Circle of willis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the Circle of Willis drawn from multiple authoritative medical textbooks.
Circle of Willis
Overview
The circle of Willis (circulus arteriosus cerebri) is an anastomotic ring of arteries at the base of the brain that connects the anterior circulation (internal carotid arteries) and the posterior circulation (vertebrobasilar system). All major cerebral vessels arise from it, and it serves as the primary collateral pathway for cerebral blood flow. - Neuroanatomy through Clinical Cases, 3rd Ed.
Anatomy and Components
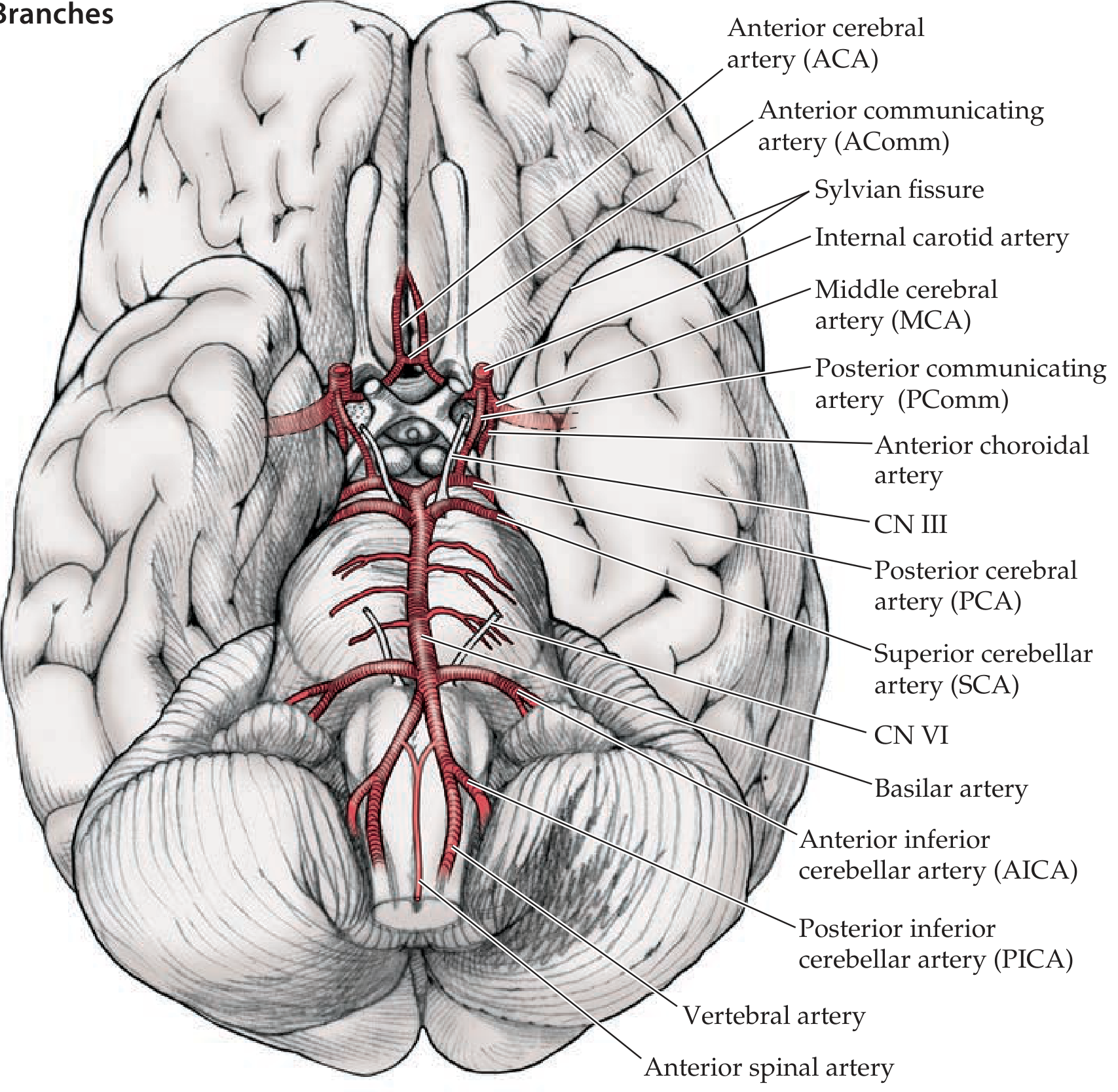
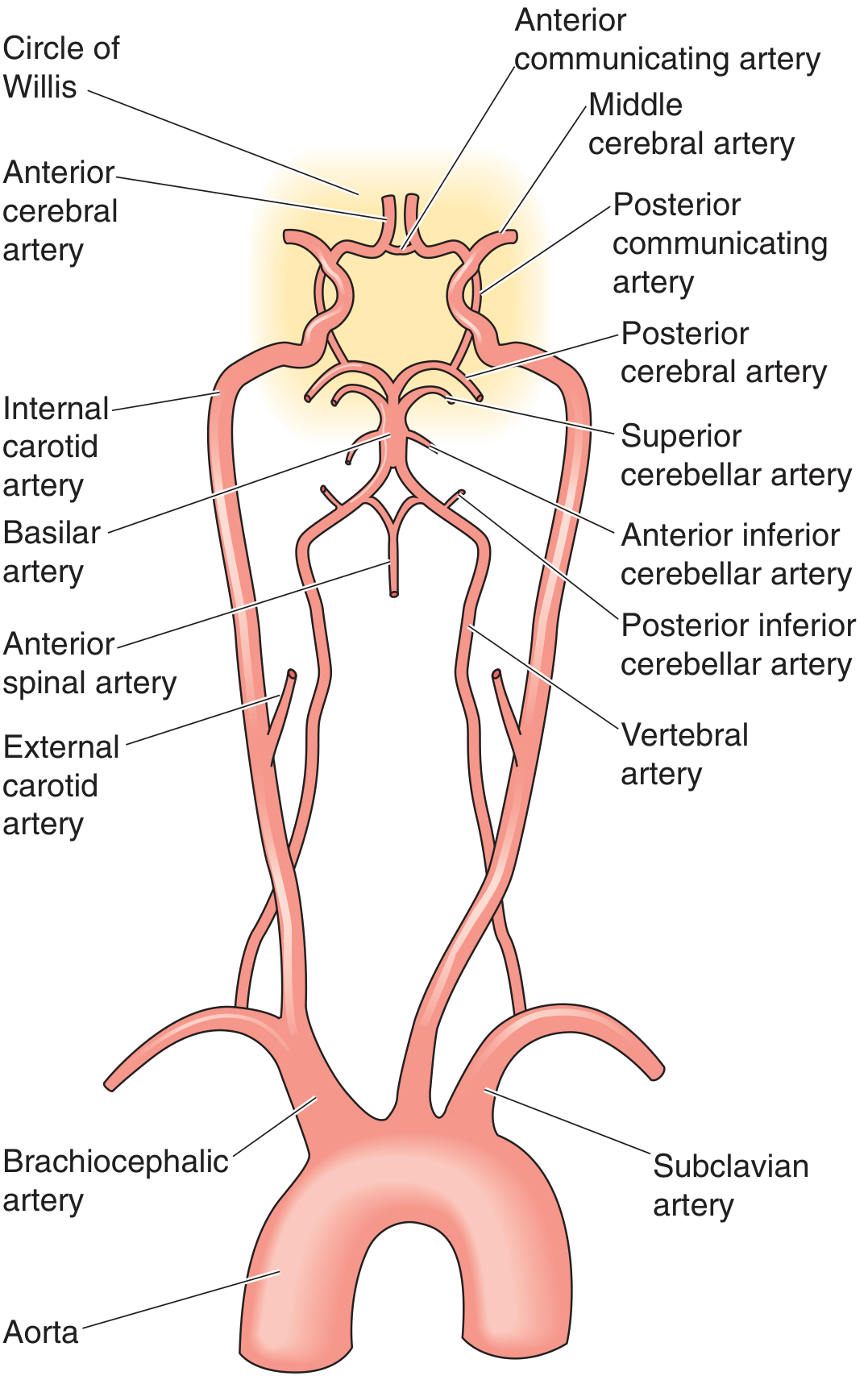
The circle is formed by 7 major vessels arranged in a heptagonal shape on the ventral surface of the brain:
Anterior part (from the internal carotid arteries):
- Bilateral Internal Carotid Arteries (ICA) - each splits into ACA and MCA
- Bilateral Anterior Cerebral Arteries (ACA) - A1 segments
- Single Anterior Communicating Artery (AComm) - connects the two ACAs
Posterior part (from the vertebrobasilar system):
- Bilateral Vertebral Arteries - arise from subclavian arteries, join to form the basilar artery
- Single Basilar Artery - formed at the pontomedullary junction
- Bilateral Posterior Cerebral Arteries (PCA) - terminal branches of the basilar artery
Connecting links:
- Bilateral Posterior Communicating Arteries (PComm) - join the ICAs to the PCAs, linking anterior and posterior circulations
The main branches of the supraclinoid ICA can be remembered by the mnemonic OPAAM: Ophthalmic, Posterior communicating, Anterior choroidal, Anterior cerebral, and Middle cerebral arteries. - Neuroanatomy through Clinical Cases, 3rd Ed.
Completeness and Anatomical Variants
A full-caliber, complete circle of Willis is present in only approximately 34% of individuals - Neuroanatomy through Clinical Cases, 3rd Ed. Barash's Clinical Anesthesia further notes that autopsy studies show the majority of specimens have anatomic anomalies: hypoplasia is the most frequently noted anomaly (24%), and complete absence of a vessel causing an incomplete circle occurs in an additional 6%.
Common variants include:
- Hypoplastic or absent communicating arteries
- Bilateral ACA supply from one carotid (one AComm supplying both)
- Fetal origin of the PCA (PCA arising from the ICA instead of the basilar artery)
- One dominant vertebral artery with contralateral hypoplasia
These variants are clinically significant - they can make occlusion of a particular vessel far more devastating than it would be in a patient with complete collateral circulation. - Schwartz's Principles of Surgery, 11th Ed.
Blood Supply Territories
| Artery | Region Supplied |
|---|---|
| ACA | Medial frontal and parietal cortex (including medial sensorimotor cortex for the lower limb) |
| MCA | Lateral convexity: frontal, parietal, temporal lobes; internal capsule, basal ganglia (lenticulostriate branches) |
| PCA | Occipital lobe, inferior temporal lobe, thalamus, midbrain |
| Lenticulostriate aa. (from MCA) | Basal ganglia, internal capsule (deep penetrating) |
| Anterior choroidal a. (from ICA) | Posterior limb of internal capsule, optic tract, hippocampus |
Deep structures (basal ganglia, thalamus, internal capsule) are supplied by small penetrating branches from the proximal segments of the main cerebral arteries near the circle of Willis. - Neuroanatomy through Clinical Cases, 3rd Ed.
Role in Collateral Circulation
The circle of Willis is the primary of three main collateral pathways for brain perfusion:
- The circle of Willis itself (connecting carotid and vertebrobasilar systems)
- Extracranial-intracranial anastomoses (e.g., ECA branches anastomosing with intracranial vessels)
- Leptomeningeal anastomoses (between terminal branches of major cerebral arteries)
- Localization in Clinical Neurology, 8th Ed.
Patients with complete proximal carotid occlusion may be entirely asymptomatic if a complete circle of Willis allows contralateral and posterior collateral flow to compensate. Conversely, an incomplete circle can make carotid occlusion catastrophic. - Schwartz's Principles of Surgery, 11th Ed.
Clinical Significance
Berry (Saccular) Aneurysms
The circle of Willis is the most common site for intracranial saccular aneurysms, forming at vessel bifurcations due to hemodynamic stress and medial defects. The frequency distribution of aneurysms is shown below:
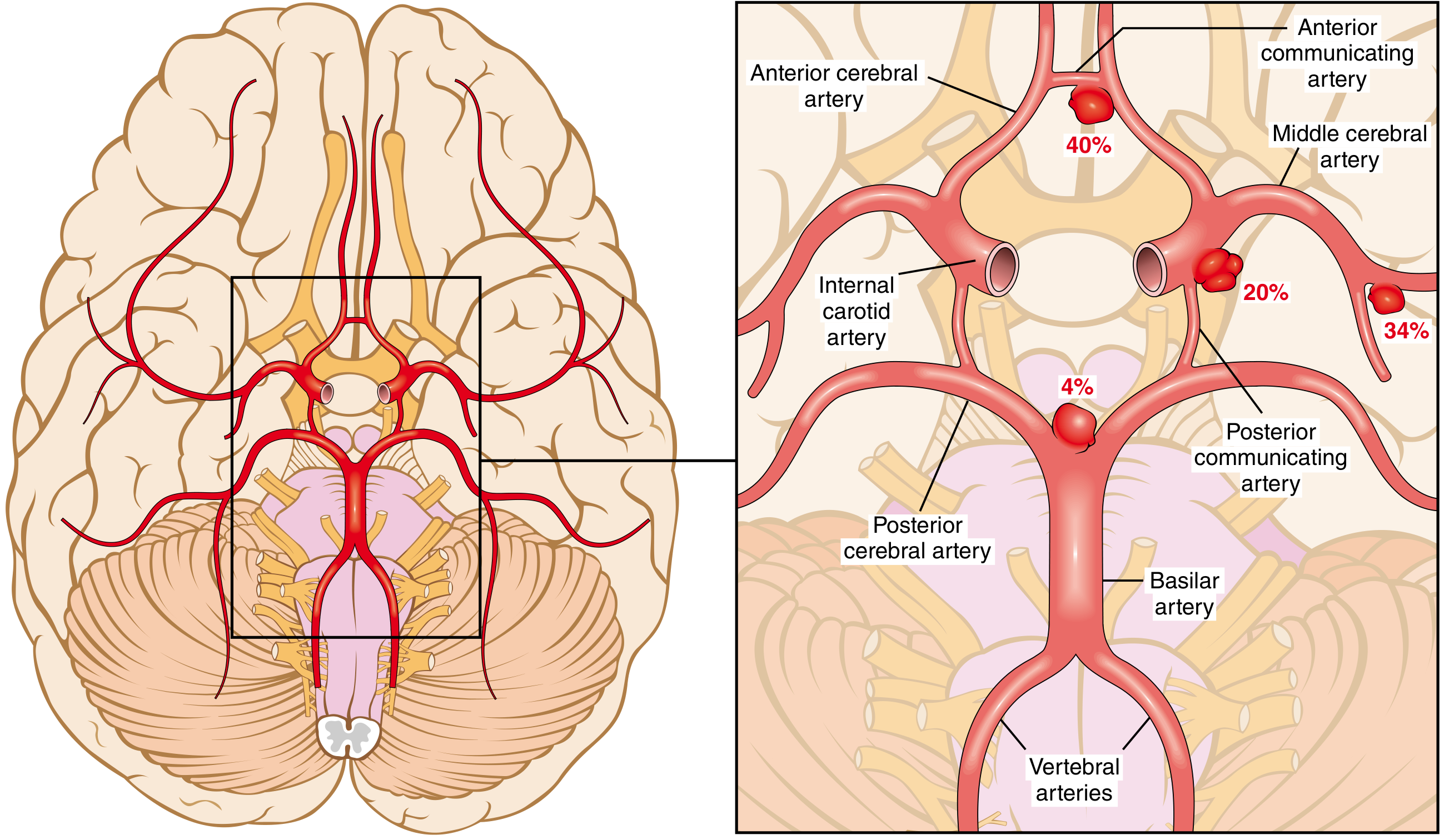
- Anterior communicating artery (AComm): ~40% - most common overall
- Middle cerebral artery bifurcation: ~34%
- Internal carotid / PComm junction: ~20%
- Basilar tip / PCA: ~4%
Rupture causes subarachnoid hemorrhage (SAH). Blood in the basal subarachnoid space can trigger vasospasm of the major vessels of the circle of Willis, driven by endothelins, nitric oxide, and arachidonic acid metabolites, causing secondary ischemic injury days after the initial bleed. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Stroke
- Occlusion proximal to the circle of Willis may be tolerated due to collateral rerouting
- Occlusion distal to the circle of Willis typically causes infarction in that artery's territory
- 85% of acute cerebrovascular events are ischemic strokes; collateral status is a key determinant of clinical outcome - Schwartz's Principles of Surgery, 11th Ed.
Carotid Endarterectomy (CEA)
During carotid cross-clamping, the ipsilateral hemisphere depends entirely on collateral flow through the circle of Willis. An incomplete circle (present in the majority of patients) may necessitate intraoperative shunting. - Barash's Clinical Anesthesia, 9th Ed.
CN III Compression
A posterior communicating artery aneurysm classically compresses CN III as it runs adjacent to it, causing a painful third nerve palsy with a dilated, "blown" pupil (pupil-involving CN III palsy) - a neurosurgical emergency.
Key Summary Table
| Component | Origin | Connects |
|---|---|---|
| AComm | ACA-ACA junction | Left and right anterior circulation |
| PComm (bilateral) | ICA to PCA | Anterior to posterior circulation |
| Basilar artery | Convergence of 2 vertebrals | Posterior circulation to PCAs |
| ACA (bilateral) | ICA terminal branch | Medial hemisphere supply |
| MCA (bilateral) | ICA terminal branch | Lateral hemisphere supply |
| PCA (bilateral) | Basilar terminal branch | Posterior hemisphere/brainstem supply |
Sources: Neuroanatomy through Clinical Cases 3rd Ed. | Schwartz's Principles of Surgery 11th Ed. | Barash's Clinical Anesthesia 9th Ed. | Robbins, Cotran & Kumar Pathologic Basis of Disease | Localization in Clinical Neurology 8th Ed. | Medical Physiology (Boron & Boulpaep)
This is a shared conversation. Sign in to Orris to start your own chat.