PCOD
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
polycystic ovary syndrome PCOS ultrasound pathology
Reading File
I now have comprehensive content. Here's a thorough overview of PCOS/PCOD:
Polycystic Ovary Syndrome (PCOS / PCOD)
PCOD (Polycystic Ovarian Disease) is an older, synonymous term for PCOS (Polycystic Ovary Syndrome) — now the preferred clinical designation.
Definition & Epidemiology
PCOS is the most common endocrine disorder in women of reproductive age, affecting 5–10% of women worldwide. It is the leading cause of:
- Hyperandrogenism (HA)
- Hirsutism
- Anovulatory infertility
First described in 1935 by Stein and Leventhal as a triad of amenorrhea, bilateral polycystic ovaries, and obesity. It is a complex, polygenic/multifactorial disorder with significant reproductive, metabolic, and cardiovascular consequences.
— Berek & Novak's Gynecology, p. 1919
Diagnostic Criteria
Rotterdam Criteria (2003) — 2 out of 3 required (after exclusion of other causes):
| Criterion | Description |
|---|---|
| 1. Oligo/anovulation | Irregular or absent menstrual cycles |
| 2. Hyperandrogenism | Clinical (hirsutism, acne, alopecia) and/or biochemical (elevated androgens) |
| 3. Polycystic ovary morphology | ≥12 follicles 2–9 mm diameter, or ovarian volume >10 mL on ultrasound |
Diagnosis requires exclusion of: congenital adrenal hyperplasia (CAH), androgen-secreting tumors, Cushing syndrome, hyperprolactinemia, thyroid disease.
4 Rotterdam Phenotypes:
- HA + ovarian dysfunction + PCO morphology
- HA + ovarian dysfunction
- HA + PCO morphology
- Ovarian dysfunction + PCO morphology
— Berek & Novak's Gynecology, p. 1919–1920
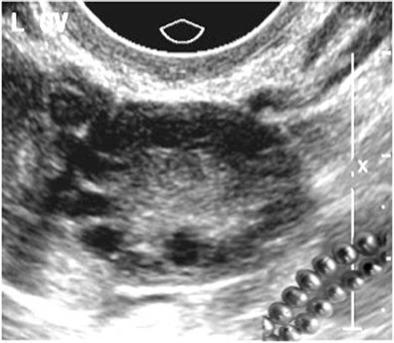
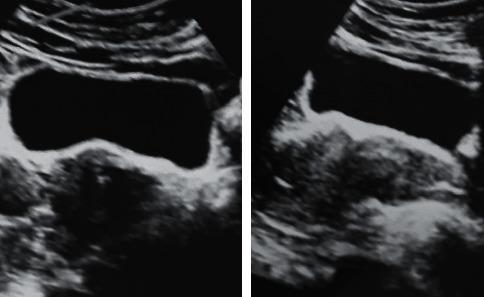
Ultrasound: "String of Pearls" Sign
The classic sonographic finding — multiple small follicles arranged peripherally around an echogenic stroma:
Pathophysiology
Hormonal Abnormalities
- ↑ LH pulse frequency (due to increased GnRH pulse frequency) → elevated LH : FSH ratio
- FSH remains normal/low due to negative feedback from elevated estrogen and inhibin
- Elevated androgens (testosterone, DHEA-S): from both ovarian theca cells and adrenal cortex
- Mild hyperprolactinemia in ~25% of cases
Insulin Resistance (IR)
- A key pathophysiological mechanism in most women with PCOS
- Compensatory hyperinsulinemia stimulates ovarian androgen production
- IR is present even in lean women with PCOS
Steroidogenesis Defect
- Theca cells show intrinsic upregulation of CYP11A, CYP17, 3β-HSD genes → excess testosterone, 17-OH progesterone, and progesterone
— Berek & Novak's Gynecology, p. 1926
Clinical Features
| Feature | Details |
|---|---|
| Menstrual irregularities | Oligomenorrhea, amenorrhea, or irregular cycles from menarche |
| Hirsutism | Most common sign of HA; male-pattern hair growth |
| Acne & oily skin | Androgen-driven |
| Alopecia | Androgenic pattern |
| Obesity | Present in many; worsens phenotype |
| Infertility | Anovulatory; most common cause in developed countries |
| Acanthosis nigricans | Marker of IR |
Associated Long-Term Risks
| System | Risk |
|---|---|
| Metabolic | Type 2 diabetes, impaired glucose tolerance, dyslipidemia, metabolic syndrome |
| Cardiovascular | Hypertension, atherosclerosis (due to hypercholesterolemia + IR) |
| Reproductive | Miscarriage, gestational diabetes, preeclampsia, preterm birth |
| Oncologic | Endometrial cancer (due to unopposed estrogen from anovulation) |
| Psychological | Depression, anxiety |
Management
Lifestyle (First-line for all overweight/obese women)
- Weight loss of 5–10% restores ovulation, reduces androgens, improves insulin sensitivity
- Reduced-calorie diet (<30% fat), ↑ fiber, low glycemic index foods
- Structured exercise >30 min/day
Not Seeking Pregnancy
| Goal | Treatment |
|---|---|
| Menstrual regulation & HA | Combined oral contraceptive pill (COCP) — lowers androgens via ↑ SHBG; first-line |
| Inadequate response to COCP (>6 months) | Add antiandrogens: spironolactone or flutamide |
| Endometrial protection | Progestins (medroxyprogesterone 10 mg, or progesterone 200 mg × 10–14 days, every ≥3 months) or levonorgestrel IUD |
| Cardiometabolic risk | Metformin (especially in overweight/obese) |
Seeking Pregnancy (Ovulation Induction)
- Letrozole (aromatase inhibitor) — first-line
- Clomiphene citrate (± metformin)
- Injectable gonadotropins — under specialist supervision (risk of ovarian hyperstimulation syndrome)
- Laparoscopic ovarian drilling — surgical option for clomiphene-resistant cases
Metformin alone is not recommended for endometrial protection, hyperandrogenism, infertility, or prevention of gestational diabetes.
— Harrison's Principles of Internal Medicine 22E, p. 3179; Berek & Novak's Gynecology, p. 1930
Screening at Diagnosis
- Obesity / BMI
- Blood pressure
- Fasting glucose / HbA1c / oral glucose tolerance test
- Fasting lipid profile (if overweight)
- Depression and anxiety screening
Summary
PCOS is a heterogeneous syndrome — not every woman presents the same way. The Rotterdam criteria allow for 4 phenotypes. Management must be tailored to the patient's primary concern: menstrual regulation, hyperandrogenism, fertility, or metabolic risk.
This is a shared conversation. Sign in to Orris to start your own chat.