Give answers for theory exam in PSM for third MBBS level. The answer should be pinned to point and grips important points, no extra information. Give answer based on all available standard resources and remember that the answer should be an examiner pleaser, not so examiner can see the important points easily and highlight important points and all, make a structure so it will be easy for examiner to scan the answers easily and also important point and answer should be writable in a 10 to 12 minutes assuming the speed of writing is moderate. The first topic is human development index. Use mind maps diagram and flow charts where ever. Necessary
human development index PSM community medicine third MBBS exam answer components HDI UNDP
Human Development Index (HDI)
1. DEFINITION ⭐
HDI is a composite index measuring achievement in three basic dimensions of human development: Long healthy life + Knowledge + Decent standard of living
- Introduced by UNDP (United Nations Development Programme)
- Values range from 0 to 1 (higher = better development)
2. DIMENSIONS & INDICATORS (FLOWCHART from Park's)
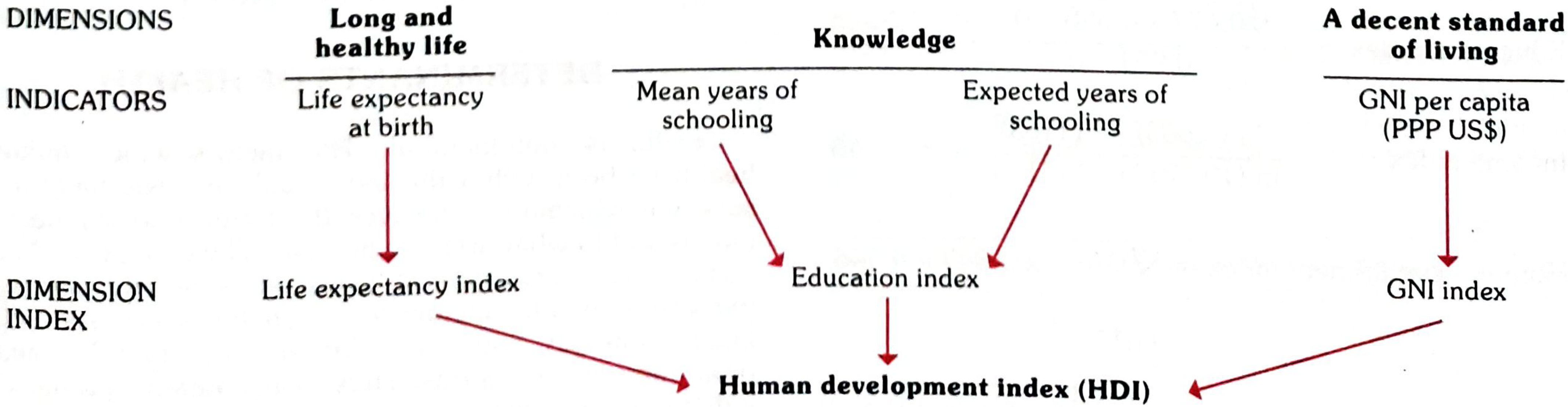
DIMENSION INDICATOR(S)
─────────────────────────────────────────────────────
Long & Healthy Life Expectancy at Birth
Life ↓
Life Expectancy Index
─────────────────────────────────────────────────────
Knowledge Mean Years of Schooling (adults ≥25 yrs)
+ Expected Years of Schooling (school-entering age)
↓
Education Index
─────────────────────────────────────────────────────
Decent Standard GNI per capita (PPP US $)
of Living ↓
GNI Index
─────────────────────────────────────────────────────
↓↓↓
[GEOMETRIC MEAN of all 3]
↓
HUMAN DEVELOPMENT INDEX
3. STEPS TO CALCULATE HDI
Step 1 - Create Dimension Index (Sub-index)
Dimension Index = (Actual value - Minimum value)
─────────────────────────────────
(Maximum value - Minimum value)
Step 2 - Calculate HDI
HDI = Geometric Mean of 3 Dimension Indices
= (Life Expectancy Index × Education Index × GNI Index)^(1/3)
Note: For Education, geometric mean of the two sub-indices is taken first, then equation re-applied.
4. GOALPOSTS (Min & Max Values) - TABLE ⭐
| Dimension | Indicator | Maximum | Minimum |
|---|---|---|---|
| Health | Life expectancy (yrs) | 83.2 | 20 |
| Education | Mean yrs of schooling | 13.2 | 0 |
| Education | Expected yrs of schooling | 20.6 | 0 |
| Education | Combined Education Index | 0.951 | 0 |
| Standard of Living | GNI per capita (PPP $) | 1,08,211 | 163 |
5. HDI CLASSIFICATION - MIND MAP
HDI VALUE
│
┌────────────┼────────────┬────────────┐
│ │ │ │
<0.550 0.550-0.699 0.700-0.799 ≥0.800
│ │ │ │
LOW MEDIUM HIGH VERY HIGH
HDI HDI HDI HDI
6. KEY FACTS FOR EXAM ⭐⭐
| Point | Fact |
|---|---|
| Introduced by | UNDP |
| Year first published | 1990 |
| Range | 0 to 1 |
| Calculation method | Geometric mean (NOT arithmetic) |
| Income measure used | GNI per capita in PPP US$ |
| India's rank (2018) | 129th - Medium HDI category |
| Top countries (2018) | Norway, Ireland, Switzerland |
| Bottom countries (2018) | Niger, Central African Republic |
7. IMPORTANCE / SIGNIFICANCE
- More comprehensive than per capita income alone
- Income is a means, not an end - HDI goes beyond income
- Focuses on human outcomes rather than economic statistics
- Two countries with same income can have very different HDI (e.g., different life expectancy/literacy)
- Used by policy makers, media, NGOs to direct interventions
- Highlights regional disparities in human development
8. LIMITATIONS (Bonus if time permits)
- Does not capture inequality within countries
- Does not reflect gender disparities (separate Gender Development Index exists)
- Does not include environmental sustainability
- Only 4 indicators - oversimplified
Source: Park's Textbook of Preventive and Social Medicine (reference standard for MBBS PSM)
Iceberg phenomenon of disease
Iceberg Phenomenon of Disease
1. CONCEPT / DEFINITION ⭐
Disease in a community can be compared to an iceberg - only the tip is visible above the waterline, while the vast mass remains hidden below.
- The pattern of disease in hospitals is very different from the pattern in the community
- A far larger proportion of disease is hidden from view than is evident to physicians or the general public
- Closely related to the Spectrum of Disease
2. THE ICEBERG DIAGRAM (Park's Fig. 10) ⭐⭐
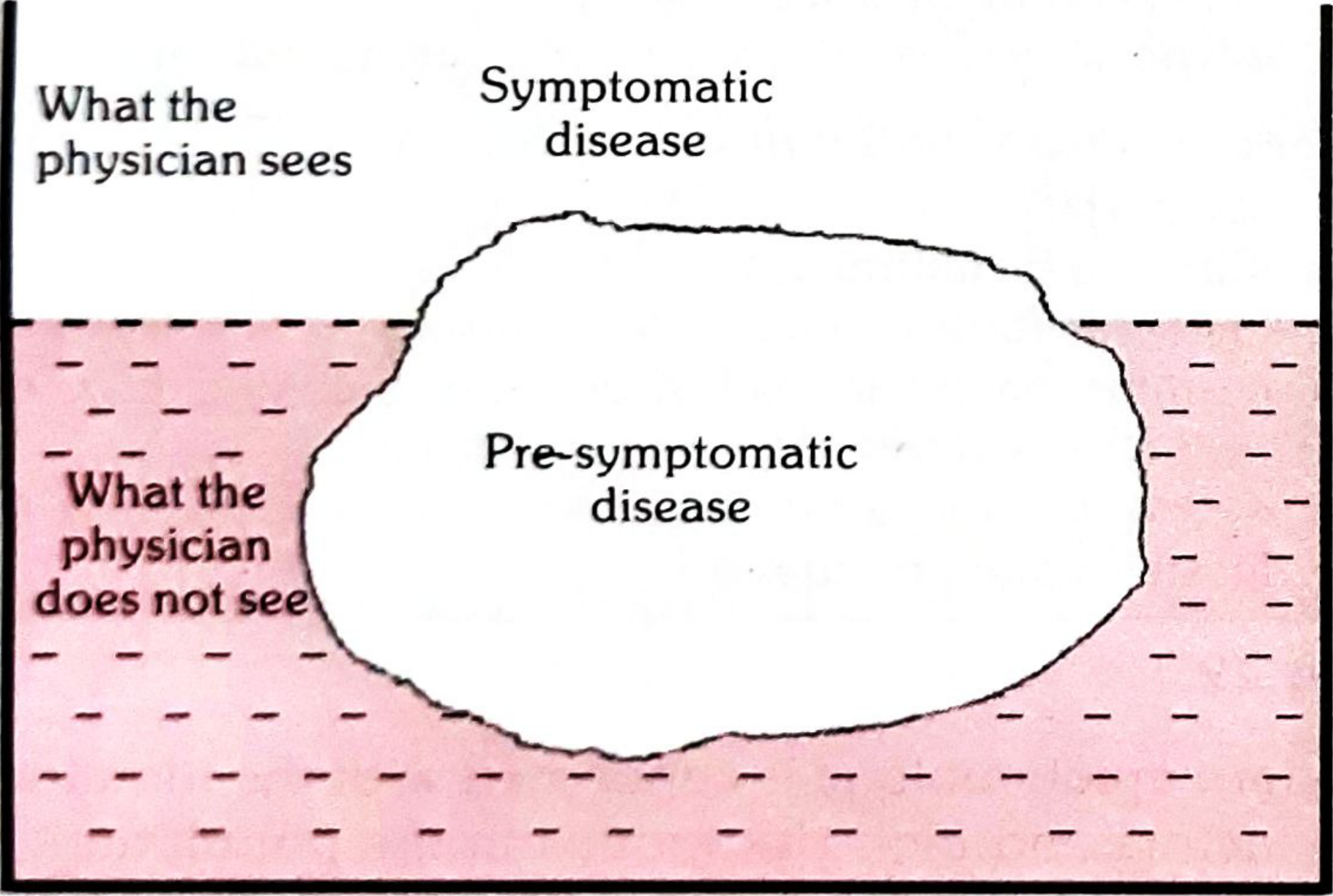
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
▲ FLOATING TIP (VISIBLE)
| → Symptomatic / Clinical disease
| → What the PHYSICIAN SEES
═══════╪══════════════ WATERLINE ═════════════
| → Apparent ←→ Inapparent demarcation
|
▼ SUBMERGED PORTION (HIDDEN MASS)
→ Subclinical cases
→ Carriers
→ Latent cases
→ Presymptomatic cases
→ Undiagnosed cases
→ What the PHYSICIAN DOES NOT SEE
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━
3. COMPONENTS OF THE ICEBERG - MIND MAP
ICEBERG OF DISEASE
│
┌───────────────┴────────────────┐
ABOVE WATERLINE BELOW WATERLINE
(Apparent Disease) (Inapparent Disease)
│ │
┌─────┤ ┌──────────┼──────────────┐
Clinical │ Subclinical Latent Carriers
cases │ infections cases │
│ │ │ │ (e.g., Typhoid,
Mild Severe No symptoms Dormant Hepatitis B)
cases cases yet infection │
Presymptomatic
cases
4. EXAMPLES BY DISEASE ⭐⭐
| Disease | Clinical (Tip) | Subclinical (Hidden) | Ratio |
|---|---|---|---|
| Poliomyelitis | Paralytic cases | Inapparent infections | 1 : 1000 (children) |
| Hypertension | Known cases | Undiagnosed cases | Large hidden portion |
| Diabetes | Diagnosed | Undiagnosed | Huge hidden mass |
| TB | Active cases | Latent TB infection | ~1.7 billion latent globally |
| Anaemia | Known | Undetected | Large hidden portion |
| Mental illness | Treated | Untreated/undiagnosed | Vast hidden mass |
| Malnutrition | Severe/obvious | Mild/moderate | Hidden portion larger |
5. SIGNIFICANCE / IMPORTANCE ⭐
- Reservoir of infection - hidden cases act as undetected source of spread
- True burden underestimated - hospital/clinic data does not reflect community disease load
- Basis for Screening - justifies active search for disease in apparently healthy individuals
- Public health challenge - detection and control of hidden portion is the goal of preventive medicine
- Epidemiological tool - explains why incidence > reported cases
6. WATERLINE = KEY CONCEPT
ABOVE WATERLINE BELOW WATERLINE
───────────────────── ─────────────────────────────
Apparent disease Inapparent disease
Diagnosed cases Undiagnosed / subclinical
Physician sees Physician does NOT see
Morbidity statistics capture These are MISSED in data
7. RELATIONSHIP WITH SPECTRUM OF DISEASE
SPECTRUM OF DISEASE (Continuous)
├── Subclinical/Inapparent ──── [BELOW waterline = Iceberg base]
├── Mild illness
├── Moderate illness [ABOVE waterline = Iceberg tip]
├── Severe illness
└── Death
The Iceberg concept gives a better picture of sub-clinical to overt disease progression than the spectrum of disease alone.
8. SOLUTION TO THE ICEBERG PROBLEM ⭐
DETECTION OF HIDDEN DISEASE
│
├── SCREENING PROGRAMMES
│ (mass/selective/multiphasic)
│
├── ACTIVE SURVEILLANCE
│
├── COMMUNITY SURVEYS
│
└── HEALTH CAMPS / OUTREACH
Screening = "search for unrecognized disease by rapidly applied tests in apparently healthy individuals" - this directly addresses the submerged portion of the iceberg.
Epidemiological triad
Epidemiological Triad
1. INTRODUCTION / BACKGROUND ⭐
- The Germ Theory of disease (single cause) was found insufficient
- Example: Not everyone exposed to TB bacilli develops TB - host and environment also matter
- This demanded a broader concept synthesizing Agent + Host + Environment
- The Epidemiological Triad is based on the communicable disease model
2. THE TRIAD DIAGRAM ⭐⭐ (Draw in exam)
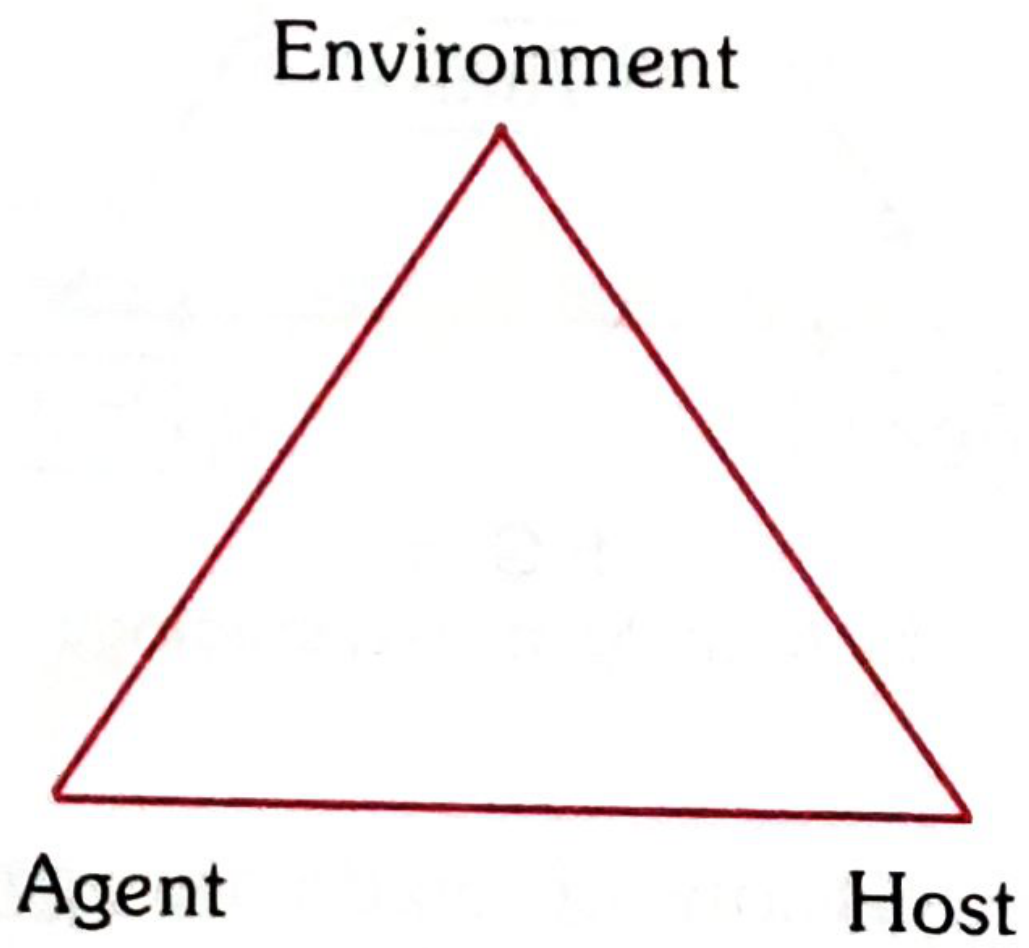
ENVIRONMENT
/\
/ \
/ \
/ \
/________\
AGENT HOST
Disease occurs when the BALANCE between the three is disturbed Prevention = Break one leg of the triangle
3. COMPONENT 1 - AGENT ⭐⭐
The cause of disease
Classification of Agents:
AGENT
│
┌─────────────────┼──────────────────┐
BIOLOGICAL PHYSICAL CHEMICAL
│ │ │
Bacteria Radiation Poisons/toxins
Viruses Heat/cold Drugs
Fungi Trauma Allergens
Parasites Noise Nutritional
Rickettsia deficiency/excess
Helminths
Properties of Agent (Biological) - KEY POINTS:
| Property | Definition |
|---|---|
| Infectivity | Ability to enter and establish in host |
| Pathogenicity | Ability to produce disease in infected host |
| Virulence | Severity of disease produced |
| Antigenicity | Ability to produce immune response |
| Invasiveness | Ability to invade tissues |
| Toxigenicity | Ability to produce toxins |
4. COMPONENT 2 - HOST ⭐⭐
An organism (usually human/animal) that harbours the disease
Host Factors (Mind Map):
HOST FACTORS
│
┌──────────┬──────────┼──────────┬────────────┐
INTRINSIC GENETIC IMMUNO- BEHAV- NUTRI-
FACTORS MAKEUP LOGICAL IOURAL TIONAL
│ │ STATUS FACTORS STATUS
Age Race │ │ │
Sex Sickle cell Immunity Lifestyle Under/over
Ethnicity trait Natural Habits nutrition
HLA type Acquired Occupation
Key determinants: Age, Sex, Genetic constitution, Immunity, Nutrition, Behaviour, Occupation
5. COMPONENT 3 - ENVIRONMENT ⭐⭐
All external conditions and surroundings of the host that affect disease transmission
Three Types:
| Type | Examples |
|---|---|
| Biological | Vectors (mosquitoes, flies), reservoir hosts, food contamination |
| Physical | Climate, season, geography, temperature, radiation |
| Social/Psychosocial | Poverty, overcrowding, sanitation, education, culture, lifestyle |
6. ROLE OF TIME ⭐
- Added to create the "Triangle of Epidemiology" (Fig. 5, Park's)
- Accounts for:
- Incubation period
- Life expectancy of host/pathogen
- Duration of illness
- Epidemic threshold timing
7. DISEASE STATES - INTERACTION DIAGRAM
EQUILIBRIUM (No disease)
Agent ←──── balanced ────→ Host
↕
Environment
DISEASE OCCURS when:
┌──────────────────────────────────────────┐
│ Agent virulence ↑ │
│ OR Host resistance ↓ │
│ OR Environment favours agent over host │
└──────────────────────────────────────────┘
8. EXAMPLES OF TRIAD IMBALANCE
| Disease | Agent | Host factor | Environment |
|---|---|---|---|
| TB | M. tuberculosis | Malnutrition, immunosuppression | Overcrowding, poverty |
| Malaria | Plasmodium | No immunity, age | Stagnant water, vector habitat |
| Rheumatic fever | Strep pyogenes | Genetic susceptibility | Overcrowding, cold |
| CHD | Multiple | Genetics, age, sex | Sedentary lifestyle, diet |
9. LIMITATIONS OF THE TRIAD ⭐
- Suitable mainly for infectious diseases - less applicable to chronic/non-communicable diseases
- Does not show interaction and interdependence between factors (Web of Causation better for this)
- Does not account for multiple causation well
- Replaced/supplemented by: Web of Causation (MacMahon & Pugh) for chronic diseases
10. SIGNIFICANCE / USE
USES OF EPIDEMIOLOGICAL TRIAD
│
┌────┴────┐
│ │
Understanding Designing
disease INTERVENTIONS
causation │
├── Target AGENT (antibiotics, vaccines)
├── Target HOST (immunization, nutrition)
└── Target ENVIRONMENT (sanitation, vector control)
Key principle: Break ANY ONE leg of the triangle = disease prevented/controlled
Now these are concepts in PSM give all imp points in them revivable in half hour presentable manner
Concept one epidemiology
⚡ EPIDEMIOLOGY - 30-MIN RAPID REVISION SHEET
🔑 1. DEFINITION (Most important - learn verbatim)
"The study of the occurrence and distribution of health-related events, states, and processes in specified populations, including the study of the determinants influencing such processes, and the application of this knowledge to control relevant health problems." — IEA Definition (International Epidemiological Association)
🔑 2. THREE CORE COMPONENTS
EPIDEMIOLOGY
│
┌────────┼────────┐
│ │ │
FREQUENCY DISTRIBUTION DETERMINANTS
│ │ │
Rates & Person Causes/
Ratios Place Risk factors
Time
| Component | What it does |
|---|---|
| Disease Frequency | Rates, ratios - prevalence, incidence, death rates |
| Distribution | Person, Place, Time (3 P's) |
| Determinants | Biological, social, behavioural, economic, political factors |
🔑 3. AIMS (IEA - 3 Aims)
- Describe distribution and magnitude of health & disease in populations
- Identify aetiological factors (risk factors) in pathogenesis
- Provide data for planning, implementation, evaluation of health services
Ultimate aim: Eliminate/reduce health problems + Promote well-being of society
🔑 4. SCOPE OF EPIDEMIOLOGY
SCOPE OF EPIDEMIOLOGY
│
┌────┴────┬──────────┬──────────┐
│ │ │ │
Infectious Chronic Accidents Mental
Diseases Diseases Health
│ │
Endemic Non-communicable
Epidemic diseases (CHD, Ca)
│
Health services &
Health-related states
🔑 5. USES OF EPIDEMIOLOGY (Morris - 7 Uses) ⭐⭐
| # | Use | Key Point |
|---|---|---|
| 1 | History of disease | Rise & fall - emerging/disappearing diseases |
| 2 | Community diagnosis | Identify + quantify health problems; epidemiology = "diagnostic tool of community medicine" |
| 3 | Planning & Evaluation | Rational resource allocation; evaluate services by RCTs |
| 4 | Individual risk assessment | Relative risk, attributable risk (e.g., smoker vs non-smoker) |
| 5 | Syndrome identification | Define/refine syndromes by group observation |
| 6 | Natural history of disease | Complete the disease picture beyond hospital data |
| 7 | Searching for causes/risk factors | Identify aetiology → prevention strategies |
Mnemonic: History Community Planning Risk Syndrome Natural Causes = HCP RS NC
🔑 6. TYPES OF EPIDEMIOLOGY
EPIDEMIOLOGY
│
┌────┴────────────┐
│ │
DESCRIPTIVE ANALYTICAL
│ │
Person ├── Case-control study
Place ├── Cohort study
Time └── Cross-sectional study
│ │
Generates Tests hypothesis
Hypothesis
+
EXPERIMENTAL
│
├── RCT (gold standard)
├── Field trials
└── Community trials
🔑 7. DESCRIPTIVE EPIDEMIOLOGY - Person, Place, Time
PERSON
- Age, Sex, Race, Religion, Occupation, Marital status, Socioeconomic status
PLACE
- Country, Region, Urban vs Rural, Local patterns
TIME
- Secular trends - long-term changes over years/decades
- Cyclic trends - periodic fluctuations (seasonal, 2-3 yearly cycles)
- Point epidemic - all cases from single source at one time
- Propagated epidemic - spread person to person
🔑 8. EPIDEMIOLOGY vs CLINICAL MEDICINE
| Feature | Epidemiology | Clinical Medicine |
|---|---|---|
| Unit of study | Defined population | Individual patient/case |
| Concern | Sick + Healthy both | Sick only |
| Approach | Goes to community | Patient comes to doctor |
| Measure | Rate (cases/population) | Diagnosis + treatment |
| Purpose | Prevention + control | Cure of individual |
Key quote: "Clinician interested in cases; statistician in population; epidemiologist in the RATE (relationship between cases and population)"
🔑 9. BASIC MEASUREMENTS IN EPIDEMIOLOGY
RATES
│
├── INCIDENCE RATE = New cases / Population at risk × K
│ (measures risk of disease)
│
├── PREVALENCE RATE = All cases (new+old) / Total population × K
│ │
│ ├── Point prevalence (at one point in time)
│ └── Period prevalence (over a period)
│
└── ATTACK RATE = Cases / Population exposed × 100
(used in outbreaks/epidemics)
RELATIONSHIP:
Prevalence ≈ Incidence × Duration of disease
🔑 10. EPIDEMIOLOGICAL METHODS (Quick Overview)
OBSERVATIONAL EXPERIMENTAL
│ │
┌────┴────┐ ┌──────┴──────┐
DESC. ANALYTIC RCT Field/
│ │ (gold Community
Person ┌──┴──┐ standard) trials
Place │ │
Time Case Cohort
ctrl │
Retrospective Prospective
(exposure?) (disease?)
🔑 11. KEY TERMS TO REMEMBER
| Term | Definition |
|---|---|
| Incubation period | Time from exposure to onset of disease |
| Herd immunity | Resistance of a group to a disease when sufficient proportion immune |
| Endemic | Constant presence of a disease in a given area |
| Epidemic | Occurrence of disease in excess of normal expectancy |
| Pandemic | Worldwide epidemic |
| Sporadic | Occasional cases, no connection |
| Attack rate | Incidence rate used in epidemic situations |
⚡ RAPID RECALL - EXAM SHORTCUTS
DEFINITION = IEA = Occurrence + Distribution + Determinants + Application
AIMS = 3 (Describe + Identify + Provide data)
USES = 7 (Morris)
↓
H-C-P-R-S-N-C
TYPES = Descriptive → Analytical → Experimental
↓ ↓ ↓
Hypothesis Test it Prove it (RCT)
generated
PERSON + PLACE + TIME = 3 variables of descriptive epi
INCIDENCE = new cases (risk measure)
PREVALENCE = all cases (burden measure)
P = I × D
Communicable disease and related nhp in India
⚡ COMMUNICABLE DISEASES & NATIONAL HEALTH PROGRAMMES (NHP) IN INDIA
🔑 PART A: COMMUNICABLE DISEASE - CORE CONCEPTS
1. DEFINITION
A communicable disease is one that can be transmitted from an infected person/animal/environment to a susceptible host, directly or indirectly.
2. CHAIN OF INFECTION (Most Exam-Important Diagram) ⭐⭐
INFECTIOUS RESERVOIR PORT OF MODE OF PORT OF SUSCEPTIBLE
AGENT → OF EXIT → TRANS- → ENTRY → HOST
(pathogen) INFECTION MISSION
│ │ │ │ │ │
Bacteria Human Resp. Direct Resp. No immunity
Virus Animal tract Contact tract Malnutrition
Fungi Environment GIT Indirect GIT Genetic
Parasite Carrier Skin Airborne Skin Age/Sex
Rickettsia GUT Vector Mucosa
Vehicle
Fomite
Break ANY link = Disease prevented
3. MODES OF TRANSMISSION
| Type | Examples |
|---|---|
| Direct contact | STDs, Rabies, Ringworm |
| Droplet/Airborne | TB, Measles, COVID, Influenza |
| Faecal-oral (vehicle) | Cholera, Typhoid, Polio, Hepatitis A |
| Vector-borne | Malaria (Anopheles), Dengue (Aedes), Filaria (Culex) |
| Blood/parenteral | HIV, Hepatitis B, C |
| Vertical (mother to child) | HIV, Syphilis, Rubella, HBV |
4. KEY DEFINITIONS
| Term | Definition |
|---|---|
| Incubation period | Time from exposure to 1st symptom |
| Communicable period | Period when disease can be transmitted |
| Carrier | Infected person who harbours pathogen without symptoms |
| Herd immunity | Group protection when sufficient proportion immune |
| Zoonosis | Disease transmitted from animal to man |
| Notifiable disease | Must be reported to health authorities by law |
5. CONTROL OF COMMUNICABLE DISEASE
CONTROL MEASURES
│
┌────┴──────────────────────┐
│ │
AT SOURCE AT HOST AT ENVIRONMENT
(Agent/Reservoir) │ │
│ Immunization Sanitation
Isolation Chemoprophylaxis Safe water
Quarantine Health education Vector control
Disinfection Nutrition Waste disposal
Treatment Screening
🔑 PART B: NATIONAL HEALTH PROGRAMMES - COMMUNICABLE DISEASES ⭐⭐
MASTER TABLE OF NHPs FOR COMMUNICABLE DISEASES
| Programme | Year Started | Target Disease | Key Strategy |
|---|---|---|---|
| NTEP (earlier RNTCP/NTP) | 1962 (NTP), 1997 (RNTCP), renamed NTEP 2020 | Tuberculosis | DOTS |
| NVBDCP | 2003 (renamed from NAMP) | Malaria, Dengue, Filaria, Kala-azar, JE | Vector control + drug treatment |
| NLEP | 1983 | Leprosy | MDT |
| NACP | 1987 | HIV/AIDS | NACO, ART, Prevention |
| NPCB | 1976 | Blindness (Trachoma etc.) | Cataract surgery |
| National Immunization Programme | 1978 (EPI), 1985 (UIP) | Vaccine-preventable diseases | UIP/Mission Indradhanush |
🔑 1. NTEP - National TB Elimination Programme ⭐⭐
NTP (1962) → RNTCP (1997, DOTS) → End TB Strategy (2014) → NTEP (renamed 2020)
- Political will & administrative commitment
- Diagnosis by quality sputum smear microscopy
- Adequate supply of quality short-course chemotherapy
- Directly Observed Treatment (DOT)
- Systematic monitoring & accountability
- Address TB/HIV + MDR-TB
- Strengthen health systems
- Engage all care providers
- Empower patients & communities
- Enable/promote research
- Cure rate ≥ 85% of infectious cases
- Case detection ≥ 70% of estimated cases
Central TB Division (CTD) - National
↓
State TB Cell (STO) - State
↓
District TB Centre (DTO) - District
↓
Peripheral Health Institutions (PHI)
🔑 2. NVBDCP - National Vector Borne Disease Control Programme ⭐⭐
| Year | Event |
|---|---|
| 1953 | NMCP launched (75 million cases pre-1953) |
| 1958 | Renamed to NMEP (Eradication) |
| 1965 | Cases reduced to 0.1 million ✓ |
| 1970s | Resurgence of malaria |
| 1976 | Cases peaked at 6.46 million ✗ |
| 1999 | Renamed to NAMP |
| 2002 | Renamed to NVBDCP |
| 2016 | National Framework for Malaria Elimination launched |
| 2017 | National Strategic Plan for Malaria Elimination 2017-2022 |
- IRS (Indoor Residual Spraying) - DDT/Malathion
- LLINs (Long-lasting insecticidal bed nets) - introduced 2009
- RDT (Rapid Diagnostic Test) - introduced 2005
- ACT (Artemisinin Combination Therapy) - introduced 2006 for Pf resistance
- Larval control, biological control
🔑 3. NLEP - National Leprosy Eradication Programme ⭐
NLCP (1955) → NLEP (1983) → MDT introduced (1982 by WHO)
Goal: Elimination = <1 case per 10,000 population
India declared leprosy eliminated: 2005
| Type | Drugs | Duration |
|---|---|---|
| Paucibacillary (PB) | Dapsone + Rifampicin | 6 months |
| Multibacillary (MB) | Dapsone + Rifampicin + Clofazimine | 12 months |
🔑 4. NACP - National AIDS Control Programme ⭐⭐
1986: First HIV case in India
1987: NACP launched
NACO set up (under MoHFW)
| Phase | Year | Focus |
|---|---|---|
| NACP-I | 1992-1999 | Slow down spread of HIV |
| NACP-II | 1999-2006 | Behaviour change, decentralization, NGO involvement |
| NACP-III | 2007-2012 | Halt and reverse epidemic |
| NACP-IV | 2012-2017 | Accelerating response |
| NSP | 2017-2024 | Ending AIDS |
- 2004: ART (Antiretroviral Treatment) initiated free
- 2006: National Council on AIDS (PM as chairman)
- State AIDS Control Societies established in all states
- Prevent further HIV transmission
- Decrease morbidity & mortality
- Minimize socio-economic impact
🔑 5. NPCB - National Programme for Control of Blindness ⭐
- Launched: 1976 (100% centrally sponsored)
- Goal: Reduce blindness from 1.4% → 0.3%
- Current prevalence (2015-19 survey): 0.36%
- 66 lakh cataract operations/year
- 9 lakh free spectacles to school children/year
- 50,000 donated eyes for keratoplasty/year
🔑 6. UNIVERSAL IMMUNIZATION PROGRAMME (UIP) ⭐⭐
EPI (1978) → UIP (1985) → Mission Indradhanush (2014)
| Vaccine | Disease | Schedule |
|---|---|---|
| BCG | TB | Birth |
| OPV | Polio | 6, 10, 14 weeks + boosters |
| IPV | Polio | 6 & 14 weeks |
| Hepatitis B | Hep B | Birth, 6, 10, 14 weeks |
| DPT | Diphtheria, Pertussis, Tetanus | 6, 10, 14 weeks |
| Hib (Pentavalent) | H. influenzae b | 6, 10, 14 weeks |
| Measles/MR | Measles, Rubella | 9-12 months, 16-24 months |
| JE | Japanese Encephalitis | Selected districts |
| Rotavirus | Rotavirus diarrhoea | Selected states |
| PCV | Pneumococcal | 6, 14 weeks, 9 months |
| TT/Td | Tetanus | 10, 16 years + pregnant women |
⚡ RAPID RECALL TABLE - NHPs at a Glance
DISEASE PROGRAMME YEAR KEY STRATEGY
──────────────────────────────────────────────────
TB NTEP 1962/97 DOTS + End TB
Malaria NVBDCP 1953/02 ACT + LLINs + IRS
Leprosy NLEP 1983 MDT (6/12 months)
HIV/AIDS NACP/NACO 1987 ART + Prevention
Blindness NPCB 1976 Cataract surgery
Filaria NVBDCP - MDA (DEC + Albendazole)
Kala-azar NVBDCP - Elimination by 2023
Dengue/Chik NVBDCP - Vector control (Aedes)
Vaccines UIP 1985 12 antigens covered
Nhp for communicable diseases give them like answer to the question all imp points covered
National Health Programmes (NHP) for Communicable Diseases in India
INTRODUCTION
National Health Programmes are centrally sponsored, goal-directed initiatives by the Government of India to reduce morbidity and mortality from major communicable diseases. Each programme operates through the national health care delivery system from central to peripheral level.
OVERVIEW FLOWCHART
COMMUNICABLE DISEASE NHPs IN INDIA
│
┌─────────┼──────────┬──────────────┬──────────────┐
│ │ │ │ │
NTEP NVBDCP NLEP NACP UIP/NIS
(TB) (Vector- (Leprosy) (HIV/AIDS) (Immunization)
borne)
│
┌──────┼────────┬────────┐
Malaria Dengue Filaria Kala-azar
Chikungunya JE
1. NATIONAL TB ELIMINATION PROGRAMME (NTEP) ⭐⭐
Evolution
NTP (1962) → RNTCP (1997, DOTS) → STOP TB (2006) → End TB (2014) → NTEP (renamed 2020)
Objectives
- Cure rate ≥ 85% of infectious cases through DOTS
- Case detection ≥ 70% of estimated cases by quality sputum microscopy
DOTS Strategy - 5 Components ⭐
| # | Component |
|---|---|
| 1 | Political will & administrative commitment |
| 2 | Diagnosis by quality-assured sputum smear microscopy |
| 3 | Adequate supply of quality short-course chemotherapy drugs |
| 4 | Directly Observed Treatment (DOT) |
| 5 | Systematic monitoring & accountability |
STOP TB Strategy (2006) - Additional Components
- Pursuing quality DOTS expansion
- Addressing TB/HIV & MDR-TB
- Contributing to health system strengthening
- Engaging all care providers
- Empowering patients & communities
- Enabling & promoting research
End TB Strategy (2014)
Vision: Zero deaths, disease and suffering due to TB (by 2030)
NTEP Organization Structure
Ministry of Health & Family Welfare
↓
Central TB Division (CTD) - National level
↓
State TB Cell (STO) - State level
↓
District TB Centre (DTO) - District level
↓
Peripheral Health Institutions (PHI)
Key Drugs
- DOTS regimen: 2HRZE / 4HR (Isoniazid + Rifampicin + Pyrazinamide + Ethambutol)
- MDR-TB: Bedaquiline-based regimens (Group A, B, C classification)
2. NATIONAL VECTOR BORNE DISEASE CONTROL PROGRAMME (NVBDCP) ⭐⭐
Diseases Covered
NVBDCP (2003)
│
├── Malaria
├── Dengue & Chikungunya
├── Lymphatic Filariasis
├── Kala-azar (Visceral Leishmaniasis)
└── Japanese Encephalitis (JE)
A. MALARIA - Programme Milestones
| Year | Milestone |
|---|---|
| Pre-1953 | 75 million cases, 0.8 million deaths |
| 1953 | NMCP (National Malaria Control Programme) launched |
| 1958 | Renamed NMEP (Eradication Programme) |
| 1965 | Cases ↓ to 0.1 million |
| 1970s | Resurgence - cases back to 6.46 million (1976) |
| 1999 | Renamed NAMP |
| 2002 | Renamed NVBDCP |
| 2005 | RDT (Rapid Diagnostic Test) introduced |
| 2006 | ACT (Artemisinin Combination Therapy) introduced for Pf resistance |
| 2009 | LLINs (Long-Lasting Insecticidal Nets) introduced |
| 2016 | National Framework for Malaria Elimination launched |
| 2017 | National Strategic Plan for Malaria Elimination 2017-2022 |
Malaria Control Strategies
ANTI-MALARIA MEASURES
│
┌────┴────┬──────────────┐
│ │ │
PARASITE VECTOR HOST
│ │ │
Diagnosis IRS (DDT/ Chemoprophylaxis
RDT/Smear Malathion) Presumptive
ACT/CQ Larvicides treatment
treatment LLINs IEC
Biological
control
B. LYMPHATIC FILARIASIS ELIMINATION
- Strategy: Annual MDA (Mass Drug Administration)
- DEC alone (till 2007) → DEC + Albendazole (from 2007)
- Given to all eligible persons except: pregnant women, children <2 years, seriously ill
- Target: Elimination = microfilaria prevalence <1%
- Started: 2004; All 250 endemic districts covered by 2007
C. KALA-AZAR (Visceral Leishmaniasis) Elimination
- Target: <1 case per 10,000 population at block level
- Drug of choice: Liposomal Amphotericin B (single dose)
- Vector: Phlebotomus argentipes (sandfly) - indoor residual spraying
D. DENGUE & CHIKUNGUNYA
- Vector: Aedes aegypti (breeds in clean stagnant water)
- Control: Source reduction, larvicides, personal protection
- No specific treatment / vaccine (dengue vaccine limited use)
3. NATIONAL LEPROSY ERADICATION PROGRAMME (NLEP) ⭐⭐
Timeline
NLCP (1955) → NLEP (1983) → WHO MDT introduced (1982) → Elimination achieved (2005)
Goal
Elimination = <1 case per 10,000 population at national level India achieved elimination at national level: 2005
MDT Regimens ⭐
| Type | Drugs | Duration |
|---|---|---|
| PB (Paucibacillary) | Rifampicin + Dapsone | 6 months |
| MB (Multibacillary) | Rifampicin + Dapsone + Clofazimine | 12 months |
MDT = Monthly supervised + daily unsupervised doses
Classification of Leprosy
LEPROSY
│
├── PB (1-5 skin patches, smear negative)
│ → Tuberculoid (TT), Borderline Tuberculoid (BT)
│
└── MB (>5 skin patches, smear positive)
→ Borderline (BB), Borderline Lepromatous (BL), Lepromatous (LL)
Key Indicators
- ANCDR: Annual New Case Detection Rate (per 1,00,000)
- PR: Prevalence Rate (per 10,000)
- Grade II disability rate among new cases
- Child proportion among new cases (indicator of active transmission)
Strategies
- Free MDT through government services
- Disability prevention & rehabilitation
- IEC for stigma reduction
- Integration with general health services
4. NATIONAL AIDS CONTROL PROGRAMME (NACP) ⭐⭐
Timeline
1986: First HIV case in India
1987: NACP launched → NACO set up
1992: NACP-I → 1999: NACP-II → 2007: NACP-III → 2012: NACP-IV → 2017: NSP 2017-2024
Phases of NACP
| Phase | Year | Focus |
|---|---|---|
| NACP-I | 1992-1999 | Slow down HIV spread; surveillance |
| NACP-II | 1999-2006 | Behaviour change; decentralisation; NGO involvement |
| NACP-III | 2007-2012 | Halt & reverse epidemic; ART scale-up |
| NACP-IV | 2012-2017 | Accelerate response; concentrate on high-risk groups |
| NSP | 2017-2024 | Ending AIDS; 90-90-90 targets |
Aims of NACP
- Prevent further HIV transmission
- Decrease morbidity & mortality associated with HIV
- Minimize socio-economic impact
NACO Structure
National AIDS Control Organization (NACO)
- Under Ministry of Health & Family Welfare
↓
State AIDS Control Societies (SACS)
↓
District AIDS Prevention & Control Units (DAPCU)
Key Interventions
- Free ART (Antiretroviral Treatment) - started 2004
- ICTC (Integrated Counselling & Testing Centres)
- PPTCT (Prevention of Parent to Child Transmission)
- TI (Targeted Interventions) for high-risk groups (FSW, MSM, IDU, migrants)
- Blood safety: National Blood Policy (2002)
- Condom promotion, IEC
90-90-90 Targets (UNAIDS)
90% of people with HIV know their status
→ 90% of diagnosed on treatment
→ 90% of treated virally suppressed
5. UNIVERSAL IMMUNIZATION PROGRAMME (UIP) ⭐⭐
Evolution
EPI launched by WHO (1974) → EPI India (Jan 1978) → UIP launched (Nov 19, 1985)
Dedicated to memory of Smt. Indira Gandhi
National Immunization Schedule (Key vaccines) ⭐
| Vaccine | Disease | Schedule |
|---|---|---|
| BCG | TB | Birth |
| OPV | Polio | Birth, 6, 10, 14 wks; 16-18 months; 5 yrs |
| IPV | Polio | 6 & 14 weeks |
| Hep B | Hepatitis B | Birth, 6 wks, 14 wks |
| Pentavalent | DPT + HepB + Hib | 6, 10, 14 weeks |
| Measles/MR | Measles, Rubella | 9-12 months; 16-24 months |
| Rotavirus | Diarrhoea | 6, 10, 14 weeks (selected states) |
| PCV | Pneumonia | 6 wks, 14 wks, 9 months |
| JE | Japanese Encephalitis | 9-12 months (endemic districts) |
| TT | Tetanus | 10 yrs, 16 yrs + Pregnant women |
Mission Indradhanush (2014) ⭐
Reach all unvaccinated/partially vaccinated children under 2 years Target: Full immunization coverage → 90%
Cold Chain
State Vaccine Store → Regional/Divisional Store → District Store
→ CHC/PHC → Sub-Centre → Village (field worker/ANM)
SUMMARY TABLE - QUICK RECALL ⭐⭐
| Programme | Started | Target | Key Strategy | Goal |
|---|---|---|---|---|
| NTEP | 1962/1997/2020 | TB | DOTS | Elimination by 2025 |
| NVBDCP | 2003 | Malaria, Dengue, Filaria, KA, JE | IRS, ACT, MDA, LLINs | Malaria elimination 2027 |
| NLEP | 1983 | Leprosy | MDT (6/12 months) | Elimination (achieved 2005) |
| NACP/NACO | 1987 | HIV/AIDS | ART, ICTC, TI | 90-90-90 |
| UIP | 1985 | Vaccine-preventable | 12 antigens; cold chain | Universal coverage |