femoral, umbilical and paraumbilical hernias
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from the textbooks. Let me compile the full answer.
Femoral, Umbilical, and Paraumbilical Hernias
FEMORAL HERNIA
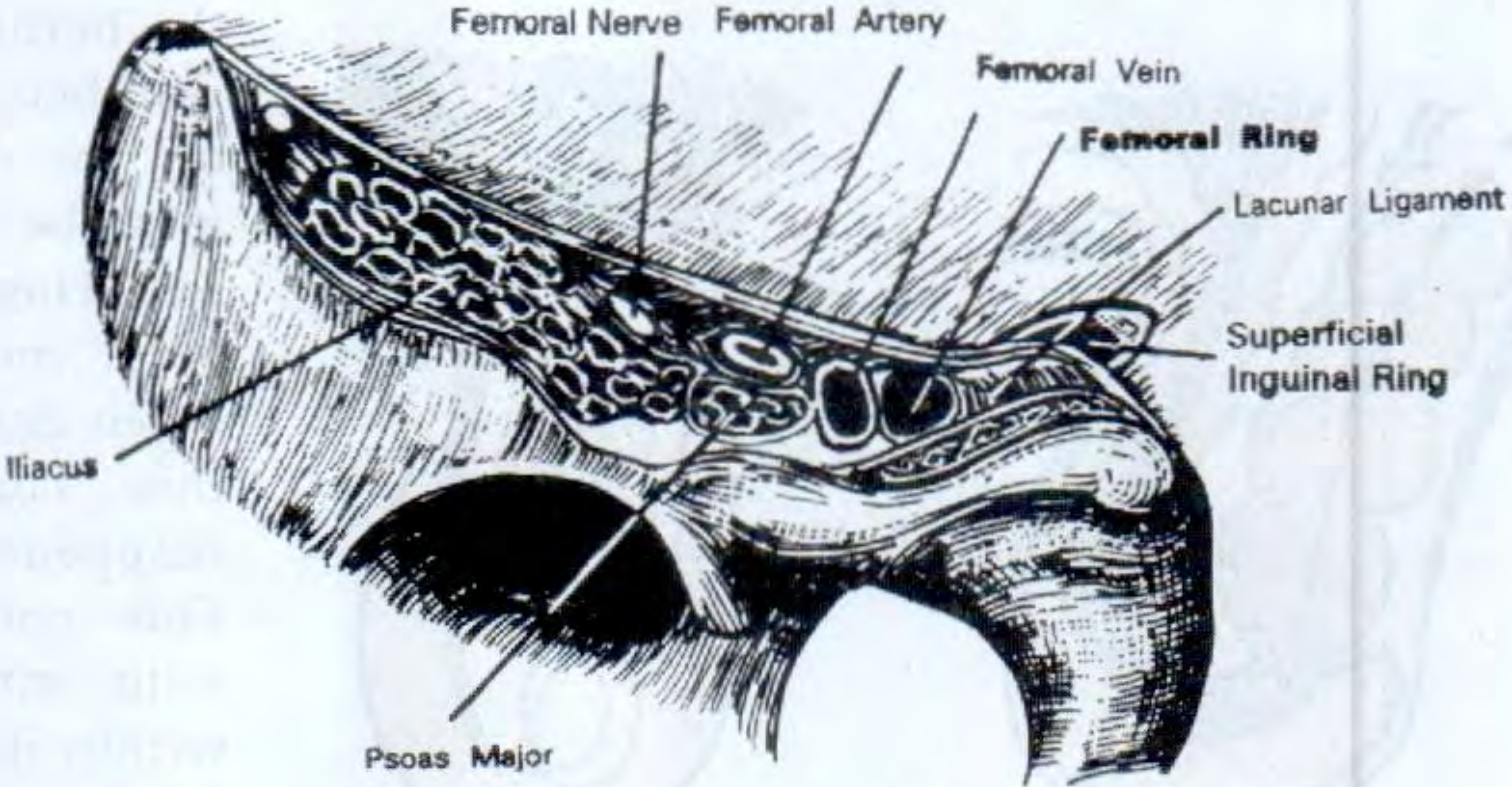
Anatomy of the Femoral Canal
A femoral hernia is a protrusion of extraperitoneal tissue, peritoneum, and sometimes abdominal contents through the femoral canal. The boundaries of the femoral canal are:
| Boundary | Structure |
|---|---|
| Anterior/superior | Inguinal ligament |
| Posterior/inferior | Pubic ramus and pectineus muscle (Cooper's/iliopectineal ligament) |
| Medial | Lacunar (Gimbernat's) ligament — sharp, unyielding edge |
| Lateral | Femoral vein |
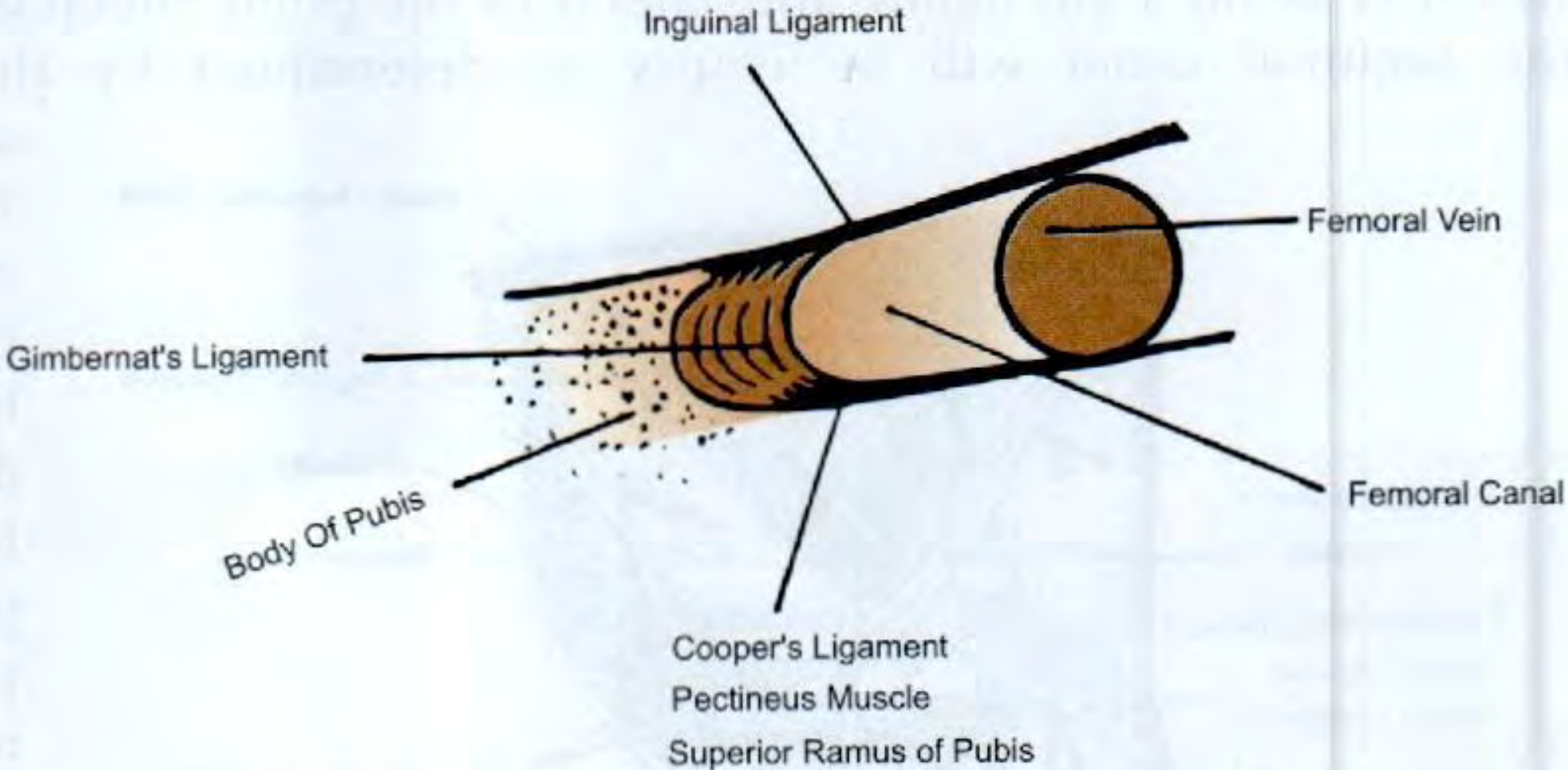
The hernia exits superficially through the saphenous opening (~4 cm below and lateral to the pubic tubercle). Once through this opening, it expands into loose areolar tissue and can curve upward above the inguinal ligament — giving it the classic retort shape.
Epidemiology
- Rare before age 20; peak incidence >50 years
- More common in women (2:1), but inguinal hernia remains the commonest groin hernia even in women
- Right > left (2:1); bilateral in ~20%
- The female pelvis is wider, enlarging the femoral canal
- Because the canal is a rigid opening, strangulation is very common — ~50% present as emergencies
Clinical Features & Diagnosis
- Swelling below and lateral to the pubic tubercle, below the inguinal ligament
- May extend superiorly and be confused with a direct inguinal hernia
- Often rapidly becomes irreducible and loses cough impulse (tight neck)
- Can be as small as 1–2 cm and mistaken for a lymph node
- The inguinal canal is empty on invagination test
Key distinguishing points from inguinal hernia:
- Femoral: below and lateral to pubic tubercle; cough impulse at saphenous opening
- Inguinal: above the inguinal ligament and medial to pubic tubercle
- Occluding the deep inguinal ring stops an indirect inguinal hernia but not a femoral hernia
Differential Diagnosis
- Saphena varix — disappears on lying flat; fluid thrill on Schwartz's test (percussion of varicosities transmits upward impulse)
- Enlarged lymph nodes — including Cloquet's node in the femoral canal; search for a distal focus of infection
- Psoas abscess — lateral to femoral vessels; cold fluctuant swelling, reducible, associated with Pott's disease
- Femoral artery aneurysm — pulsatile, expansile
Treatment — Surgery is Mandatory (no alternative)
Three open approaches:
| Approach | Description | Best for |
|---|---|---|
| Low (Lockwood) | Transverse incision over hernia; reduce contents and sac; non-absorbable sutures between inguinal and pectineal ligaments | Elective; suitable for local anaesthesia |
| Inguinal (Lotheissen) | Same incision as Bassini/Lichtenstein; transversalis fascia opened; hernia reduced from above; neck closed with sutures or mesh plug | Elective |
| High (McEvedy/Nyhus) | Transverse incision above inguinal canal; preperitoneal approach; allows bowel inspection and resection | Emergency — risk of strangulation; requires GA/RA |
Laparoscopic repair (TEP/TAPP) is also appropriate for selected cases.
UMBILICAL HERNIA
Classification (S Das)
Four varieties of hernia related to the umbilicus:
- Exomphalos — abdominal contents protrude into umbilical cord, covered by transparent membrane; congenital
- Congenital umbilical hernia — protrudes through the centre of a congenital weak umbilical scar; common in African infants; wide neck → low strangulation risk; ~90% resolve spontaneously within 5 years
- Acquired umbilical hernia — protrudes through the umbilical scar in adult life due to raised intra-abdominal pressure (pregnancy, ascites, ovarian cyst, bowel distension)
- Para-umbilical hernia — see below (commonest acquired type)
Umbilical Hernia in Children
- Occurs in up to 10% of infants (higher in premature and Black infants)
- Appears within weeks of birth; classic conical shape that enlarges on crying
- Obstruction/strangulation extremely uncommon before age 3
- Treatment: conservative under age 2 — 95% resolve spontaneously; surgical repair if persists beyond 2 years
Surgery (children): Small curved infra-umbilical incision; sac opened, contents reduced, sac closed, linea alba defect closed with interrupted slowly absorbable sutures.
Umbilical Hernia in Adults
- Predisposing conditions: obesity, pregnancy, liver cirrhosis with ascites
- Small hernias contain extraperitoneal fat or omentum; larger ones contain bowel
- Narrow neck relative to sac → prone to irreducibility, obstruction, strangulation
- Bulge typically slightly to one side of the umbilical depression → crescent-shaped appearance

Treatment: Surgery advised when hernia contains bowel; small asymptomatic hernias may be observed.
Open repair:
- Defects <1 cm: simple suture or darn technique
- Defects up to 2 cm: Mayo repair — transverse incision, reduce contents, close peritoneum, extend defect transversally, overlap fascial edges ("waistcoat over trousers" fashion) with non-absorbable sutures
- Defects >2 cm: mesh repair strongly recommended (lower recurrence)
Special considerations:
- Pregnancy-related: encourage weight loss and core strengthening postpartum; avoid surgery during pregnancy
- Liver cirrhosis (Child's B/C): very high surgical mortality; requires hepatology support; continuous sutures to minimise ascites leak
PARAUMBILICAL HERNIA
A paraumbilical hernia protrudes not through the umbilicus itself but through a defect in the linea alba adjacent to it — most commonly just above the umbilicus between the two rectus muscles. The lower half of the sac is often covered by the umbilicus itself.
Note: Under current guidelines (Bailey & Love, 28th Ed.), any hernia in the immediate vicinity of the umbilicus can be classified as "umbilical." The term "paraumbilical" is still widely used clinically.
Features
| Feature | Detail |
|---|---|
| Commonest acquired umbilical hernia | Most frequent type in adults |
| Demographics | Middle/old age; obese women predominantly affected |
| Symptoms | Pain and swelling (if small, pain/discomfort dominate) |
| Consistency | Firm if omentum; soft and resonant if bowel |
| Neck | Firm fibrous edge of linea alba defect (felt on reduction) |
| Reducibility | Many become irreducible — contents adhere to sac or narrow neck |
| Strangulation | Less common than obstruction, but defect does not enlarge proportionately → intermittent abdominal pain |
Treatment
Same principles as adult umbilical hernia:
- Surgical repair with Mayo technique (overlap) or mesh repair
- Laparoscopic/robotic preperitoneal repair is increasingly used for midline paraumbilical hernias
- Mesh recommended for all defects >2 cm
Key Comparisons at a Glance
| Feature | Femoral | Umbilical (adult) | Paraumbilical |
|---|---|---|---|
| Location | Below/lateral to pubic tubercle | Through umbilical ring | Adjacent to (usually above) umbilicus |
| Sex predominance | Women > men | Women > men | Obese middle-aged women |
| Strangulation risk | Very high (rigid canal) | High (narrow neck) | Moderate (less common) |
| Spontaneous resolution | Never | Only in children | Never |
| Emergency rate | ~50% | Significant | Less frequent |
| Repair | Lockwood / Lotheissen / McEvedy / Laparoscopic | Mayo / mesh / laparoscopic | Mayo / mesh / laparoscopic |
Sources: Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 64; S Das A Manual on Clinical Surgery, 13th Ed., Ch. 38
This is a shared conversation. Sign in to Orris to start your own chat.