Hirsutism
Reading File
Finding Sources
Searching Images
hirsutism female androgen excess clinical presentation
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of hirsutism based on authoritative medical textbooks.
Hirsutism
Definition
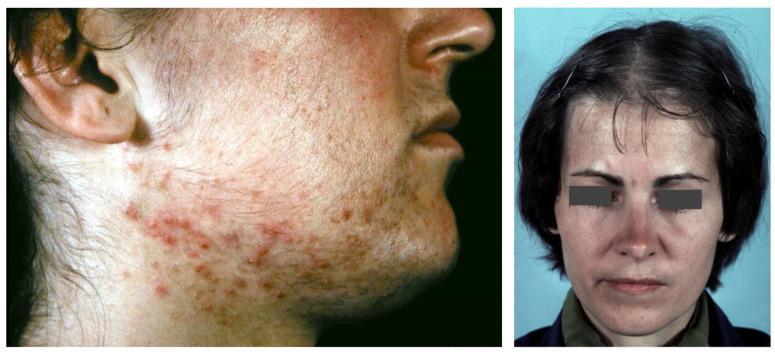
Hirsutism is the presence of excess terminal (coarse) hairs in androgen-dependent areas of a woman, producing a male-like distribution pattern. It affects approximately 5–15% of women. Affected areas include the upper lip, chin, chest, lower abdomen, and extremities.
It must be distinguished from hypertrichosis — a diffuse increase in fine, vellus hair that is not androgen-dependent and may be congenital or drug-induced (e.g., diazoxide, minoxidil, phenytoin).
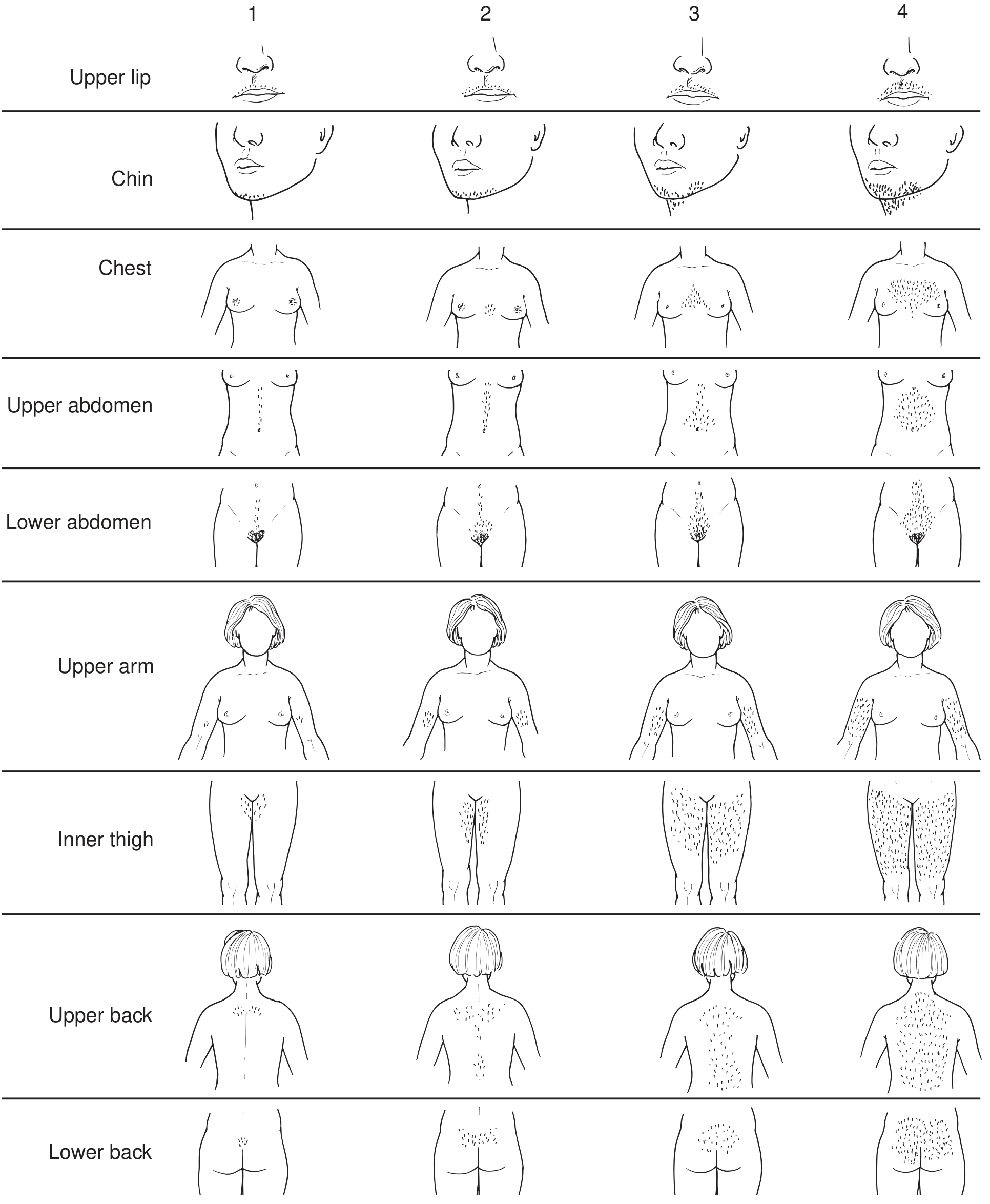
Assessment — Modified Ferriman-Gallwey Score
Hair growth in 9 body areas is scored 0–4 (0 = no hair; 4 = frankly virile). A total score >8 qualifies as hirsutism. Ethnic and racial variation must be considered (e.g., southern European women may have more body hair without true virilization).
Virilization is more severe and includes deepening of the voice and clitoral hypertrophy in addition to hirsutism.
Pathophysiology
True hirsutism reflects androgen excess — involving testosterone, androstenedione, DHEA, or DHEA-S. Androgens convert fine vellus hairs to coarse terminal hairs in androgen-sensitive pilosebaceous units. The principal intracellular androgen in the hair follicle is dihydrotestosterone (DHT), formed by 5α-reductase action on testosterone.
Causes
| Category | Examples |
|---|---|
| Most common | Idiopathic hirsutism; Polycystic ovary syndrome (PCOS) |
| Adrenal | Congenital adrenal hyperplasia (21-hydroxylase deficiency — classic or non-classic); Adrenal tumors; Cushing syndrome |
| Ovarian | Ovarian androgen-secreting tumors; Ovarian hyperthecosis |
| Other endocrine | Hyperprolactinemia; Hyperandrogenic insulin-resistant acanthosis nigricans (HAIRAN) syndrome |
| Drug-induced | Anabolic steroids, danazol |
Clinical Evaluation
History: ethnic background, age of onset, menstrual irregularities, virilization, pelvic masses, hypertension, drug use.
Laboratory workup:
- Total and bioavailable testosterone
- Serum DHEA-S
- 24-hour urine 17-ketosteroids
- Consider prolactin, 17-hydroxyprogesterone (for CAH screening), fasting insulin/glucose
Imaging: pelvic ultrasound, CT, or MRI to identify ovarian or adrenal masses if indicated.
Treatment
Non-Pharmacologic (all patients)
| Method | Notes |
|---|---|
| Bleaching | Cosmetic, for mild cases |
| Shaving / chemical depilatory | Removes surface hair; shaving does NOT increase density |
| Waxing / plucking | Temporary; uncomfortable |
| Electrolysis | Effective for permanent removal, especially in skilled hands |
| Laser / IPL | Best for large areas of pigmented terminal hair; photothermolysis of melanin in follicle; can cause permanent removal |
Pharmacologic
Drug therapy targets four mechanisms:
- Suppression of ovarian/adrenal androgen production
- Enhancement of SHBG (reducing free testosterone)
- Impairment of peripheral androgen conversion
- Inhibition of androgen action at target tissue
Attenuation of hair growth is typically not evident until 4–6 months after starting treatment; maximum effect may require 9–12 months.
| Drug | Mechanism | Notes |
|---|---|---|
| Combined OCP (1st line) | Suppresses LH → ↓ovarian androgens; ↑SHBG; direct sebaceous suppression | ~20% improvement in hirsutism; ~50% improvement in acne. Prefer non-androgenic progestins (norgestimate, drospirenone). Avoid in thromboembolism history, smokers, hypertension, migraine |
| Spironolactone (100–200 mg/day) | Weak antiandrogen — competitive AR inhibition; also mineralocorticoid antagonist | Monitor for hyperkalemia and hypotension. Avoid in pregnancy (feminization of male fetus). Often combined with OCP |
| Cyproterone acetate (50–100 mg, days 1–15) | Prototypic antiandrogen — competitive AR inhibition; ↑testosterone clearance | Not available in USA; widely used in Europe/Canada. Side effects: irregular bleeding, nausea, fatigue, decreased libido |
| Finasteride | 5α-reductase type 2 inhibitor → ↓DHT | Limited efficacy (PSU predominantly expresses type 1). Avoid in pregnancy |
| Dutasteride | Inhibits both 5α-reductase types 1 and 2 | More promising than finasteride for hirsutism; limited studies |
| Flutamide | Potent nonsteroidal antiandrogen | Effective but hepatotoxicity risk limits use |
| GnRH analogues | Suppress gonadotropins → ↓ovarian androgens | Used in severe or refractory cases |
| Glucocorticoids (low-dose) | Suppress adrenal androgen in CAH | Dexamethasone 0.2–0.5 mg/night; OCP preferred first in CAH |
| Metformin (insulin sensitizer) | Reduces hyperinsulinemia → ↓ovarian androgen in PCOS | Adjunct in PCOS with insulin resistance |
| Eflornithine cream | Topical — inhibits ornithine decarboxylase in follicle | Slows facial hair growth; not a depilatory |
Key Points
- OCP + spironolactone is the most commonly used pharmacologic combination
- Drug therapy must be combined with non-pharmacologic hair removal for best results
- Patients should be counseled about the slow response timeline (6–12 months) to avoid early discontinuation
- Pregnancy must be avoided with most antiandrogens (teratogenic risk)
Sources: Harrison's Principles of Internal Medicine 22E, p. 3185 | Textbook of Family Medicine 9e, p. 1053
This is a shared conversation. Sign in to Orris to start your own chat.