Usmle step 2 ck ki book pta hai
Finding Sources
Finding Sources
Hamaari library mein specifically USMLE Step 2 CK ki dedicated book nahi hai. Lekin library mein bahut saari specialist textbooks hain jo Step 2 CK preparation ke liye extremely useful hain - subject by subject:
Hamaari Library Mein Available Books (Step 2 CK Relevant):
| Subject | Book |
|---|---|
| Internal Medicine | Firestein & Kelley's Textbook of Rheumatology |
| Cardiology | Braunwald's Heart Disease |
| Surgery | Bailey & Love's Surgery (28th Ed), Fischer's Mastery of Surgery |
| OB/GYN | Berek & Novak's Gynecology, Creasy & Resnik's Maternal-Fetal Medicine |
| Neurology | Adams & Victor's Neurology (12th Ed), Bradley & Daroff's Neurology |
| Nephrology | Comprehensive Clinical Nephrology (7th Ed), Brenner & Rector's The Kidney |
| Gastroenterology | Clinical Gastrointestinal Endoscopy |
| Dermatology | Andrews' Diseases of the Skin, Dermatology 2-Volume Set |
| Urology | Campbell Walsh Wein Urology |
| ENT | Cummings Otolaryngology |
| Anesthesia | Barash Clinical Anesthesia (9th Ed) |
| Biochemistry | Lippincott Illustrated Reviews Biochemistry (8th Ed) |
| Physiology | Costanzo Physiology (7th Ed) |
Kya karna chahte hain?
- Kisi specific topic ke baare mein poochh sakte hain (e.g., heart failure, eclampsia, nephrology cases)
- Main clinical scenarios ke jawab in books se dhoondh ke de sakta hoon
- Step 2 CK style questions ke liye relevant content extract kar sakta hoon
Kaunsa subject ya topic cover karna hai?
Hypercalcemia samjhao full detailed mai urdu roman mai samjhao
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Ab main puri tarah se detailed jawab likh sakta hoon. Saari information collect ho gayi hai.
🩺 Hypercalcemia - Mukammal Urdu Roman Mein Tafseeli Wazahat
📌 Hypercalcemia Kya Hai? (Definition)
Hypercalcemia matlab blood mein calcium ka level normal se zyada hona.
- Normal serum calcium: 8.2 - 10.2 mg/dL
- Hypercalcemia: > 10.2 mg/dL
- Severe / Symptomatic: > 13-14 mg/dL
- Hypercalcemic crisis: > 14 mg/dL (emergency!)
Calcium body mein ionized (free) ya protein-bound hota hai. PTH (Parathyroid Hormone) aur Vitamin D calcium ko regulate karte hain.
🔬 Calcium Regulation Ka Mechanism (Normal Physiology)
Calcium ko 3 organs control karte hain:
| Organ | Kaam |
|---|---|
| Parathyroid gland | PTH banata hai - calcium badhata hai |
| Kidney | Calcium reabsorb ya excrete karta hai |
| Intestine | Vitamin D ke zariye calcium absorb karta hai |
| Bone | Calcium ka bada store - PTH se release hota hai |
PTH ka kaam:
- Bone se calcium release karta hai (osteoclast activate karke)
- Kidney mein calcium reabsorb karta hai
- Kidney mein Vitamin D ko activate karta hai (25-OH-D ko 1,25-OH-D banata hai)
- 1,25-OH-D intestine se calcium absorb karata hai
⚡ Causes of Hypercalcemia (Asbab)
Mnemonic yaad rakhein: "CHIMPANZEES"
| Letter | Cause |
|---|---|
| C | Calcium supplements / Milk-Alkali syndrome |
| H | Hyperparathyroidism (PRIMARY - sabse common cause overall) |
| I | Immobilization (prolonged bed rest) |
| M | Malignancy (cancer - hospital patients mein sabse common) |
| P | Paget's disease of bone |
| A | Addison's disease (adrenal insufficiency) |
| N | Neoplasm (cancer) |
| Z | Zollinger-Ellison syndrome |
| E | Excess Vitamin D / Excess Vitamin A |
| E | Endocrine (thyrotoxicosis, pheochromocytoma) |
| S | Sarcoidosis / granulomatous diseases |
🔴 DO SABSE IMPORTANT CAUSES (USMLE ke liye):
1. PRIMARY HYPERPARATHYROIDISM (PHPT)
Outpatients / Ambulatory patients mein #1 cause
- 80% cases: Solitary parathyroid adenoma
- 15% cases: Parathyroid hyperplasia (especially MEN-1, MEN-2A mein)
- <1% cases: Parathyroid carcinoma
PTH level: HIGH (ya inappropriately normal)
Phosphate: LOW (PTH kidney se phosphate nikal deta hai)
Urinary calcium: HIGH
Lab profile (PHPT mein):
- Serum Ca: 10.7 mg/dL (high)
- PTH: 119 pg/mL (normal: 10-65) - HIGH
- Phosphorus: 2.8 mg/dL (low-normal)
- Alkaline phosphatase: slightly elevated
2. MALIGNANCY-ASSOCIATED HYPERCALCEMIA
Inpatients / Hospital patients mein #1 cause
Cancer ke 30% patients mein hoti hai. Yeh 3 tareeqon se hoti hai:
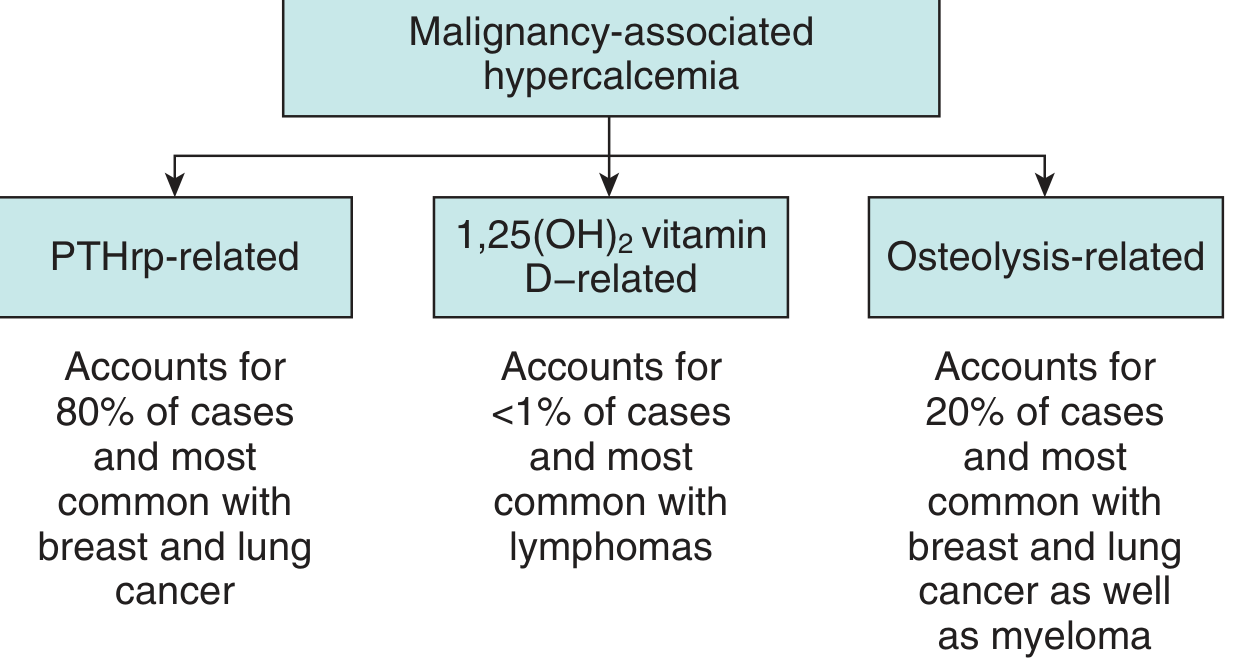
Mechanism 1 - PTHrP (Parathyroid Hormone-related Peptide) - 80% cases:
- Tumor ek fake PTH banata hai jo PTHrP kehlata hai
- Yeh PTH ki tarah kaam karta hai - bone resorption badhata hai, renal calcium reabsorption badhata hai
- BUT - Intestinal calcium absorption nahi badhata (PTH se fark)
- Breast cancer, lung cancer (squamous cell) mein common
- PTH: LOW, PTHrP: HIGH
Mechanism 2 - Local Osteolysis - 20% cases:
- Cancer seedha bone mein grow karta hai
- IL-1, IL-6, TNF release hote hain jo osteoclasts activate karte hain
- Bone destroy hoti hai, calcium blood mein aata hai
- Multiple myeloma, breast cancer, lymphoma mein common
- Skeletal X-ray mein: lytic bone lesions
Mechanism 3 - Vitamin D activation by tumor - <1%:
- Lymphoma cells 1,25-OH-D (active Vit D) banate hain
- Intestinal calcium absorption badhti hai
- PTH: LOW, 1,25-OH-D: HIGH
3. SARCOIDOSIS / GRANULOMATOUS DISEASES
- Granuloma cells (macrophages) Vitamin D ko activate kar deti hain
- 1,25-OH-D level HIGH hota hai
- PTH: LOW
4. MEDICATIONS
- Thiazide diuretics: Kidney mein calcium retention badhate hain
- Lithium: PTH secretion badh jaati hai
- Calcium carbonate + Vitamin D (excess): Milk-Alkali syndrome
- Agar asymptomatic hai aur Ca < 14 mg/dL - medication band karo, 1 hafte baad dobara check karo
😣 Symptoms of Hypercalcemia
Classic Mnemonic: "Bones, Stones, Moans, Abdominal Groans" (+ Psychic Overtones!)
| Symptom | Detail |
|---|---|
| 🦴 Bones (bone pain) | Osteitis fibrosa cystica, pathologic fractures, osteoporosis |
| 🪨 Stones (renal calculi) | Nephrolithiasis - kidney mein patthar, nephrocalcinosis |
| 😔 Moans (psychiatric) | Depression, anxiety, confusion, psychosis, lethargy, coma |
| 🤢 Abdominal Groans | Nausea, vomiting, constipation, pancreatitis, peptic ulcer |
| 💧 Polyuria / Polydipsia | Nephrogenic diabetes insipidus - kidney ADH ko ignore karne lagti hai |
| ❤️ Cardiac | Bradycardia, short QT interval on ECG, cardiac arrest (severe) |
| 💪 Muscle weakness | Proximal muscle weakness, fatigue |
Yaad rakhein: Symptoms ki severity depend karta hai:
- Calcium kitna high hai
- Kitni tezi se badha hai
>13 mg/dL wale patients usually symptomatic hote hain.
🔍 Diagnosis / Workup
Step 1: Confirm Hypercalcemia
- Serum ionized calcium measure karo (total calcium albumin se adjust hota hai)
- Albumin correction: Total Ca + 0.8 × (4.0 - serum albumin)
Step 2: PTH measure karo - YEH SABSE PEHLA AUR ZAROORI TEST HAI
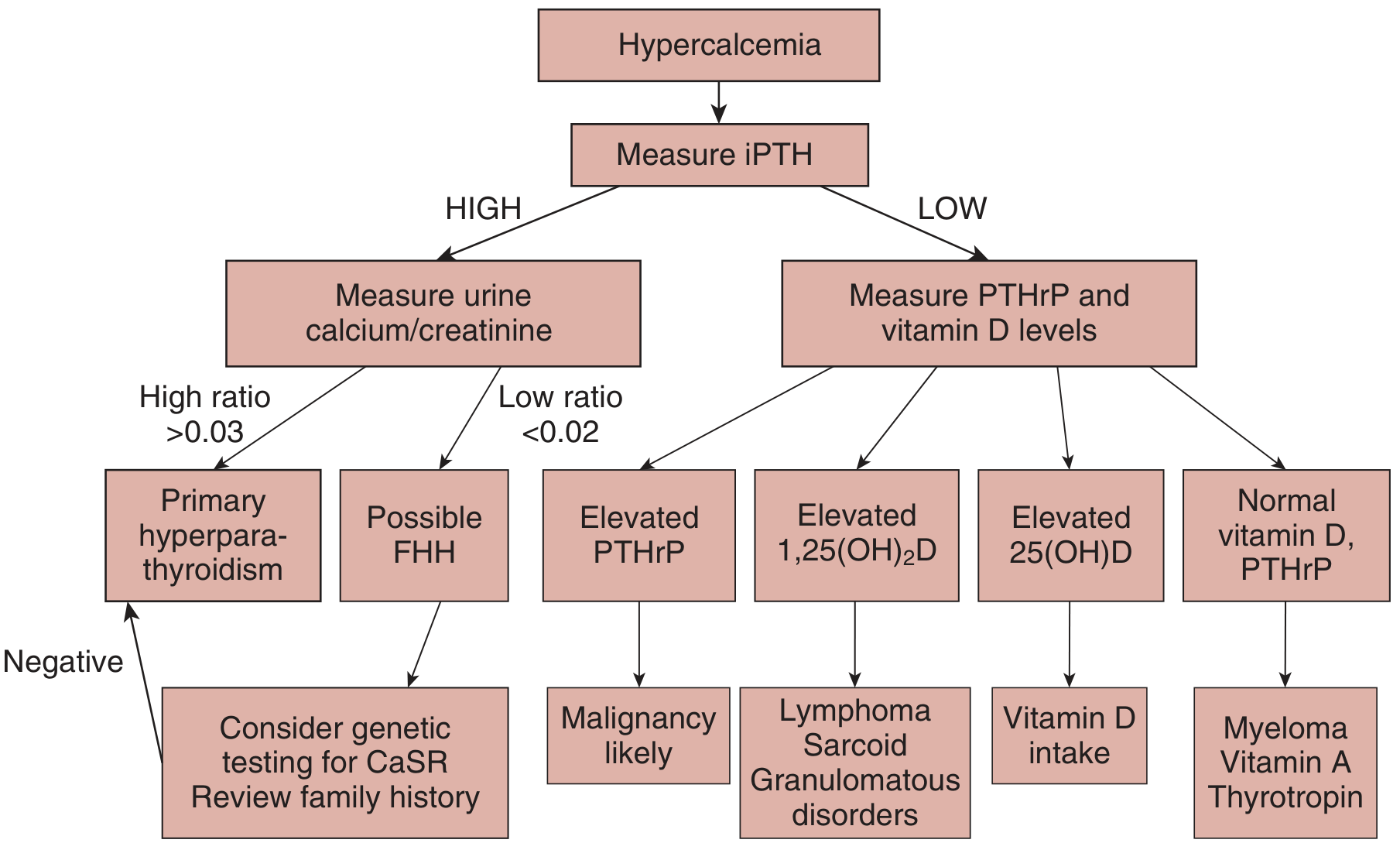
Diagram ki explanation:
PTH HIGH hai:
- 24-hour urine calcium/creatinine ratio check karo
- Ratio > 0.03 → Primary Hyperparathyroidism (PHPT)
- Ratio < 0.02 → FHH (Familial Hypocalciuric Hypercalcemia) - benign condition
PTH LOW hai:
- PTHrP aur Vitamin D levels check karo:
- PTHrP HIGH → Malignancy (most likely)
- 1,25-OH-D HIGH → Lymphoma, Sarcoidosis, Granulomatous disease
- 25-OH-D HIGH → Vitamin D intoxication
- Sab normal → Myeloma, Vitamin A toxicity, Thyrotropin
Lab Summary Table:
| Cause | PTH | Calcium | Phosphate | PTHrP | Vit D |
|---|---|---|---|---|---|
| PHPT | HIGH ↑ | HIGH ↑ | LOW ↓ | Normal | Normal |
| Malignancy (PTHrP) | LOW ↓ | HIGH ↑ | LOW ↓ | HIGH ↑ | Normal |
| Malignancy (Osteolysis) | LOW ↓ | HIGH ↑ | High/Normal | Normal | Normal |
| Sarcoidosis/Lymphoma | LOW ↓ | HIGH ↑ | Normal | Normal | 1,25-OH-D HIGH ↑ |
| Vit D toxicity | LOW ↓ | HIGH ↑ | HIGH ↑ | Normal | 25-OH-D HIGH ↑ |
| FHH | HIGH/Normal | Mildly HIGH | Normal | Normal | Normal |
💊 Treatment (Ilaj)
🚨 Acute / Severe Hypercalcemia (Emergency Treatment):
Step 1 - IV Normal Saline (sabse pehle!)
- 2-4 L/day aggressive rehydration
- Hypercalcemia se nephrogenic DI hoti hai → polyuria → dehydration
- Calcium sensing receptor loop of Henle mein natriuresis karta hai → aur dehydration
- Isliye pehle fluid do!
Step 2 - Loop Diuretics (Furosemide)
- Fluid overload prevent karne ke liye
- Elderly patients aur cardiac/renal disease mein especially
- Note: Thiazide diuretics KABHI NAHI dena - yeh calcium badhate hain!
Step 3 - Bisphosphonates (bone resorption rokne ke liye)
- Zoledronate (Zometa): 4 mg IV over 15 min - most potent
- Pamidronate: 60-90 mg IV over 2-4 hrs
- Onset: 2-4 din mein effect shuru, 4-7 din mein peak
- Renal function monitor karo - nephrotoxic ho sakta hai
Step 4 - Calcitonin
- Fastest action (4-6 ghante mein kaam karta hai)
- Calcium ~1-2 mg/dL kam karta hai
- Tachyphylaxis develop hoti hai (2-3 din baad effect khatam)
- Bisphosphonate ke sath milake use karo (bridge therapy)
Step 5 - Denosumab
- RANKL antibody - osteoclasts ko block karta hai
- Renal insufficiency mein safe (dose adjust nahi chahiye)
- Malignancy mein use hota hai
Step 6 - Corticosteroids
- Specifically: Sarcoidosis, Lymphoma, Vitamin D toxicity mein
- Vitamin D activation block karte hain
Step 7 - Dialysis
- Severe refractory hypercalcemia mein last resort
💊 Long-term / Definitive Treatment:
| Cause | Definitive Treatment |
|---|---|
| Primary Hyperparathyroidism (symptomatic) | Parathyroidectomy - yehi ek cure hai |
| PHPT (asymptomatic) | Surgery if: Ca > 1 mg/dL above normal, age <50, osteoporosis, renal stones |
| Malignancy | Treat underlying cancer + bisphosphonates |
| Sarcoidosis | Corticosteroids |
| Medication-induced | Band karo, 1 hafta wait karo |
🎯 USMLE Step 2 CK High-Yield Points (Yaad rakho!)
- Outpatients mein #1 cause = Primary Hyperparathyroidism (parathyroid adenoma)
- Inpatients mein #1 cause = Malignancy (squamous cell lung cancer, breast cancer, myeloma)
- Mnemonic: "Bones, Stones, Groans, Psychic Moans"
- ECG finding: Short QT interval
- First step in workup: Measure iPTH
- First step in TREATMENT: IV Normal Saline (aggressive hydration)
- PTHrP: Cancer mein hota hai, PTH LOW rahta hai
- FHH: PTH high lekin urine calcium LOW - benign, surgery NAHI chahiye
- Sarcoidosis mein: 1,25-OH-D high, PTH low - treat with steroids
- Calcitonin: Fastest acting but tachyphylaxis hoti hai
- Bisphosphonates: Serum creatinine monitor karo - nephrotoxic!
- MEN-1: Hyperparathyroidism + Pituitary tumor + Pancreatic tumor
- Thiazide diuretics: Hypercalcemia BADHATE hain (urine mein calcium retention)
- Loop diuretics (Furosemide): Treatment mein use karte hain (calcium excretion badhata hai)
📊 Quick Comparison: PTH vs PTHrP
| Feature | PTH (PHPT) | PTHrP (Malignancy) |
|---|---|---|
| Source | Parathyroid gland | Tumor |
| PTH level | HIGH | LOW |
| Bone resorption | YES | YES |
| Renal Ca reabsorption | YES | YES |
| Intestinal Ca absorption | YES (via Vit D activation) | NO |
| 1,25-OH-D | High | Low/Normal |
| Urine cAMP | HIGH | HIGH |
Sources: Textbook of Family Medicine, 9e; Brenner and Rector's The Kidney (2-Volume Set)
Hyperparathyroidism samjhao
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Sab zaroori information aa gayi. Ab mukammal Roman Urdu jawab likhta hoon.
🩺 Hyperparathyroidism - Mukammal Urdu Roman Wazahat
📌 Hyperparathyroidism Kya Hai?
Hyperparathyroidism matlab parathyroid glands se zaroorat se zyada PTH (Parathyroid Hormone) nikalna. Iska seedha natija hypercalcemia (blood mein zyada calcium) hota hai.
Parathyroid glands 4 choti glands hoti hain jo thyroid ke peeche hoti hain. Inki zaroorat sirf calcium aur phosphate ko regulate karna hai.
🔢 Hyperparathyroidism ke 3 Types
| Type | Kya hota hai | Cause |
|---|---|---|
| Primary | Parathyroid khud hi zyada PTH banane lagti hai | Adenoma / Hyperplasia |
| Secondary | Koi aur cheez calcium kam karti hai, parathyroid compensate karne ki koshish mein PTH badhata hai | Chronic Renal Failure, Vit D deficiency |
| Tertiary | Secondary ko itna waqt guzar jaata hai ke parathyroid autonomously kaam karne lagti hai | Long-standing renal failure |
1️⃣ PRIMARY HYPERPARATHYROIDISM (PHPT)
Epidemiology:
- 1000 adults mein se 3 mein hoti hai
- Females mein 3 guna zyada (males se)
- Age: 40-65 saal mein peak
- Asymptomatic hypercalcemia ki #1 cause hai
Causes (Etiology):
| Cause | % |
|---|---|
| Solitary parathyroid adenoma | 80-85% |
| Parathyroid hyperplasia (4 glands) | 15-20% |
| Parathyroid carcinoma | < 0.5% |
Genetic Mutations (USMLE ke liye important):
- MEN-1 gene mutation - 35-50% sporadic adenomas mein
- Cyclin D1 (CCND1) overexpression - 15% mein
- CDC73 mutation - 70% parathyroid carcinomas mein
- Wnt/β-catenin pathway abnormality - 85% mein
Microscopic Appearance (Histology):
Parathyroid Adenoma ka Histology:
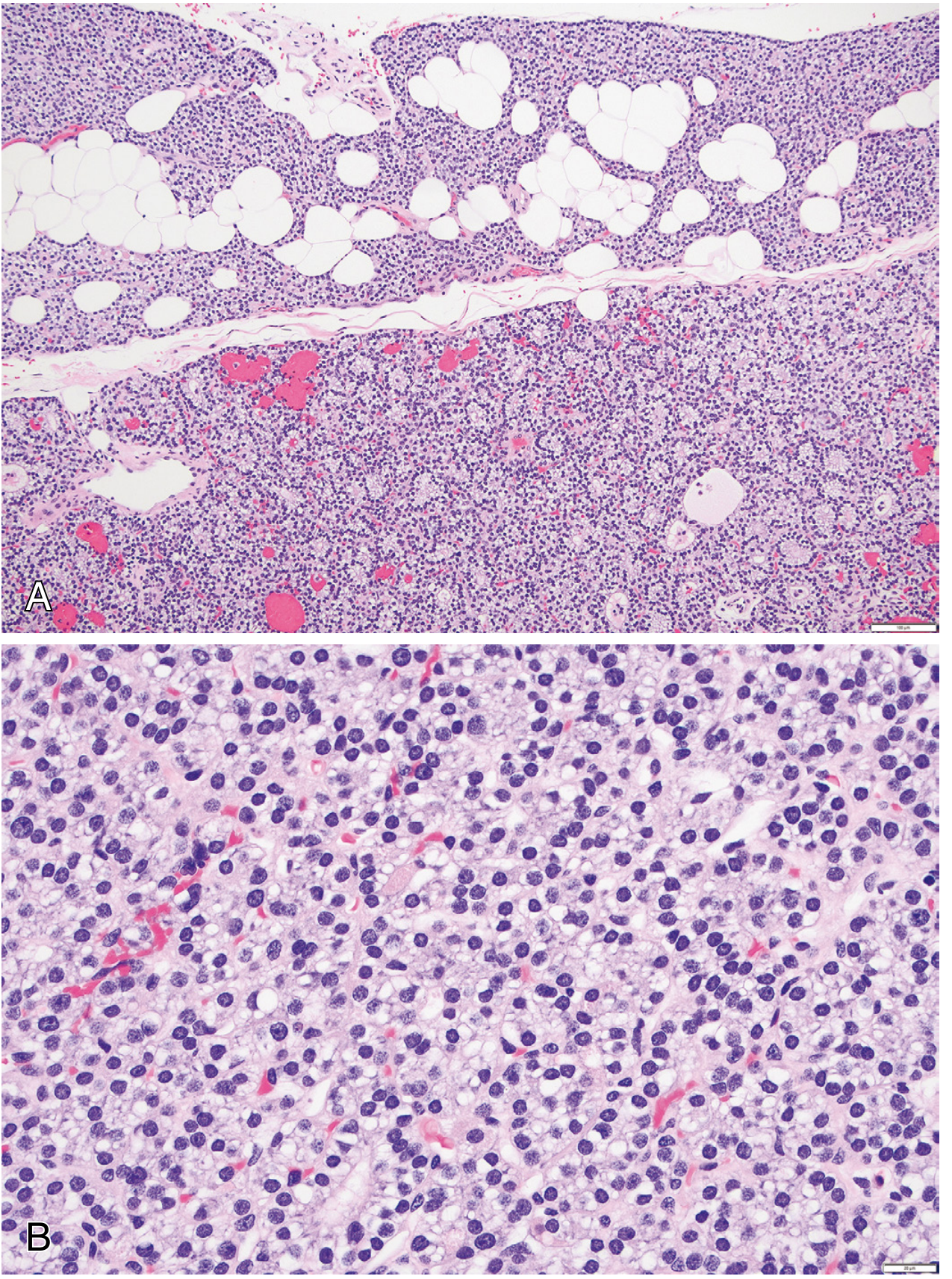
- Chief cells se bani hoti hai (uniform, monotonous)
- Fat cells: kam ya nahi ke barabar (normal gland mein hote hain)
- Adenoma ke edge par normal parathyroid tissue ki rim hoti hai
- Mitoses rare hote hain
- Dusri glands: normal ya choti (feedback inhibition se)
Pathophysiology (Kaise hota hai nuksaan):
PTH excess se yeh changes aate hain:
PTH barh jaata hai
↓
1. BONE: Osteoclasts activate → RANKL expression badh jaata hai
→ Bone resorption → Calcium blood mein aata hai
→ Osteitis fibrosa cystica, brown tumors
2. KIDNEY: Calcium reabsorption BADHTA hai
Phosphate excretion BADHTA hai
→ Hypercalcemia + Hypophosphatemia
3. INTESTINE: PTH → Vitamin D activate karta hai
→ 1,25-OH-D badhta hai
→ Intestinal calcium absorption badhti hai
Net result: Blood calcium HIGH, Phosphate LOW
Clinical Features (Symptoms):
Classic Mnemonic: "Painful Bones, Renal Stones, Abdominal Groans, Psychic Moans"
🦴 BONES (Haddiyon mein changes):
- Osteitis fibrosa cystica - PTH se bone buri tarah resorb hoti hai
- Brown tumors - bone cysts (hemorrhage se brown rang aata hai) - long bones mein
- Subperiosteal bone resorption - X-ray mein radial border of middle phalanx par
- Salt and pepper skull - khopri ki X-ray mein pattern
- Distal clavicle tapering (clavicle ka end ghis jaata hai)
- Osteoporosis - especially cortical bone mein (radius, hip)
- Pathologic fractures
Note: Aaj kal early detection ki wajah se classic bone changes sirf <5% patients mein milte hain!
🪨 STONES (Kidney mein):
- Nephrolithiasis (kidney stones) - 20% patients mein
- Nephrocalcinosis - kidney mein calcium deposits
- Hypercalciuria - 30% patients mein
- Polyuria aur polydipsia (nephrogenic DI)
🤢 ABDOMINAL GROANS:
- Peptic ulcers (gastrin secretion badhti hai)
- Pancreatitis (calcium pancreatic enzymes activate karta hai)
- Nausea, vomiting
- Constipation
- Gallstones
😔 PSYCHIC MOANS (Neuropsychiatric):
- Depression, anxiety
- Lethargy, fatigue
- Proximal muscle weakness (neuromuscular)
- Confusion
- Seizures (severe mein)
- Aortic/mitral valve calcification (cardiac)
Diagnosis (PHPT ki):
Step 1: Hypercalcemia confirm karo (serum calcium >10.2 mg/dL)
Step 2: PTH measure karo
- PTH HIGH ya inappropriately normal = Primary Hyperparathyroidism
Lab Findings:
| Test | Result |
|---|---|
| Serum Calcium | HIGH ↑ |
| Serum Phosphate | LOW ↓ |
| PTH | HIGH ↑ (normally calcium badhne par PTH gir jaati hai - yahan nahi girta) |
| Alkaline Phosphatase | Elevated (bone turnover badha) |
| Urine Calcium | HIGH ↑ (30% mein) |
| Chloride | Slightly HIGH |
| Bicarbonate | Slightly LOW |
| 1,25-OH-D | HIGH ↑ (sometimes) |
| 25-OH-D | Normal |
| Urine cAMP | HIGH ↑ |
| Chloride:Phosphate ratio | >33 = PHPT ka clue |
Imaging for Localization (tumor dhundne ke liye):
- Sestamibi scintigraphy (Tc-99m MIBI) + CT (SPECT) - PREFERRED (3D image deta hai)
- Ultrasound neck
- MRI
- (Note: Do modalities milake confirm karte hain - false positives hote hain)
Surgery ke Guidelines (Parathyroidectomy kab karein?):
Surgery zaroori hai agar koi bhi ek condition ho:
- Nephrolithiasis ya bone erosions (complications) hain
- Life-threatening hypercalcemia ka episode aaya ho
- Serum Ca > 1 mg/dL above normal limit
- Urinary Ca > 400 mg/24 hr (men) ya >300 mg/24 hr (women)
- Creatinine clearance < 60 mL/min
- Bone mineral density T-score < -2.5 (osteoporosis)
- Age < 50 years
Surgery ke baad:
- 98% cases mein biochemical cure hoti hai (skilled surgeon ke haath se)
- Bone mineral density 6-12 mahine mein badh jaati hai, 10 saal tak improve hoti rehti hai
- Complications: Recurrent laryngeal nerve damage, permanent hypoparathyroidism
Asymptomatic PHPT Management:
- Sirf 25% progressive hoti hai (10 saal mein)
- Watchful waiting kaafi hai agar surgery criteria na milen
- Medical therapy: Cinacalcet (calcimimetic) - calcium-sensing receptor ko activate karta hai, PTH aur calcium dono kam karta hai
- Bisphosphonates - bone density maintain karte hain
2️⃣ SECONDARY HYPERPARATHYROIDISM
Kya hota hai:
Parathyroid gland normal hoti hai, lekin koi external cause chronic hypocalcemia kar raha hota hai. Iske jawab mein parathyroid compensatory PTH badhati hai.
Causes:
- Chronic Renal Failure (#1 cause) - sabse common
- Vitamin D deficiency
- Malabsorption / steatorrhea
- Inadequate calcium intake
Mechanism (Renal Failure mein):
Chronic Renal Failure
↓
Phosphate excretion kam → Hyperphosphatemia
↓
Phosphate calcium ko seedha depress karta hai → Hypocalcemia
↓
PLUS: Kidney mein α1-hydroxylase kam → 1,25-OH-D kam
↓
Intestinal calcium absorption kam → Aur zyada hypocalcemia
↓
Parathyroid gland stimulate hoti hai → PTH BARH JAATA HAI
↓
Bone resorption → Renal Osteodystrophy
Lab Findings (Secondary HPT):
| Test | Result |
|---|---|
| Serum Calcium | LOW ↓ ya Normal |
| Serum Phosphate | HIGH ↑ (renal failure mein) |
| PTH | HIGH ↑ |
| 1,25-OH-D | LOW ↓ |
| Alkaline Phosphatase | HIGH ↑ |
Treatment:
- Underlying cause treat karo
- Active Vitamin D analog (Calcitriol / Paricalcitol)
- Cinacalcet (calcimimetic) - PTH suppress karta hai
- Phosphate binders (calcium carbonate, sevelamer)
- Parathyroidectomy (subtotal) - severe persistent cases mein
3️⃣ TERTIARY HYPERPARATHYROIDISM
- Secondary hyperparathyroidism bahut lambe arse tak rahe
- Parathyroid gland autonomous ho jaati hai (calcium levels ki parvah nahi karti)
- Calcium HIGH hone ke bawajood PTH HIGH rehta hai
- Najdi misaal: Renal transplant ke baad bhi PTH elevated rehta hai
⚖️ Comparison Table (USMLE Exam ke liye)
| Feature | Primary | Secondary | Tertiary |
|---|---|---|---|
| Calcium | HIGH ↑ | LOW/Normal | HIGH ↑ |
| PTH | HIGH ↑ | HIGH ↑ | HIGH ↑ |
| Phosphate | LOW ↓ | HIGH ↑ | Variable |
| 1,25-OH-D | HIGH | LOW | Variable |
| Cause | Adenoma/Hyperplasia | CRF, Vit D def | Long-standing 2° HPT |
| Treatment | Parathyroidectomy | Treat cause + drugs | Parathyroidectomy |
🎯 USMLE Step 2 High-Yield Points:
- PHPT = #1 cause of asymptomatic hypercalcemia (outpatients mein)
- Solitary parathyroid adenoma = 80-85% PHPT cases
- Classic triad: Bones, Stones, Groans, Moans
- X-ray clue: Subperiosteal bone resorption at radial aspect of middle phalanx
- PTH HIGH + Calcium HIGH = Primary HPT (ya FHH)
- FHH se farq: Urine Ca/Cr ratio - PHPT mein HIGH (>0.03), FHH mein LOW (<0.01)
- Surgery criteria yaad karo: Ca >1 mg/dL above normal, age <50, T-score <-2.5, CrCl <60, stones
- Cinacalcet: Medical therapy - calcium sensing receptor agonist - PTH aur Ca dono kam karta hai
- MEN-1: HPT + Pituitary tumor + Pancreatic tumor (Zollinger-Ellison)
- MEN-2A: HPT + Pheochromocytoma + Medullary thyroid cancer
- Secondary HPT mein: Calcium LOW, Phosphate HIGH (renal failure)
- Chloride:Phosphate ratio >33 = PHPT ka hint
- Brown tumors = PHPT mein bone cysts - malignancy se confuse mat karna!
- Sestamibi scan = preoperative localization ki best test
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Goldman-Cecil Medicine; Robbins & Kumar Basic Pathology; Costanzo Physiology
Hypocalcemia samjhao
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Kaafi comprehensive data aa gaya hai. Ab mukammal jawab likhta hoon.
🩺 Hypocalcemia - Mukammal Urdu Roman Wazahat
📌 Definition (Tarif)
Hypocalcemia matlab blood mein calcium ka level normal se kam hona.
| Severity | Total Serum Calcium | Ionized Calcium |
|---|---|---|
| Normal | 8.5 - 10.2 mg/dL | > 4.65 mg/dL (1.16 mmol/L) |
| Mild Hypocalcemia | 8.0 - 8.5 mg/dL | Slightly low |
| Severe Hypocalcemia | < 7.6 mg/dL (1.9 mmol/L) | Significantly low |
Important: Symptoms ionized calcium se relate hote hain, total calcium se nahi. Aur jitni tezi se calcium gire, utne zyada symptoms hote hain.
⚠️ Ek Zaroori Concept: Albumin Correction
Calcium blood mein 2 forms mein hota hai:
- Bound calcium (albumin se binda hua) - 40%
- Ionized/Free calcium (active form) - 50%
Agar albumin LOW hai (jaise cirrhosis ya nephrotic syndrome mein), to total calcium falsely low aayega - lekin ionized calcium normal hoga!
Formula (correct karne ke liye):
Corrected Ca = Measured Ca + 0.8 × (4.0 - serum albumin)
Matlab: Sirf albumin giri hui hai - real hypocalcemia nahi hai. Yeh sabse common "fake" hypocalcemia ka sabab hai.
🔢 Causes of Hypocalcemia (Asbab)
Classification: PTH ke level se decide karo
🔵 GROUP 1: PTH LOW hai (Hypoparathyroidism)
1. Post-Surgical Hypoparathyroidism (#1 Most Common Cause Overall)
- Thyroid surgery ya parathyroid surgery ke baad parathyroid glands accidentally nikal jaati hain
- Symptoms 12-24 ghante ke andar shuru
- Specially: Total thyroidectomy, radical neck dissection
2. Autoimmune Hypoparathyroidism
- Immune system parathyroid glands ko destroy kar deta hai
- Autoimmune Polyglandular Syndrome (APS type 1) = Hypoparathyroidism + Adrenal insufficiency + Mucocutaneous candidiasis (APECED syndrome)
3. DiGeorge Syndrome
- 22q11.2 deletion - chromosome 22 ka deletion
- 3rd/4th pharyngeal pouch develop nahi hote
- Parathyroid glands + Thymus ka agenesis
- Tetralogy of Fallot + Hypocalcemia + Immune deficiency (T cell) - classic triad
- Neonatal period mein hypocalcemia present hoti hai
4. Hypomagnesemia (#1 Reversible cause)
- Magnesium < 0.4 mmol/L ho to PTH ki release block ho jaati hai
- Aur PTH ke action ka resistance bhi aata hai
- Causes: Crohn disease, renal tubular disorders, alcoholism, malabsorption
- Key point: Hypocalcemia tab tak theek nahi hogi jab tak Mg correct na karo!
5. Infiltrative Diseases
- Hemochromatosis (iron deposits), Wilson disease (copper deposits)
- Amyloidosis, sarcoidosis - parathyroid glands mein infiltrate
🟠 GROUP 2: PTH HIGH hai (Secondary HPT - body compensate kar rahi hai)
1. Chronic Renal Failure (CRF) - #1 Most Common Cause Overall
- Kidney phosphate nahi nikal sakti → Hyperphosphatemia
- Hyperphosphatemia directly calcium ko suppress karta hai
- Kidney mein α1-hydroxylase kam → 1,25-OH-D (active Vit D) kam → intestinal Ca absorption kam
- PTH reactive taur par badh jaata hai (Secondary HPT)
2. Vitamin D Deficiency
- Inadequate diet ya sun exposure
- Malabsorption (celiac disease, Crohn's)
- Liver disease (25-hydroxylation nahi ho sakti)
- 25-OH-D low → calcium absorption kam → PTH badh jaata hai
3. Acute Pancreatitis
- Fat necrosis hoti hai, calcium fat ke sath "soap" bana leta hai (saponification)
- Calcium intra-abdominal fat necrosis mein chali jaati hai
- PTH normally HIGH hoti hai (compensatory)
4. Tumor Lysis Syndrome
- Cancer treatment ke baad rapidly phosphate release → hyperphosphatemia → hypocalcemia
5. Rhabdomyolysis (Early phase)
- Muscle breakdown → phosphate release → hypocalcemia
6. Bisphosphonates / Denosumab
- Bone resorption block karte hain → calcium release kam hoti hai
🔴 GROUP 3: PTH HIGH hai lekin kaam nahi kar raha (Pseudohypoparathyroidism)
Pseudohypoparathyroidism (PHP) - Albright Hereditary Osteodystrophy
- PTH banata hai, lekin target organs (kidney, bone) PTH ko respond nahi karte
- Cause: Gs-alpha protein (adenylyl cyclase) mein defect → cAMP nahi banta
- Lab: Ca LOW, Phosphate HIGH, PTH very HIGH (kyunki parathyroid zyada banane ki koshish karta hai)
- Clinical features:
- Chota qad (short stature)
- Mote/round face
- Shortened 4th/5th metacarpals (haath mein choti ungliyan)
- Mental retardation
- Calcifications (basal ganglia, subcutaneous)
- Cataracts
PHP se Hypoparathyroidism ka farq:
| Feature | Hypoparathyroidism | PHP |
|---|---|---|
| PTH | LOW | VERY HIGH |
| Response to PTH injection | urine cAMP badh jaata | urine cAMP nahi badhta |
| Body habitus | Normal | Albright features (short, round) |
😣 Symptoms & Signs (Alamat)
Main mechanism: Calcium kum hone se cell membranes ki excitability badh jaati hai - khaaskar nerves aur muscles mein.
🔴 Neuromuscular Irritability (Sabse Important)
| Sign | Detail |
|---|---|
| Paresthesias | Tingling - fingers, toes, aur munhk ke aas paas (circumoral) - pehla symptom |
| Muscle cramps | Painful spasms |
| Tetany | Involuntary muscle contractions |
| Carpopedal spasm | Haath "obstetrician's hand" mein aa jaata hai - wrist flex, MCP flex, IP extend |
| Laryngospasm | Emergency - airway block ho sakta hai → stridor → respiratory arrest |
| Seizures | Generalized tonic-clonic |
👆 2 Classic Physical Signs (USMLE favorite!)
1. Chvostek Sign:
- Facial nerve ko cheek par tap karo (tragus ke saamne)
- Positive = Ipsilateral facial muscle twitch/contraction
- (Note: 10-15% normal logon mein bhi positive ho sakta hai - low specificity)
2. Trousseau Sign (zyada specific):
- BP cuff arm par lagao, systolic se 20 mmHg zyada inflate karo, 3 minute raho
- Positive = Carpal spasm - wrist flexion, thumb adduction, finger extension
- Ischemia se neuromuscular irritability unmask hoti hai
❤️ Cardiac Changes:
- Prolonged QT interval - most important ECG finding!
- Dysrhythmia, cardiac dysfunction
- Aortic/mitral valve calcification (chronic mein)
- Generally reversible when calcium normalize hota hai
🧠 Neuropsychiatric:
- Anxiety, depression, confusion, psychosis
- Dementia (chronic mein)
- Extrapyramidal symptoms (basal ganglia calcification se - PHP mein)
- Papilledema (raised ICP)
- Seizures
👁️ Chronic Hypocalcemia ke Extra Features:
- Subcapsular cataracts (aankhon mein)
- Ectopic calcification (basal ganglia, subcutaneous)
- Abnormal dentition (daant mein problems)
- Dry skin, brittle nails, coarse hair (hypoparathyroidism mein)
🔍 Diagnosis Algorithm
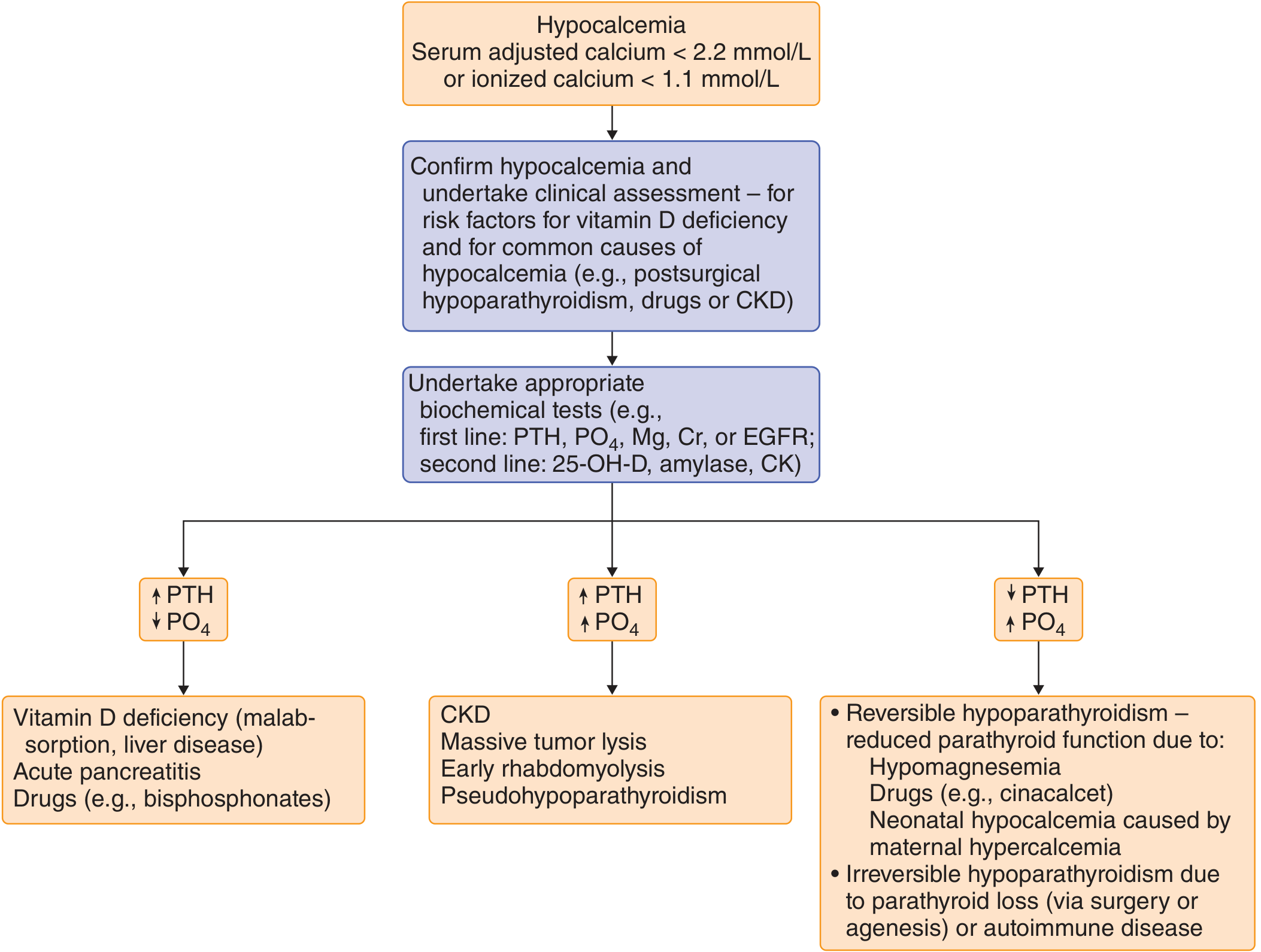
Diagram ki explanation:
Pehle hypocalcemia confirm karo, phir PTH aur Phosphate dekho:
| PTH | Phosphate | Diagnosis |
|---|---|---|
| HIGH ↑ | LOW ↓ | Vitamin D deficiency, Acute pancreatitis, Bisphosphonates |
| HIGH ↑ | HIGH ↑ | CKD, Tumor lysis, Rhabdomyolysis, Pseudohypoparathyroidism |
| LOW ↓ | HIGH ↑ | Hypoparathyroidism (surgical, autoimmune, DiGeorge, Hypomagnesemia) |
Lab Findings Summary:
| Condition | Ca | PTH | Phosphate | 25-OH-D | 1,25-OH-D |
|---|---|---|---|---|---|
| Hypoparathyroidism | LOW | LOW | HIGH | Normal | Low/Normal |
| Pseudohypoparathyroidism | LOW | VERY HIGH | HIGH | Normal | Low |
| Vit D deficiency | LOW | HIGH | LOW | LOW | LOW |
| CRF | LOW | HIGH | HIGH | Normal | LOW |
| Hypomagnesemia | LOW | LOW/Normal | Normal | Normal | Normal |
| Acute pancreatitis | LOW | HIGH | Normal | Normal | Normal |
💊 Treatment (Ilaj)
🚨 Acute / Symptomatic Hypocalcemia (Emergency):
IV Calcium Gluconate - First line!
- 10% calcium gluconate, 10 mL → 50 mL 5% dextrose mein dilute karo
- Slow IV injection: 5 minute se zyada waqt mein do (tezi se dena dangerous hai - cardiac arrest!)
- Repeat kar sakte hain zaroorat par
- Phir IV calcium infusion: 10 ampoules 1L dextrose mein - 50 mL/hr se shuru karo
Dosing insight: 1.2-1.6 mg/kg elemental calcium 4-6 ghante mein → serum Ca 2-3 mg/dL badhta hai
Calcium Chloride vs Calcium Gluconate:
- Gluconate prefer karo peripheral line mein (less irritating)
- Chloride zyada elemental calcium contain karta hai (cardiac arrest mein prefer)
Saath mein zaroor check/treat karo:
- Hypomagnesemia - pehle Mg theek karo warna Ca theek nahi hogi!
- Hyperphosphatemia
- Alkalosis (alkalosis mein ionized calcium aur bhi kam ho jaata hai)
💊 Chronic Hypocalcemia (Long-term Treatment):
1. Oral Calcium Supplements:
- 10-20 mmol calcium har 6-12 ghante mein
- Calcium carbonate (khaane ke sath - acid chahiye absorb hone ke liye)
- Calcium citrate (khaali pet bhi de sakte hain)
2. Vitamin D:
- Calcitriol (1,25-OH-D) - DRUG OF CHOICE for:
- Hypoparathyroidism
- Chronic renal failure
- Dose: 0.25 - 2 mcg/day
- Kidney mein 1-hydroxylation ki zaroorat nahi hoti
- Cholecalciferol (Vit D3) / Ergocalciferol (Vit D2): Vitamin D deficiency ke liye (10,000-50,000 units/day)
- Alfacalcidol (1α-OH-D3): Hepatic 25-hydroxylation chahiye
3. Thiazide Diuretics (special use):
- Hypoparathyroidism mein use ho sakti hai
- Urinary calcium kam karte hain (hypercalciuria aur nephrolithiasis prevent karte hain)
- Note: Hypercalcemia mein BILKUL NAHI!
4. Recombinant PTH:
- Chronic hypoparathyroidism mein - skeletal aur biochemical indices improve karta hai
Monitoring (regular follow-up):
- Pehle 1-2 hafte mein serum aur urine calcium check karo
- Phir stable hone ke baad har 3-6 mahine
- Goal: Hypercalcemia, hypercalciuria, nephrolithiasis aur renal failure AVOID karna
📊 Hypocalcemia vs Hypercalcemia - Quick Comparison
| Feature | Hypocalcemia | Hypercalcemia |
|---|---|---|
| Neuromuscular | Excitability BADHTI hai | Excitability GHATTI hai |
| Muscles | Tetany, spasm | Weakness, flaccidity |
| ECG | Long QT | Short QT |
| CNS | Anxiety, seizures | Lethargy, confusion, coma |
| GI | Nausea, vomiting | Constipation, anorexia |
| Classic signs | Chvostek, Trousseau | Bones, stones, groans, moans |
🎯 USMLE Step 2 High-Yield Points:
- #1 cause overall: Postsurgical hypoparathyroidism (thyroidectomy ke baad)
- #1 cause in CKD patients: Chronic renal failure
- Hypomagnesemia: Hypocalcemia theek karne se pehle Mg correct karo!
- Albumin low = Fake hypocalcemia - ionized calcium check karo
- Chvostek sign = facial nerve tap → facial twitch (low specificity)
- Trousseau sign = BP cuff → carpal spasm (more specific)
- ECG: LONG QT = hypocalcemia (SHORT QT = hypercalcemia)
- Alkalosis hypocalcemia ko worse banata hai (bound calcium badh jaata hai)
- DiGeorge: 22q11.2 deletion → No parathyroids + No thymus → Hypocalcemia + Immune deficiency
- Pseudohypoparathyroidism: PTH HIGH hai but organs respond nahi karte (Gs-alpha defect)
- Albright features: Short stature, round face, short 4th/5th metacarpals = PHP
- Acute treatment: IV Calcium Gluconate SLOW (5 min se zyada) - tezi se dene se cardiac arrest!
- Chronic treatment: Calcitriol (active Vit D) + Oral calcium
- Vitamin D deficiency: Ca LOW, PO4 LOW, PTH HIGH, 25-OH-D LOW, ALP HIGH
- Hypoparathyroidism: Ca LOW, PO4 HIGH, PTH LOW, Vit D normal
- PHP: Same as hypoparathyroidism EXCEPT PTH is VERY HIGH
Sources: Goldman-Cecil Medicine; Textbook of Family Medicine, 9e; Henry's Clinical Diagnosis & Management by Laboratory Methods; Robbins Pathologic Basis of Disease
Paget disease of bone yeh samjhao
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
Loading Image
Sab zaroori information aur images aa gayi hain. Ab mukammal jawab likhta hoon.
🦴 Paget Disease of Bone - Mukammal Urdu Roman Wazahat
📌 Definition (Tarif)
Paget Disease of Bone ek focal bone remodeling disorder hai jisme:
- Osteoclasts zyadati se haddi tod dete hain (bone resorption badh jaati hai)
- Iske jawab mein osteoblasts bhi zor se haddi banane lagte hain
- Lekin jo nai haddi banti hai woh disorganized, weak aur mosaic pattern mein hoti hai
- Natija: Affected haddian badi, deformed, kamzor aur fracture prone ho jaati hain
Ek sentence mein: "Bone galat tareeqe se badhti hai - zyada matra mein, lekin kam quality ki"
🌍 Epidemiology (Kon se log zyada mutasir hote hain)
- Prevalence: UK aur USA mein ~0.5% adults mein
- Western Europe (Britain, France, Germany) aur unse migrate karne wale logon mein common
- Scandinavians, Africans, Asians mein rare
- Males > Females (mard zyada mutasir)
- Age: 40 saal ke baad shuru hoti hai, umar ke sath badhti hai
- Autopsy studies: 3% logon mein jo 40+ umr ke hain
- Positive family history: 15-25% patients mein milti hai
🧬 Etiology (Cause) - Dono theories hain
1. Genetic Theory:
- SQSTM1 gene (sequestosome-1 / p62 protein) - sabse common mutation, familial aur sporadic dono mein
- TNFRSF11A - RANK gene encode karta hai
- TNFRSF11B - Osteoprotegerin encode karta hai (juvenile Paget's mein deletion)
- VCP, OPTN, TM7SF4 genes bhi implicated hain
2. Viral Theory:
- Pagetic osteoclasts mein paramyxovirus (measles, respiratory syncytial virus) jaisi inclusions milti hain
- Measles vaccination ke widespread hone ke baad Paget's ka prevalence kam hua hai - indirect support
- Lekin live virus kabhi culture nahi hua - theory controversial hai
⚙️ Pathophysiology (Kaise hota hai)
Normal bone remodeling ka RANK pathway:
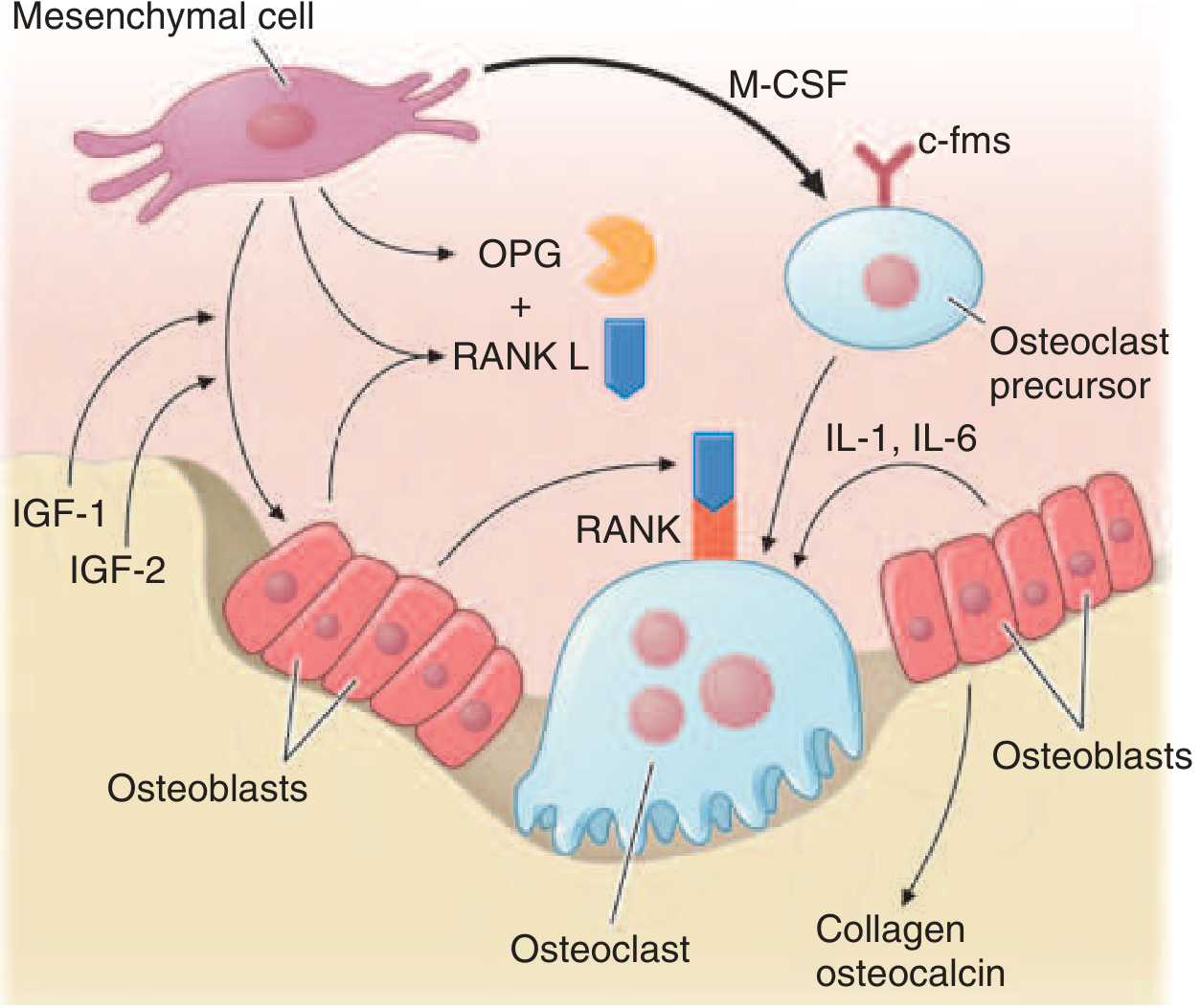
Diagram explanation:
- Mesenchymal cells RANKL banate hain → Osteoclast precursors par RANK receptor activate karta hai → Mature osteoclast banta hai (bone todta hai)
- OPG (Osteoprotegerin) RANKL ko block karta hai - brakes ka kaam karta hai
- Paget's mein: RANKL badh jaata hai, OPG kam ho jaata hai → Osteoclasts uncontrolled ho jaate hain
3 Phases of Paget's Disease:
Phase 1: OSTEOLYTIC (lytic phase)
- Overactive osteoclasts bone tod dete hain
- Extreme hypervascularization
- X-ray mein: "Blade of grass" lesion (advancing lytic wedge)
↓
Phase 2: MIXED (osteolytic + osteoblastic)
- Osteoblasts compensate karne ki koshish karte hain
- Normal lamellar bone → haphazard "WOVEN BONE" se replace
- Fibrous connective tissue marrow mein aa jaata hai
- MOST SYMPTOMATIC phase
↓
Phase 3: SCLEROTIC (burned-out phase)
- Bone resorption kam ho jaati hai
- Dense, hard, less vascular "mosaic bone" banti hai
- X-ray mein: Dense sclerotic lesions
Pagetic Osteoclasts kaisi hoti hain:
- Normal osteoclast: 3-5 nuclei
- Pagetic osteoclast: up to 100 nuclei!
- 10-100 guna zyada in number
- Resorption rate: 9 mcg/day (normal: 1 mcg/day)
Serum calcium: NORMAL rehta hai (kyunki bone formation bhi sath sath badhti hai - coupled hai)
📍 Common Sites (Kahan kahan hoti hai)
USMLE mnemonic: "Please Visit Some Famous Temples"
| Bone | Relative Frequency |
|---|---|
| Pelvis | Sabse zyada - #1 |
| Vertebral bodies | #2 |
| Skull | #3 |
| Femur | #4 |
| Tibia | #5 |
(Hands aur feet mein rare)
😣 Clinical Manifestations (Symptoms)
Aksar ASYMPTOMATIC hota hai!
- Zyada tar diagnosis routine blood test mein elevated ALP ya incidental X-ray se hoti hai
Jab symptoms hon:
🦴 Bone Pain (Sabse common symptom):
- Localized dard - affected bone mein
- Raat ko bhi rehta hai (rest pain)
- Causes: Increased vascularity, lytic lesions, microfractures, bowing
📐 Deformity:
- Tibia bowing (curved tibia) - "Sabre tibia" - most classic
- Femur bowing → chalne mein takleef, secondary osteoarthritis of hip/knee
- Skull enlargement - hat size badh jaata hai, frontal bossing
- Short stature with kyphosis aur "simian posture" (age ke sath)
- Platybasia - skull ka base soft ho jaata hai
👂 Deafness (Hearing Loss):
- Temporal bone mein Paget's → cochlear nerve compression → sensorineural deafness (rare mein conductive bhi)
- Kaan ki problems skull involvement mein common
🦷 Jaw/Dental Problems:
- Facial bones mein Paget's → teeth loose ho jaate hain, facial deformity
🔴 Neurological Complications:
- Spinal stenosis → nerve compression → radiculopathy, myelopathy
- Cranial nerve palsies - facial, oculomotor
- Brainstem compression (platybasia se)
- Rarely: Spinal cord compression
❤️ Cardiac Complications:
- Agar 15-35% skeleton involved ho aur ALP 4x normal se zyada:
- Pagetic bone mein arteriovenous shunting → excessive blood flow
- High-output cardiac failure (rare, usually sath mein cardiac disease ho toh)
- Calcific aortic stenosis
🦠 Malignant Transformation (Sabse feared complication):
- Incidence: <0.5% (rare lekin serious)
- Mostly Osteosarcoma (long bones mein, especially femur)
- Presentation: Purani Paget's lesion mein naya pain → RED FLAG
- Prognosis: Very poor
- Giant cell tumors bhi ho sakte hain - glucocorticoids se respond karte hain
🔍 Diagnosis
Lab Tests:
| Test | Result in Paget's |
|---|---|
| Serum ALP (Alkaline Phosphatase) | VERY HIGH ↑↑ - sabse important marker! |
| Serum Calcium | NORMAL (mostly) |
| Serum Phosphate | NORMAL |
| PTH | Normal |
| Urine/Serum N-telopeptide or C-telopeptide | HIGH ↑ (bone resorption marker) |
| PINP (bone formation marker) | HIGH ↑ |
| Osteocalcin | Reliable nahi hai Paget's mein |
Key point: Immobilization ke sath Paget's → rare mein hypercalcemia ho sakti hai
X-Ray Findings (Bohot important for USMLE!):
| Location | X-ray Finding |
|---|---|
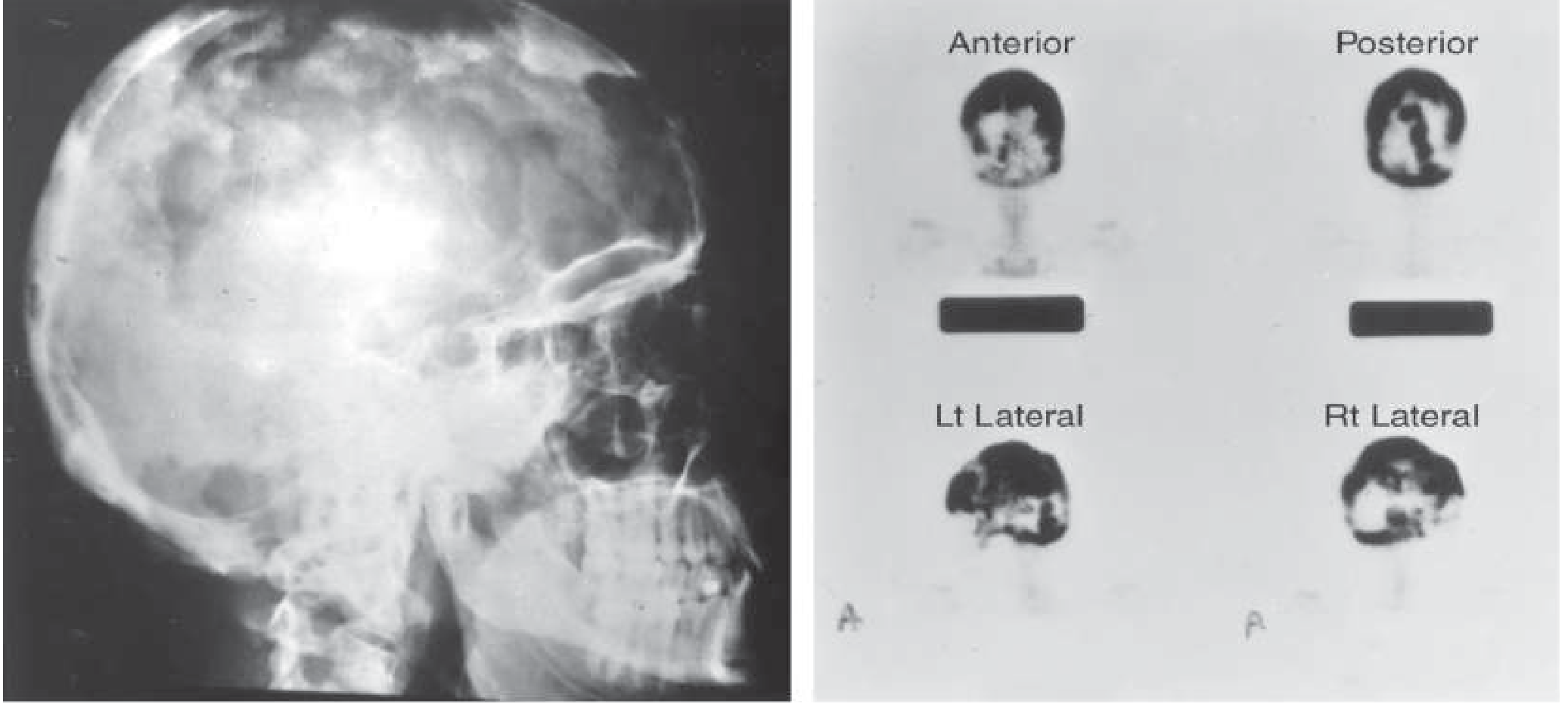
| Skull | "Cotton wool" appearance, thickened diploic layer, "osteoporosis circumscripta" (early lytic) |
| Vertebra | "Picture frame vertebra" - cortical thickening at superior/inferior endplates |
| Vertebra (diffuse) | "Ivory vertebra" - dense white vertebra |
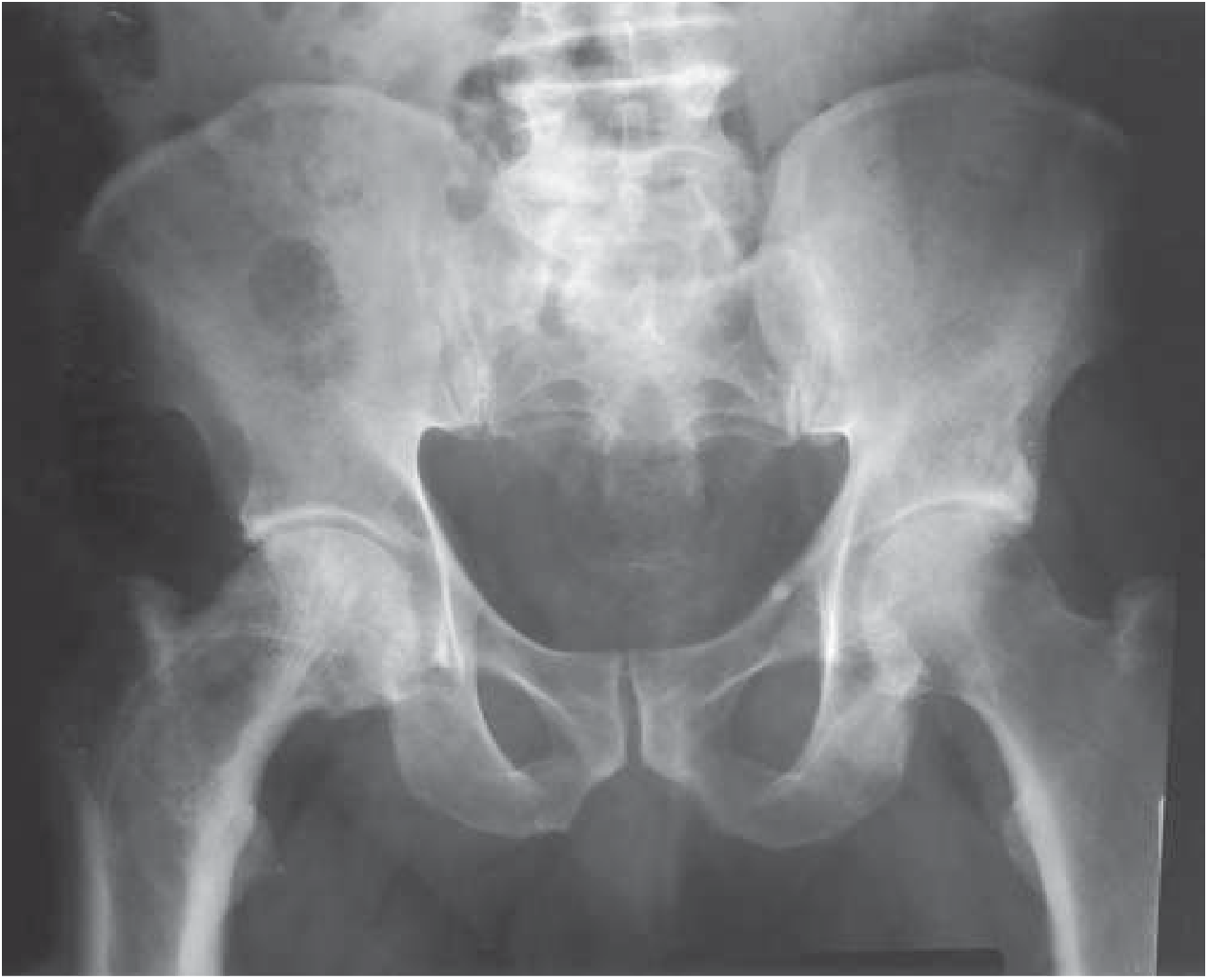
| Pelvis | Thickened iliopectineal line (brim sign), coarse trabeculation |
| Long bones | "Blade of grass" lytic lesion (early), bowing, cortical thickening |
| General | Bone enlargement/expansion (different from other bone diseases) |
Paget's skull X-ray (Cotton wool appearance):
Paget's pelvis X-ray:
Imaging Modalities:
| Test | Purpose |
|---|---|
| Plain X-ray | Diagnosis ke liye kaafi |
| Bone scan (Tc-99m) | Most sensitive - active lesions identify karne ke liye, extent of disease |
| CT | Fracture assessment |
| MRI | Sarcoma ya malignancy suspect ho toh |
| Bone biopsy | Malignancy confirm karne ke liye |
💊 Treatment (Ilaj)
Treatment kab karein?
Asymptomatic patients mein treatment zaroori nahi - watchful waiting acceptable hai. Lekin treatment zaroori hai agar:
- Bone pain jo pagetic site se related ho
- Fracture ya fracture ka high risk
- Surgery planned pagetic bone par (blood loss kam karna)
- Neurological complications (nerve compression)
- High disease activity (ALP bahut high) + involvement of skull, vertebra, ya weight-bearing bones
- Hearing loss se bachao ke liye
🥇 Drug of Choice: BISPHOSPHONATES
Bisphosphonates osteoclast activity block karte hain (RANKL pathway mein interfere karte hain)
| Drug | Dose | ALP Normalize karne ki rate |
|---|---|---|
| Zoledronic acid (Zometa) - #1 choice | 5 mg IV, 15 min mein | 90% patients mein (6 mahine mein) |
| Risedronate | 30 mg/day PO × 2 months | 73% |
| Alendronate | 40 mg/day PO × 6 months | 63% |
| Pamidronate | 30 mg/day IV × 3 days | ~50% |
| Tiludronate | 800 mg/day PO × 3 months | 35% |
| Etidronate | 200-400 mg/day PO × 6 months | 15% (least effective) |
Zoledronic acid ki khasiyat:
- Single injection - prolonged effect, effects saalon tak reh sakte hain
- Best pain response
- Treatment of choice
2. Calcitonin
- 100 U subcutaneous daily × 6-18 months
- ALP sirf 50% tak kam karta hai
- Second line - jab bisphosphonates available na hon ya contraindicated hon
⚠️ Important: Bisphosphonate se pehle zaroor do:
- Calcium + Vitamin D supplements - kyunki bone resorption suddenly block hone se "hungry bone syndrome" ho sakta hai → hypocalcemia
📊 Paget's Disease - Lab Summary
| Parameter | Value |
|---|---|
| ALP (Alkaline Phosphatase) | VERY HIGH ↑↑ |
| Serum Ca | Normal |
| Serum Phosphate | Normal |
| PTH | Normal |
| Urine hydroxyproline/telopeptides | HIGH ↑ |
| X-ray | Cotton wool (skull), picture frame (vertebra), blade of grass (long bone) |
| Bone scan | Most sensitive |
🎯 USMLE Step 2 High-Yield Points:
- Definition: Focal bone remodeling disorder - osteoclast overactivity → disorganized bone
- Most common sites: Pelvis > Vertebra > Skull > Femur > Tibia
- Calcium: NORMAL - yeh bohot important hai (hypercalcemia nahi hoti normally)
- ALP: VERY HIGH - best marker for diagnosis and monitoring
- Deafness - temporal bone involvement se cochlear nerve compression
- "Cotton wool" skull - X-ray mein classic pagetic finding
- "Picture frame vertebra" - vertebra mein cortical thickening at end plates
- "Blade of grass" - long bone mein early lytic advancing front
- "Ivory vertebra" - dense sclerotic vertebra
- Osteosarcoma - Paget's ka feared complication (<0.5%) - naya pain = RED FLAG
- Treatment: Zoledronic acid - single IV dose, 90% mein ALP normalize karta hai
- High-output cardiac failure - extensive pagetic skeleton, AV shunting
- Before bisphosphonates: Calcium aur Vitamin D zaroor do
- Immobilization + Paget's = Hypercalcemia risk
- Bone scan (Tc-99m) = most sensitive test for disease extent
- Paramyxovirus (measles) - viral theory (controversial)
- SQSTM1/p62 gene - most common mutation in familial + sporadic cases
- Males > Females, Age > 40, Western European ancestry
Sources: Harrison's Principles of Internal Medicine, 22nd Ed (2025); Goldman-Cecil Medicine; Firestein & Kelley's Textbook of Rheumatology
Hypercortisolism samjhao full detailed mai
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
Sari zaroori information aur images aa gayi hain. Ab puri tarah detailed jawab likhta hoon.
🩺 Hypercortisolism (Cushing Syndrome) - Mukammal Urdu Roman Wazahat
📌 Definition
Hypercortisolism ya Cushing Syndrome matlab blood mein cortisol ka level chronically high rehna - chahe kisi bhi wajah se.
- Cushing SYNDROME: Sare causes ki wajah se hypercortisolism (broad term)
- Cushing DISEASE: Specifically pituitary adenoma se ACTH excess → cortisol high (narrow term)
🔬 Normal HPA Axis (Samajhne ke liye zaroori)
Hypothalamus → CRH (Corticotropin Releasing Hormone)
↓
Anterior Pituitary → ACTH (Adrenocorticotropic Hormone)
↓
Adrenal Cortex (Zona Fasciculata) → CORTISOL
↓
Cortisol HIGH → Feedback inhibition → CRH aur ACTH dono suppress hote hain
Normal mein yeh feedback loop cortisol ko control karta hai. Cushing's mein yeh loop TOOT JAATA HAI.
⚡ Causes of Hypercortisolism - Classification
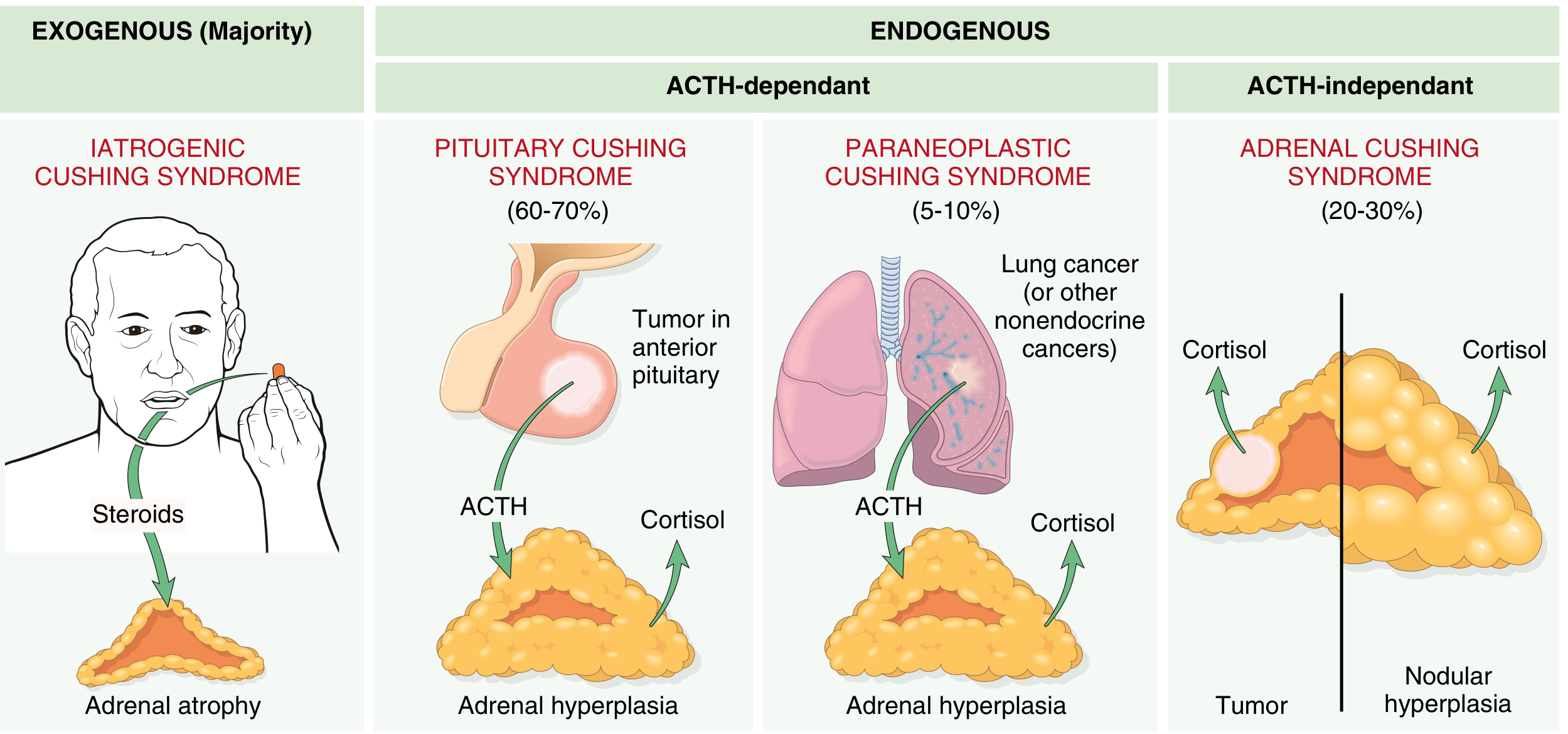
🔴 EXOGENOUS (Most Common Overall!)
- Iatrogenic Cushing's - steroids bahar se de rhe hain (doctor ne diya)
- Asthma, RA, SLE, transplant patients mein steroid therapy
- ACTH LOW, Cortisol HIGH
- Adrenal glands ATROPHY ho jaati hain (exogenous ACTH suppress karta hai)
- Yeh overall sabse common cause hai - USMLE mein pehla dhundho!
🟡 ENDOGENOUS CAUSES:
1. PITUITARY CUSHING'S DISEASE - 60-70% of endogenous
= TRUE "Cushing Disease"
- Pituitary mein ACTH-secreting adenoma (corticotroph adenoma) hota hai
- Adenoma bahut chota hota hai - mass effect nahi hota aksar
- ACTH HIGH → Bilateral adrenal hyperplasia → Cortisol HIGH
- Females 4x zyada affected, age 20-40
- ACTH-dependent Cushing's
- Adrenal glands: bilateral diffuse hyperplasia
2. ECTOPIC ACTH SYNDROME - 10-15% of endogenous
- Non-pituitary tumor ACTH banata hai
- Sabse common: Small cell carcinoma of lung
- Iske alawa: Carcinoid tumor, Medullary thyroid carcinoma, Pancreatic NETs
- ACTH bahut HIGH (pituitary se bhi zyada)
- Hypokalemia - zyada ACTH → aldosterone-like effect → K+ loss
- Hyperpigmentation - ACTH ke sath MSH (melanocyte stimulating hormone) bhi release hota hai
- Classic Cushing features kam prominent hote hain (disease tezi se chalti hai)
- ACTH-dependent Cushing's
3. ADRENAL CUSHING'S - 20-30% of endogenous
- Adrenal gland khud autonomously cortisol banati hai
- Causes: Adrenal adenoma ya adrenal carcinoma ya primary hyperplasia
- ACTH SUPPRESSED (cortisol feedback se) → dono adrenals compress
- Ek adrenal tumor → doosri adrenal atrophy
- ACTH-independent Cushing's
Causes ka Quick Summary:
| Type | ACTH | Adrenal | Common Cause |
|---|---|---|---|
| Exogenous/Iatrogenic | LOW ↓ | Atrophy | Steroid therapy |
| Pituitary (Cushing disease) | HIGH ↑ | Bilateral hyperplasia | Pituitary adenoma |
| Ectopic ACTH | VERY HIGH ↑↑ | Bilateral hyperplasia | Small cell lung Ca |
| Adrenal tumor | LOW ↓ | Unilateral tumor + contralateral atrophy | Adrenal adenoma/carcinoma |
😣 Clinical Features (Symptoms & Signs)
Cushing Syndrome ka patient - classic appearance:

🔴 1. FAT REDISTRIBUTION (Central Obesity - Sabse Characteristic)
- Truncal obesity - pet bara, haath pair patlay
- Moon face (Moon facies) - gol sootha hua chehra
- Buffalo hump - gardan ke peeche fat ka deposit (posterior neck)
- Supraclavicular fat pads - collar bone ke upar fat
- Extremities: Thin (muscle atrophy se)
Mechanism: Cortisol peripheral lipolysis + central fat redistribution karta hai
🔴 2. SKIN CHANGES
- Purple/violaceous striae - pet, janghon, kaankhon par (>1 cm wide, purple rang) - CLASSIC!
- Thin, fragile skin - skin atrophy
- Easy bruising - minor trauma se nishan pad jaate hain
- Poor wound healing - cortisol fibroblast activity suppress karta hai
- Hyperpigmentation - SIRF ectopic ACTH mein (MSH ka co-secretion)
- Acne, hirsutism (androgen excess se)
🔴 3. MUSCLE WEAKNESS (Myopathy)
- Proximal muscle weakness - upar uthhna, seedhiyan chadhna mushkil
- Type II (fast-twitch) myofibers atrophy specifically
- Thin extremities despite truncal obesity - classic finding
🔴 4. HYPERTENSION
- Diastolic hypertension - most common cardiovascular feature
- Cortisol mineralocorticoid receptors par act karta hai → sodium aur pani retain
- Renin-angiotensin system bhi stimulate hota hai
🔴 5. METABOLIC EFFECTS
- Hyperglycemia / Diabetes mellitus - cortisol gluconeogenesis badhata hai, insulin resistance
- Hypokalemia - especially ectopic ACTH mein (mineralocorticoid excess)
- Dyslipidemia - cholesterol, triglycerides badhte hain
- Metabolic alkalosis (ectopic ACTH mein)
🔴 6. BONES - Osteoporosis
- Osteoporosis - vertebral compression fractures
- Cortisol osteoblast activity suppress karta hai + calcium absorption kam karta hai
- Back pain, height loss
🔴 7. REPRODUCTIVE / GONADAL
- Females: Menstrual irregularities (oligomenorrhea/amenorrhea), infertility, hirsutism, acne
- Males: Decreased libido, erectile dysfunction, testicular atrophy
- Cortisol gonadotropins suppress karta hai
🔴 8. PSYCHIATRIC / NEUROLOGICAL
- Depression - most common psychiatric manifestation
- Anxiety, irritability, emotional lability
- Cognitive dysfunction, memory impairment
- Psychosis (severe mein)
- Fatigue (chronic)
🔴 9. IMMUNE SUPPRESSION
- Recurrent infections (bacterial, fungal)
- Lymphopenia, eosinopenia
- Cortisol T-cell proliferation block karta hai
🔴 10. EXTRA FEATURES (Ectopic ACTH mein khas)
- Hyperpigmentation - skin aur mucous membranes par (ACTH ke sath MSH release)
- Severe hypokalemia
- Metabolic alkalosis
- Rapid onset - moon face etc. kam prominent kyunki disease tez hoti hai
🔍 Diagnosis Algorithm
2 STEPS mein socho:
- Pehle CONFIRM karo ke Cushing's hai
- Phir pata karo CAUSE kya hai
STEP 1: Screening Tests (Cushing's confirm karna)
Exogenous steroids PEHLE rule out karo! (History lena - koi steroid le raha hai?)
Phir 3 tests mein se koi 2 positive hon:
| Test | Normal | Cushing's mein |
|---|---|---|
| 24-hour urinary free cortisol (3 baar karo) | Normal | 2x above normal |
| Overnight 1 mg Dexamethasone Suppression Test | Morning cortisol suppressed (<50 nmol/L) | Fail to suppress (>50 nmol/L) |
| Midnight salivary/serum cortisol | Low (physiologically lowest) | HIGH (diurnal rhythm lost) |
| Low-dose DEX test (0.5 mg q6h × 2 days) | Cortisol suppress | Cortisol nahi suppresses |
Diurnal rhythm ka concept:
- Normal mein: Cortisol subah HIGH, raat ko LOW
- Cushing's mein: Yeh rhythm KHATAM ho jaati hai - raat ko bhi cortisol high
STEP 2: Differential Diagnosis (Cause pata karna)
Sabse pehle ACTH measure karo:
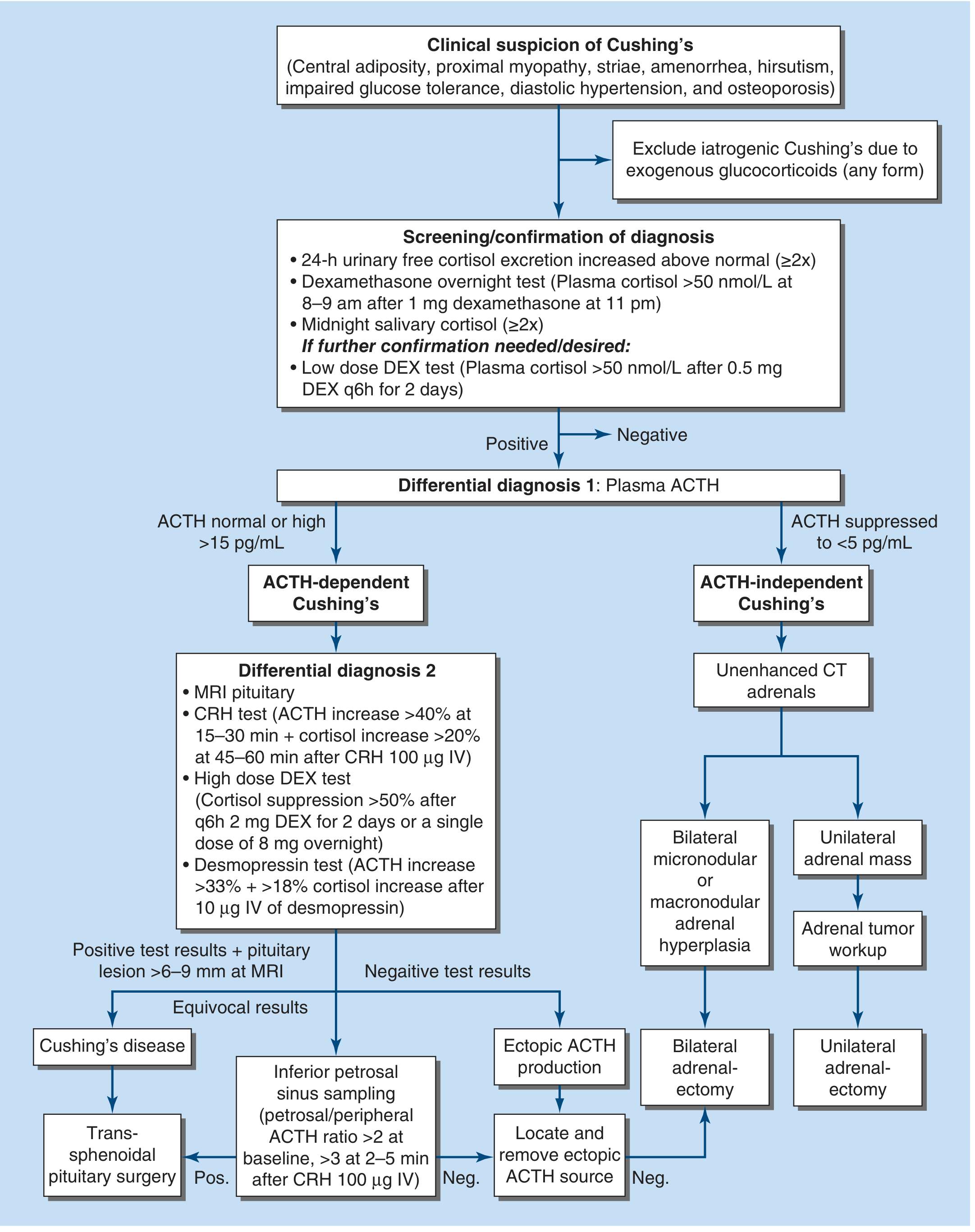
Agar ACTH suppressed (<5 pg/mL):
- → ACTH-independent = Adrenal tumor
- → Unenhanced CT adrenals karo
- Unilateral mass → Adrenal tumor
- Bilateral → Primary adrenal hyperplasia
Agar ACTH normal ya HIGH (>15 pg/mL):
- → ACTH-dependent = Pituitary ya Ectopic
- → MRI pituitary karo
Pituitary aur Ectopic mein farq karne ke tests:
| Test | Pituitary Cushing's | Ectopic ACTH |
|---|---|---|
| High-dose DEX test (8 mg overnight) | Cortisol SUPPRESS >50% | Cortisol suppress nahi hota |
| CRH stimulation test | ACTH badh jaata hai (>40%) | Response nahi |
| Inferior Petrosal Sinus Sampling (IPSS) | Central:peripheral ACTH ratio >2 (baseline), >3 after CRH | Ratio <2 |
| MRI pituitary | Adenoma dikhta hai (40% cases mein miss bhi ho sakta) | Normal |
IPSS (Inferior Petrosal Sinus Sampling):
- Sabse accurate test pituitary vs ectopic differentiate karne ke liye
- Pituitary se drain hone wali veins mein ACTH measure karte hain
- Central/peripheral ratio > 2 baseline = pituitary source confirm
Lab Summary Table:
| Iatrogenic | Pituitary | Ectopic | Adrenal Tumor | |
|---|---|---|---|---|
| Cortisol | HIGH | HIGH | HIGH | HIGH |
| ACTH | LOW ↓ | HIGH ↑ | VERY HIGH ↑↑ | LOW ↓ |
| Dex suppression (low dose) | Suppress nahi | Suppress nahi | Suppress nahi | Suppress nahi |
| Dex suppression (high dose) | Suppress nahi | SUPPRESS karta hai | Suppress nahi | Suppress nahi |
| Adrenal | Atrophy | Bilateral hyperplasia | Bilateral hyperplasia | Tumor + contralateral atrophy |
| Hyperpigmentation | No | No | YES | No |
💊 Treatment (Ilaj)
🥇 Cause ke hisaab se ilaj:
1. Exogenous/Iatrogenic:
- Steroid dose gradually taper karo (abrupt bandh karna dangerous - adrenal crisis!)
- Steroid-sparing agents use karo
2. Pituitary Cushing's Disease - DEFINITIVE TREATMENT:
- Transsphenoidal pituitary surgery (endoscopic) - 1st line
- Cure rate: 60-80% (experienced surgeon ke haath se)
- Agar surgery fail ho: Repeat surgery, Radiotherapy (fractionated ya stereotactic), Medical therapy, Bilateral adrenalectomy
3. Adrenal Tumor:
- Laparoscopic adrenalectomy - benign adenoma mein
- Open adrenalectomy - malignancy suspected ho toh
- Bilateral hyperplasia → Bilateral adrenalectomy
4. Ectopic ACTH:
- Primary tumor treat karo (lung cancer, carcinoid)
- Agar tumor na mile: Medical therapy ya bilateral adrenalectomy
💊 Medical / Drug Therapy (Cortisol kam karne ke liye):
| Drug | Mechanism | Use |
|---|---|---|
| Metyrapone | 11β-hydroxylase block → cortisol synthesis kam | Pre-op aur refractory cases |
| Osilodrostat | 11β-hydroxylase block | Approved for Cushing's |
| Ketoconazole / Levoketoconazole | Early steroidogenesis block | Medical management |
| Mifepristone (RU-486) | Glucocorticoid receptor BLOCKER | Cortisol effects block karta hai |
| Mitotane (o,p-DDD) | Adrenolytic (adrenal cells destroy karta hai) | Adrenal carcinoma + severe Cushing's |
| Etomidate (IV) | Fast 11β-hydroxylase block | Emergency/ICU mein severe Cushing's |
⚠️ Post-Surgery Consideration:
Pituitary surgery ke baad → Adrenal glands ATROPHY mein hoti hain (ACTH suppress tha) → Adrenal insufficiency ho sakti hai → Short-term steroid replacement zaroori!
Nelson Syndrome (Rare):
- Bilateral adrenalectomy ke baad agar pituitary adenoma baaki ho
- ACTH feedback remove hone se pituitary tumor grow karta hai
- Mass effects: headache, visual field defects
- Hyperpigmentation (ACTH bahut high)
🎯 USMLE Step 2 High-Yield Points:
- Most common cause overall = Exogenous steroids (Iatrogenic) - pehle poochho!
- Cushing DISEASE = specifically pituitary ACTH adenoma (60-70% endogenous)
- Ectopic ACTH = small cell lung cancer - hyperpigmentation + hypokalemia + rapid onset
- Moon face + Buffalo hump + Purple striae + Truncal obesity = classic Cushing's picture
- Purple/violaceous striae > 1 cm = Cushing's (normal striae pale/white hoti hain)
- First test: 24h urine free cortisol / Overnight 1 mg Dex suppression test
- ACTH measure karo - pituitary/ectopic (HIGH) vs adrenal/exogenous (LOW)
- High-dose Dex test: Pituitary adenoma suppress KARTA hai, ectopic nahi karta
- IPSS = most accurate for pituitary vs ectopic differentiation
- Hypokalemia + alkalosis especially in ectopic ACTH (excessive mineralocorticoid effect)
- Hyperpigmentation = ONLY ectopic ACTH ya untreated Addison's (ACTH + MSH)
- Definitive treatment: Transsphenoidal surgery (pituitary), laparoscopic adrenalectomy (adrenal)
- Post-surgery: Steroid cover zaroori - HPA axis suppressed hota hai
- Metyrapone aur Osilodrostat - 11β-hydroxylase inhibitors (cortisol kam karte hain)
- Nelson Syndrome - bilateral adrenalectomy ke baad pituitary tumor grow karna
- Osteoporosis Cushing's mein - vertebral fractures common
- Diurnal rhythm loss - midnight cortisol HIGH = sensitive marker
- Proximal muscle weakness - characteristic (type II fiber atrophy)
- Pseudo-Cushing's = alcohol excess, obesity, depression mein bhi cortisol high - dex test se distinguish
- Crooke hyaline change - histology mein pituitary ACTH cells ka characteristic finding
Sources: Robbins & Kumar Basic Pathology; Harrison's Principles of Internal Medicine, 22nd Ed (2025); Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.