Guidelines and Rx for projectile vomiting
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive overview of projectile vomiting — its causes, evaluation, and management.
Projectile Vomiting
Definition & Mechanism
Projectile vomiting is sudden, forceful emesis — typically without warning — caused by powerful gastric contractions overcoming outflow obstruction, or by direct stimulation of the emetic center. It is distinct from ordinary regurgitation (passive effortless reflux) and standard vomiting (preceded by nausea). — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Key Causes
1. Hypertrophic Pyloric Stenosis (HPS) — Most Common in Infants
The classic cause of projectile vomiting. Progressive smooth muscle hypertrophy of the pylorus causes gastric outlet obstruction.
| Feature | Details |
|---|---|
| Incidence | ~1 in 250 live births |
| Sex | Males 4× more affected |
| Age of onset | 2–6 weeks of life (peak 5th week, up to 10 weeks) |
| Vomiting character | Nonbilious, projectile, immediately post-feed |
| Appetite | Ravenous ("hungry vomiter") |
| Risk factors | First-born, white race, family history, macrolide antibiotic exposure, prematurity |
Exam findings:
- Palpable firm, mobile "olive" in right upper/mid-epigastrium (pathognomonic when present)
- Visible peristaltic waves left → right across the abdomen
Labs: Hypochloremic, hypokalemic metabolic alkalosis (gastric acid loss); serum HCO₃⁻ ≥29 mmol/L, Cl⁻ ≤98 mmol/L
2. Increased Intracranial Pressure (ICP)
A sudden rise in ICP (e.g., from subarachnoid hemorrhage, posterior fossa tumors, hydrocephalus) can directly stimulate the floor of the fourth ventricle, producing sudden "projectile" vomiting without warning or preceding nausea. In children with posterior fossa tumors, vomiting may occur without headache. Adults may awaken with severe headache followed by projectile vomiting. — Plum and Posner's Diagnosis and Treatment of Stupor and Coma
Think of this cause when: vomiting is accompanied by headache, altered consciousness, papilledema, or focal neurologic signs.
3. Other Causes in Infants/Neonates
| Condition | Distinguishing Feature |
|---|---|
| Malrotation with midgut volvulus | Bilious vomiting; surgical emergency |
| Duodenal atresia | Bilious vomiting at birth; associated with trisomy 21 |
| Intussusception | Colicky pain, currant-jelly stools; ages 3–12 months |
| Tracheoesophageal fistula | Vomiting from birth |
Diagnosis of HPS
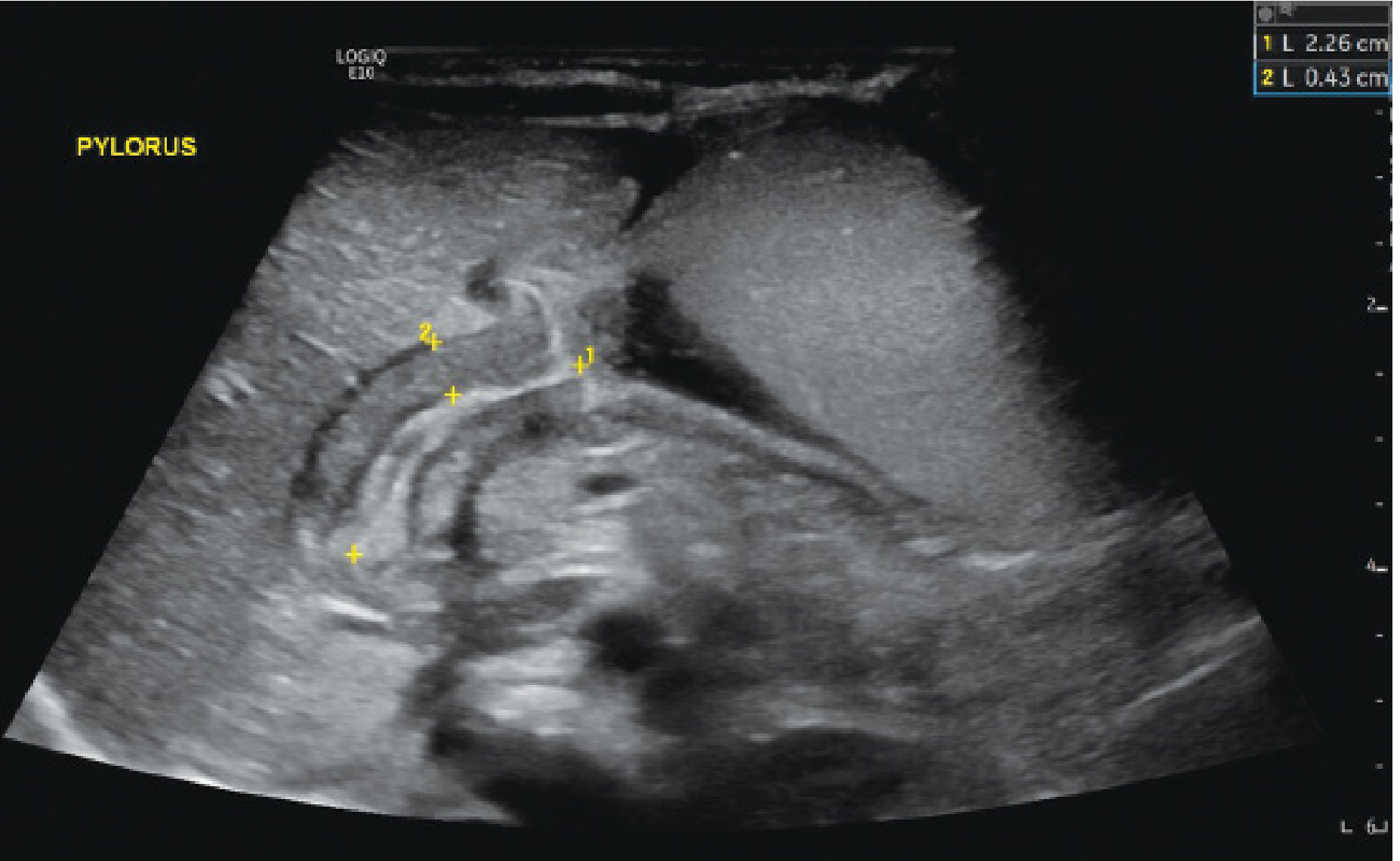
Ultrasound (first-line):
- Pyloric muscle thickness ≥4 mm
- Pyloric channel length ≥15–19 mm
- Pyloric diameter >14 mm
- Sensitivity/specificity >95%
Upper GI contrast series (alternative): Shows the "string sign" — contrast through the narrowed pyloric channel. Useful when bilious vomiting raises concern for more distal obstruction.
Plain films: Distended, air-filled stomach in advanced obstruction.
Management of HPS
HPS is not a surgical emergency — it is a fluid and electrolyte emergency. Correct metabolic derangements before operating.
Step 1 — Resuscitation (ED/Pre-op)
| Intervention | Detail |
|---|---|
| IV fluid bolus | Normal saline 20 mL/kg repeated as needed for dehydration/shock |
| Potassium replacement | KCl 0.5–1 mEq/kg IV over 1–2 hours |
| Electrolyte targets before OR | Serum Cl⁻ ≥90–95 mEq/L; serum CO₂ <30 mEq/L |
Step 2 — Surgery: Ramstedt Pyloromyotomy
- A single longitudinal incision through the hypertrophied pyloric muscle (not through mucosa)
- The submucosa must bulge into the myotomy site and both muscle edges must be freely mobile
- Can be performed open (Ramstedt) or laparoscopically — both have >95% success; laparoscopic approach is now standard at most pediatric centers
Post-op:
- Feeds started within 6–8 hours after anesthesia recovery
- Most infants tolerate feeds and are discharged within 24 hours
- Mortality is extremely rare in the absence of comorbid disease
Disposition
Admit all symptomatic infants for rehydration, electrolyte correction, imaging, and surgical consultation. Well-appearing, non-dehydrated infants may be managed with outpatient surgical planning, but this is uncommon. — Rosen's Emergency Medicine
Differential: Projectile Vomiting by Age
| Age Group | Top Causes |
|---|---|
| Neonate (0–2 wk) | Tracheoesophageal fistula, duodenal atresia, malrotation |
| Infant (2–12 wk) | Pyloric stenosis (nonbilious), malrotation (bilious = emergency) |
| Infant (3–12 mo) | Intussusception, pyloric stenosis (late), gastroenteritis |
| Any age | ↑ICP (tumor, hemorrhage, hydrocephalus), sepsis, meningitis, metabolic disorders |
Key red flags requiring urgent action:
- Bilious vomiting in an infant → malrotation with volvulus until proven otherwise
- Neurologic signs + projectile vomiting → ↑ICP workup (CT/MRI, neurosurgery)
- Ill-appearing or hemodynamically unstable infant → resuscitate and consult surgery immediately
This is a shared conversation. Sign in to Orris to start your own chat.