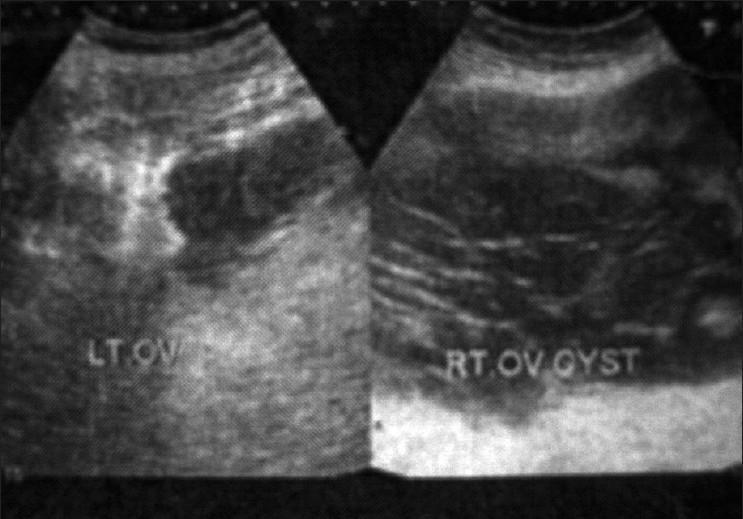
Ultrasound Image Comparison
The image below shows how a multiloculated ovarian cyst with internal septations appears on ultrasound — similar to what is described in this report:
What Makes This Cyst "Complex"?
A complex cyst differs from a simple cyst by having one or more of:
- Internal septations (dividing walls) ✅ — present here
- Loculated fluid ✅ — present here
- Solid components, mural nodules, or papillations (not mentioned — reassuring)
The absence of free fluid in the cul-de-sac and no solid components are relatively reassuring signs, but the large size (>7 cm) + septations + age >40 make this a cyst that must be assessed for malignancy risk.
Differential Diagnoses
| Diagnosis | Features Supporting | Features Against |
|---|---|---|
| Ovarian cystadenoma (serous or mucinous) | Large size, septations, loculated, common at this age | — |
| Endometrioma | Pelvic pain, age group | No "ground glass" echogenicity mentioned |
| Tubo-ovarian cyst / hydrosalpinx | Can be septated | USG can help differentiate with 3D |
| Dermoid cyst (teratoma) | Common in reproductive age | No echogenic foci/fat-fluid level mentioned |
| Ovarian malignancy | Age >40, large cyst, septations | No solid nodules, no free fluid — lower suspicion, but must rule out |
The most likely diagnoses are serous or mucinous cystadenoma, but malignancy cannot be excluded on USG alone (Bailey & Love's, p. 1613).
Recommended Next Steps
1. Tumour Markers (Blood Tests) — Urgent
- CA-125 — elevated in ovarian cancer, also in endometriosis, fibroids
- CEA, CA 19-9 — for mucinous tumours
- HE4 — more specific than CA-125 for epithelial ovarian cancer
- ROMA score (combines CA-125 + HE4 + menopausal status) — risk stratification
2. Imaging
- Transvaginal ultrasound (TVS) — better resolution than transabdominal for ovarian masses; can assess septation thickness, vascularity (Doppler), and solid components
- Contrast-enhanced MRI pelvis — gold standard to characterize complex adnexal masses; distinguishes benign from malignant features better than CT
- CT abdomen & pelvis — if malignancy suspected, to assess for peritoneal deposits, lymph nodes, ascites
3. Gynaecology Referral — Urgent
- A 42-year-old with a >8 cm complex septated ovarian cyst requires gynecologic oncology evaluation
- Risk of Malignancy Index (RMI) should be calculated using USG score, menopausal status, and CA-125
4. IOTA Classification (ultrasound-based)
Per performance guidelines (IOTA/ACRP), a detailed re-evaluation should document:
- Septation thickness (thin <3 mm vs thick ≥3 mm)
- Presence/absence of papillary projections or solid areas
- Doppler vascularity pattern
Symptoms Explained
| Symptom | Mechanism |
|---|---|
| Abdominal pain | Capsular distension, pressure on adjacent structures, possible intermittent torsion |
| Abdominal bulging | An ~8.8 cm cyst is clinically palpable and can cause visible distension |
Bottom Line
This is a large complex left ovarian cyst that requires prompt gynaecology referral. The radiologist's advice — "correlate clinically and further investigation" — is appropriate. Do not delay CA-125, TVS, and a specialist consultation. Most such cysts in this age group are benign cystadenomas, but the possibility of malignancy must be formally excluded.
⚠️ This analysis is for informational purposes only and does not replace evaluation by a qualified gynaecologist or oncologist.
This is a shared conversation. Sign in to Orris to start your own chat.