

1000045401.jpg
1000045402.jpg
Make detail and easy to understand notes as a nursing student in points in each topic
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have excellent textbook diagrams and content. Here are your complete, detailed nursing notes:
📚 ADMINISTRATION OF MEDICATIONS
Complete Nursing Notes
TOPIC 1: INTRODUCTION
A. Definition of Medication
- A medication (drug) is any substance that, when taken into or applied to the body, changes or affects body function
- Drugs can be used to diagnose, treat, cure, prevent disease, or provide symptom relief
- Medications can be natural (plant, animal, mineral origin) or synthetic (chemically manufactured)
B. Drug Nomenclature (Naming of Drugs)
Every drug has 3 names:
| Name | Description | Example |
|---|---|---|
| Chemical name | Exact chemical formula | N-acetyl-para-aminophenol |
| Generic name | Official non-proprietary name | Paracetamol / Acetaminophen |
| Brand/Trade name | Manufacturer's name (has ®) | Crocin, Calpol, Tylenol |
- Nurses should always know the generic name - it is universal and used globally
- One generic drug can have many brand names from different companies
C. Effects of Drugs
- Therapeutic effect - the desired, intended action of the drug (e.g., paracetamol reduces fever)
- Side effect - unintended but predictable effect at normal dose (e.g., drowsiness with antihistamines)
- Adverse effect - harmful, unintended effect, more severe than side effect (e.g., liver damage with paracetamol overdose)
- Toxic effect - dangerous effect due to overdose or drug accumulation in the body
- Allergic reaction - immune response to the drug (rash, itching, anaphylaxis)
- Idiosyncratic effect - unusual/unexpected reaction specific to an individual (due to genetics)
- Drug interaction - one drug alters the effect of another drug
- Synergism: two drugs together are MORE effective than individually
- Antagonism: one drug reduces/blocks the effect of another
D. Forms of Medications
Solid Forms:
- Tablet - compressed powder; most common oral form
- Capsule - drug enclosed in gelatin shell
- Enteric-coated tablet - has a coating that prevents dissolving in the stomach (protects stomach); dissolves in the intestine. Example: aspirin, omeprazole
- Extended-release (ER/SR/XR/CR) - releases drug slowly for prolonged action; dosed less frequently; improves patient compliance
- Suppository - solid at room temperature, melts at body temperature; for rectal or vaginal use
Liquid Forms:
- Solution - drug fully dissolved in liquid
- Suspension - drug particles mixed (not dissolved) in liquid - must be shaken before use
- Elixir - drug dissolved in sweetened alcohol solution
- Syrup - drug in concentrated sugar solution
- Emulsion - fat droplets dispersed in water
Other Forms:
- Ointment/Cream/Gel/Lotion/Patch - topical applications
- Powder - for reconstitution
- Aerosol/Inhaler - for inhalation
E. Purposes of Medication Administration
- Curative - to cure a disease (antibiotics for infection)
- Preventive/Prophylactic - to prevent disease (vaccines, malaria prophylaxis)
- Diagnostic - to diagnose disease (contrast dye for imaging)
- Palliative - to relieve symptoms without curing (morphine for pain)
- Replacement/Substitution - to replace missing body substances (insulin for diabetes, thyroxine for hypothyroidism)
- Restorative - to restore normal body function
TOPIC 2: PHARMACODYNAMICS AND PHARMACOKINETICS
A. Pharmacokinetics - "What the body does to the drug"
Remember with the acronym ADME:
1. Absorption
- Process by which drug moves from site of administration into the bloodstream
- Factors affecting absorption:
- Route of administration (IV = 100% absorbed; oral = variable)
- Drug solubility (lipid-soluble drugs absorb better)
- pH of GI tract (some drugs destroyed by stomach acid)
- First-pass metabolism - oral drugs absorbed from gut go to the liver FIRST before reaching systemic circulation; liver may break down the drug significantly, reducing its effective dose
- Blood flow at the site
2. Distribution
- Movement of drug from bloodstream to body tissues and organs
- Affected by:
- Blood flow to tissues
- Protein binding - drug binds to plasma proteins (mainly albumin); only free (unbound) drug is active
- Blood-brain barrier - prevents many drugs from reaching the brain
- Lipid solubility - lipid-soluble drugs distribute widely
3. Metabolism (Biotransformation)
- The body chemically changes (inactivates or activates) drugs - mainly in the liver
- Prodrugs are inactive when given but become active after liver metabolism (e.g., codeine becomes morphine)
- Liver disease reduces drug metabolism - doses may need adjustment
4. Excretion (Elimination)
- Removal of drug from the body - mainly via kidneys (urine)
- Also through: bile/feces, lungs (exhaled), sweat, breast milk, saliva
- Kidney disease slows excretion - drug accumulates and can become toxic
- Half-life (t½) - time required for drug concentration in blood to decrease by 50%
- Short half-life = needs more frequent dosing
- Long half-life = can be dosed less frequently
B. Pharmacodynamics - "What the drug does to the body"
- Study of how drugs produce their effects
- Most drugs work by binding to specific receptors on cells
- Agonist - drug that binds to receptor and activates it (produces a response)
- Antagonist - drug that binds to receptor but blocks it (no response, prevents agonist from acting)
- Dose-response relationship - higher dose generally produces greater effect up to a maximum
- Therapeutic index (TI) - ratio of toxic dose to therapeutic dose; narrow TI drugs (e.g., digoxin, warfarin, lithium) require careful monitoring
TOPIC 3: FACTORS INFLUENCING MEDICATION ACTION
- Age - children and elderly metabolize drugs differently; dosing must be adjusted
- Body weight - heavier patients may need higher doses; pediatric doses calculated in mg/kg
- Gender - women have more body fat (affects fat-soluble drug distribution); hormonal differences
- Genetics - genetic variations affect drug metabolism (pharmacogenetics)
- Nutritional status - malnutrition reduces plasma proteins, affecting drug binding
- Disease states - liver/kidney disease impairs metabolism and excretion
- Psychological factors - anxiety, placebo effect, patient compliance
- Drug tolerance - body becomes less responsive to drug over time; higher dose needed for same effect
- Time of administration - some drugs work better when taken with/without food
- Route of administration - affects speed of onset and intensity
- Drug interactions - multiple drugs can increase or decrease each other's effects
- Environment - temperature, smoking, alcohol use affect drug action
TOPIC 4: MEDICATION ORDERS AND PRESCRIPTIONS
Parts of a Valid Prescription:
- Patient's full name, age, date of birth, address
- Date of prescription
- Drug name (generic or brand)
- Dose (amount per administration)
- Route of administration (oral, IV, IM, etc.)
- Frequency/Timing (once daily, BD, TDS, QID, PRN, etc.)
- Duration of treatment
- Prescriber's name, signature, registration number
Types of Medication Orders:
- Routine/Standing order - given at regular scheduled times until discontinued (e.g., Tab. Metformin 500 mg OD)
- PRN (Pro Re Nata) - given as needed, when patient requires it (e.g., Tab. Paracetamol PRN for pain)
- Single/One-time order - given only once at a specified time (e.g., pre-op medication)
- STAT order - given immediately, only once (emergencies)
- Verbal/Telephone order - doctor gives order verbally; nurse writes it down, reads back to confirm, and doctor must sign within 24 hours
- Standing protocols - pre-authorized orders for specific situations (e.g., hypoglycemia protocol)
TOPIC 5: SYSTEMS OF MEASUREMENT
Metric System (Most commonly used in healthcare):
- Weight: milligrams (mg), grams (g), kilograms (kg)
- 1 g = 1000 mg | 1 kg = 1000 g
- Volume: milliliters (mL), liters (L)
- 1 L = 1000 mL
- Length: millimeters (mm), centimeters (cm), meters (m)
Household System:
- Teaspoon (tsp) = 5 mL
- Tablespoon (tbsp) = 15 mL
- 1 cup = 240 mL
Apothecary System (Old, rarely used now):
- Grain (gr), dram, ounce
- 1 grain = 60 mg (approximately)
TOPIC 6: MEDICATION DOSE CALCULATION
Basic Formula:
Dose to give = (Desired dose ÷ Dose on hand) × Volume on hand
Example: Doctor orders 250 mg; on hand is 500 mg/5 mL
= (250 ÷ 500) × 5 = 2.5 mL
Pediatric Dose (mg/kg):
Dose = Weight (kg) × mg/kg ordered
IV Drip Rate:
Drip rate (drops/min) = (Volume to be infused × Drop factor) ÷ Time in minutes
Common drop factors: Macrodrip = 15 or 20 gtt/mL | Microdrip = 60 gtt/mL
Key Points:
- Always double-check calculations
- For high-risk drugs, two nurses should independently calculate and verify
- If in doubt, consult a pharmacist or senior nurse
- Never round up dangerous drug doses
TOPIC 7: 10 RIGHTS OF MEDICATION ADMINISTRATION
These are the principles every nurse must follow before giving any medication:
| # | Right | What to Check |
|---|---|---|
| 1 | Right Patient | Check name band, ask patient to state their name and DOB |
| 2 | Right Drug | Verify drug name (generic and brand); do not confuse look-alike/sound-alike drugs |
| 3 | Right Dose | Calculate and verify the correct amount |
| 4 | Right Route | Confirm the prescribed route (oral, IV, IM, etc.) |
| 5 | Right Time | Give at the correct scheduled time |
| 6 | Right Documentation | Record immediately after giving - never before |
| 7 | Right Reason | Know why the patient is receiving this drug |
| 8 | Right Response | Monitor and document the patient's response to the drug |
| 9 | Right to Refuse | Patient has the right to refuse; document and inform prescriber |
| 10 | Right Education | Educate the patient about their medication |
TOPIC 8: MEDICATION ERRORS
Definition:
- Any preventable event that may cause or lead to inappropriate medication use or patient harm
Types of Medication Errors:
- Prescribing error - wrong dose, wrong drug, illegible handwriting
- Transcription error - error when copying the order
- Dispensing error - pharmacy gives wrong drug/dose
- Administration error - nurse gives wrong drug, dose, route, or time
- Monitoring error - failure to monitor for side effects or toxicity
- Omission error - drug not given at scheduled time
Common Causes:
- Poor handwriting / verbal orders
- Look-alike / sound-alike drug names (e.g., Hydroxyzine vs. Hydralazine)
- Distraction and interruptions while preparing medications
- Calculation errors
- Poor communication between healthcare team
- High workload
- Missing or incomplete patient allergies recorded
Prevention of Medication Errors (Nurse's Role):
- Always follow the 10 Rights
- Never prepare medications in advance and leave them unattended
- Read drug labels 3 times: when taking from shelf, when preparing, before giving
- Clarify any unclear or illegible order with the prescriber
- Keep the medication area quiet and free of distractions
- Report ALL errors - even near-misses - for quality improvement
- Maintain up-to-date drug knowledge
TOPIC 9: ROUTES OF ADMINISTRATION
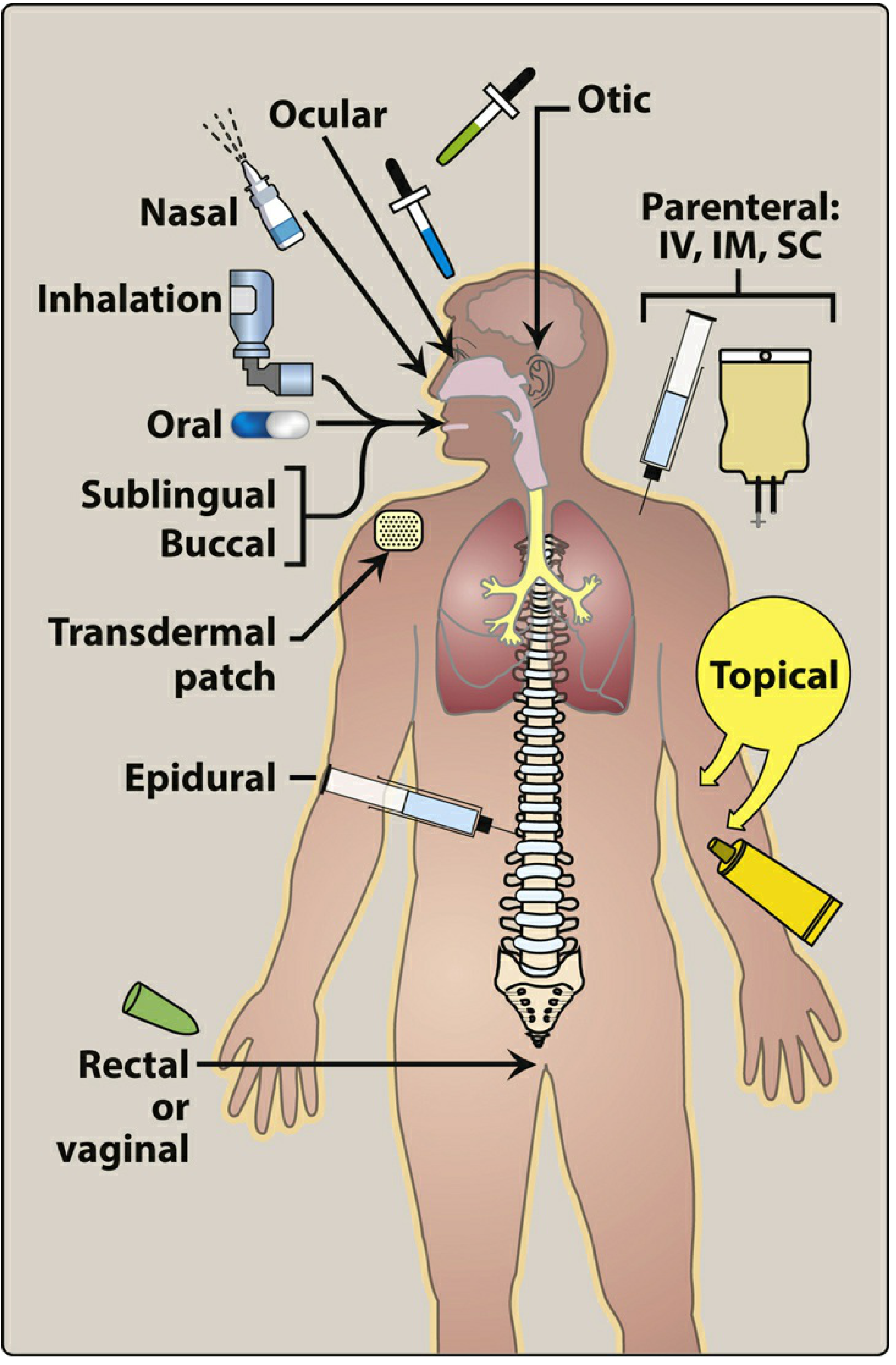
Overview of Routes:
1. ENTERAL ROUTES (via GI tract)
a) Oral (PO)
- Most common, convenient, safest, cheapest route
- Drug swallowed and absorbed from stomach/small intestine
- Disadvantages: slow onset; affected by food, gastric pH; first-pass metabolism; cannot use if vomiting/unconscious
- Available forms: tablets, capsules, liquids, suspensions
b) Sublingual (SL)
- Drug placed under the tongue
- Absorbed directly into blood vessels under tongue (bypasses first-pass metabolism)
- Fast onset (within minutes)
- Example: Glyceryl trinitrate (GTN) for angina
- Important: Patient must NOT swallow the tablet
c) Buccal
- Drug placed between cheek and gum
- Similar advantages to sublingual - fast absorption, bypasses liver
- Example: buccal midazolam for seizures
2. PARENTERAL ROUTES (bypass GI tract)
(Covered in detail in Topic 12)
3. TOPICAL ROUTES
(Covered in detail in Topic 13)
4. INHALATION ROUTE
(Covered in Topic 14)
TOPIC 10: STORAGE AND MAINTENANCE OF DRUGS - NURSE'S RESPONSIBILITY
General Drug Storage:
- Store at room temperature (15-25°C) unless specified otherwise
- Refrigerator (2-8°C): vaccines, insulin, suppositories, some eye drops
- Keep in original, labeled containers
- Protect from light, heat, moisture
- Never store drugs near disinfectants or cleaning agents
- Check expiry dates regularly and remove expired drugs
Controlled/Narcotic Drug Storage:
- Must be stored in a double-locked cupboard
- A separate narcotic register must be maintained
- Two nurses must sign for each controlled drug given
- Regular stock counts must be performed
Nurse's Responsibilities:
- Never leave the medicine trolley unlocked or unattended
- Ensure all drug labels are clear and not defaced
- Return unused drugs according to hospital policy
- Report any discrepancies in narcotic count immediately
- Check drug compatibility before mixing
- Discard partially used ampoules (single-dose vials)
- Report damaged, discolored, or contaminated medications
TOPIC 11: TERMINOLOGIES AND ABBREVIATIONS IN PRESCRIPTIONS
| Abbreviation | Latin Term | Meaning |
|---|---|---|
| OD / OD | Omni die | Once daily |
| BD / BID | Bis in die | Twice a day |
| TDS / TID | Ter die sumendum | Three times a day |
| QID | Quater in die | Four times a day |
| PRN | Pro re nata | As needed / when required |
| STAT | Statim | Immediately |
| AC | Ante cibum | Before meals |
| PC | Post cibum | After meals |
| HS | Hora somni | At bedtime |
| PO | Per os | By mouth (oral) |
| IV | - | Intravenous |
| IM | - | Intramuscular |
| SC / SQ | - | Subcutaneous |
| ID | - | Intradermal |
| SL | - | Sublingual |
| TOP | - | Topical |
| INH | - | Inhalation |
| tabs | Tabella | Tablet |
| caps | Capsula | Capsule |
| sol | Solutio | Solution |
| supp | Suppositorium | Suppository |
| gtt | Gutta | Drop(s) |
| mL | - | Milliliter |
| mg | - | Milligram |
TOPIC 12: DEVELOPMENTAL CONSIDERATIONS IN MEDICATION
Neonates and Infants:
- Immature liver and kidneys - slower drug metabolism and excretion
- Higher body water percentage - affects drug distribution
- Drug doses calculated by weight (mg/kg)
- Use appropriate liquid formulations
Children:
- Doses calculated by weight or body surface area
- Oral route preferred; use flavored preparations when possible
- Involve parents in medication teaching
Pregnant Women:
- Many drugs cross the placenta and can harm the fetus
- Nurse must always ask about pregnancy before administering medications
- Avoid teratogenic drugs (category D, X drugs)
- Breastfeeding mothers: some drugs pass into breast milk
Elderly Patients:
- Reduced liver/kidney function = slower metabolism and excretion = drug accumulation
- More sensitive to drug effects - start with lower doses ("start low, go slow")
- Multiple medications (polypharmacy) - high risk of drug interactions
- Visual/cognitive impairment may affect compliance
- Increased fall risk with sedatives, antihypertensives
TOPIC 13: ORAL, SUBLINGUAL, AND BUCCAL ROUTES
Oral Medication Administration - Procedure:
- Perform hand hygiene
- Check the medication order (5+Rights minimum)
- Gather equipment: medication, medicine cup, water, medication record
- Prepare the medication - read label 3 times
- Identify the patient (ask name + check wristband)
- Explain the procedure to the patient
- Assist patient to upright or semi-Fowler's position (prevents aspiration)
- Give the medication with sufficient water (at least 60-90 mL) to aid swallowing
- Stay with the patient until all medications are swallowed
- Document immediately in the medication record
- Monitor for therapeutic effect and side effects
Sublingual Medication Procedure:
- Place tablet under the tongue
- Patient must not chew, swallow, or eat/drink until tablet dissolves (about 5 minutes)
- Monitor for relief of symptoms (e.g., chest pain relief with GTN)
Buccal Medication Procedure:
- Place tablet/film between cheek and upper gum
- Patient must not chew or swallow
- Alternate sides with each dose to prevent mucous membrane irritation
TOPIC 14: PARENTERAL ADMINISTRATION OF DRUGS
Definition:
- Parenteral = administering drug by any route OTHER than the GI tract (comes from Greek: para = beside, enteron = intestine)
- Drug goes directly into tissues or bloodstream
Advantages of Parenteral Route:
- Fast onset of action
- Can be used when oral route is not possible (unconscious, vomiting, NPO)
- Allows precise dosing
- Useful for drugs destroyed by GI tract
Disadvantages:
- Invasive - causes pain and anxiety
- Risk of infection, embolism, hematoma
- Cannot be reversed once given
- Requires sterile technique and trained personnel
- More expensive
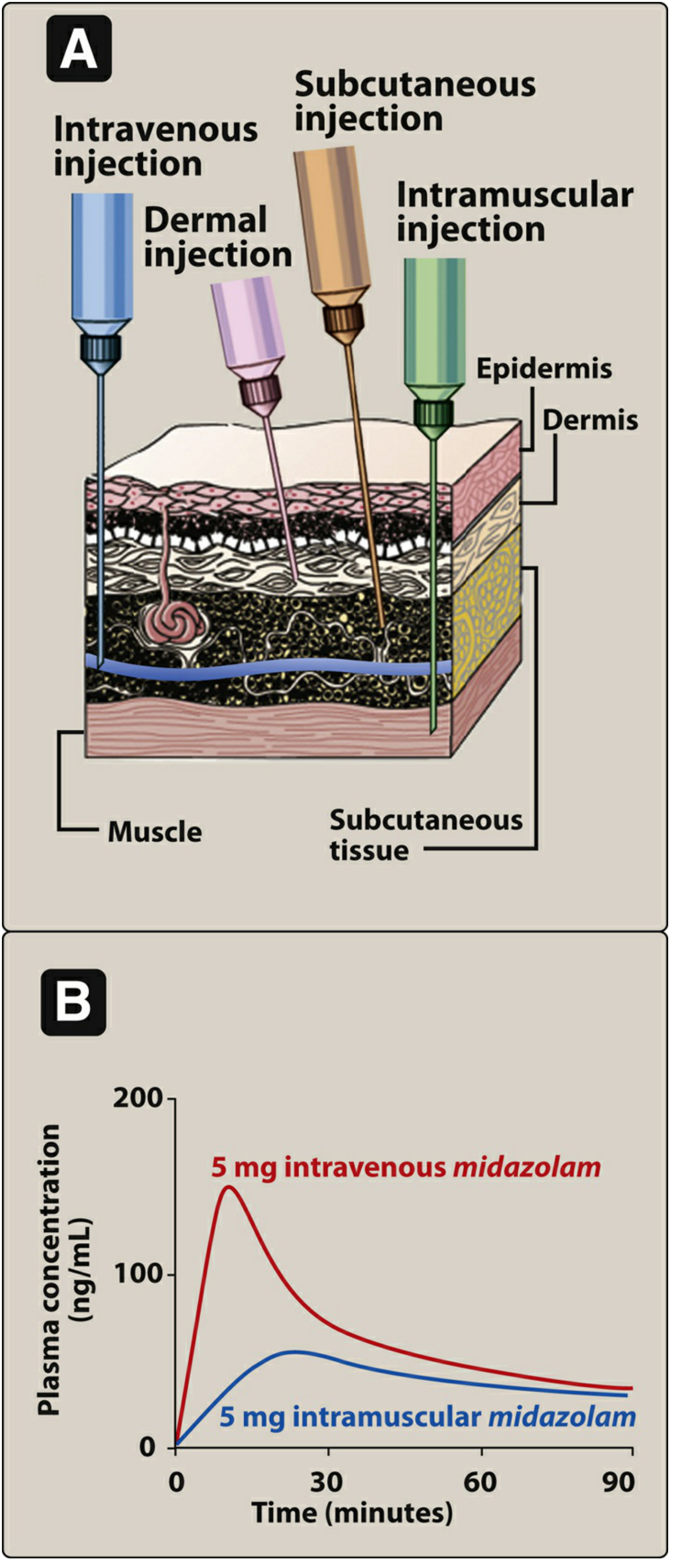
A. Intradermal (ID) Injection
What it is:
- Drug injected into the dermis (just below the surface of the skin)
- Needle angle: 5-15 degrees (almost flat against skin)
- Volume: 0.01 - 0.1 mL only
- Needle: Short, fine gauge (26-27G)
Sites:
- Inner (volar) forearm - most common
- Upper chest
- Upper back (scapular area)
Uses:
- Tuberculin (Mantoux) test for TB
- Allergy testing
- Local anesthetic before IV insertion
Technique:
- Insert bevel up
- A bleb (wheal) should form upon injection
- Do NOT massage the site after injection
- Mark the site with a pen for TB test reading (read after 48-72 hours)
B. Subcutaneous (SC / SQ) Injection
What it is:
- Drug injected into the subcutaneous tissue (fatty layer below the dermis)
- Needle angle: 45-90 degrees (90° if patient is obese; 45° if thin)
- Volume: 0.5-1 mL (maximum 2 mL)
Sites:
- Abdomen (2 inches away from the umbilicus) - best absorption
- Outer upper arm
- Anterior thigh
- Upper back
Uses:
- Insulin injections
- Heparin (anticoagulant)
- Vaccines (e.g., MMR, varicella)
Important nursing points:
- Rotate injection sites to prevent lipodystrophy (fatty lumps/depressions)
- Do NOT aspirate for insulin or heparin
- Do NOT massage heparin injection site (causes bruising)
- Insulin absorption is fastest from abdomen
C. Intramuscular (IM) Injection
What it is:
- Drug injected into a muscle
- Needle angle: 90 degrees
- Muscles have rich blood supply = faster absorption than SC
- Volume: up to 3-5 mL in large muscles (max 2-3 mL in deltoid)
Sites and Key Points:
| Site | Location | Max Volume | Landmarks |
|---|---|---|---|
| Vastus lateralis (outer thigh) | Middle 1/3 of the outer thigh | 5 mL | Preferred in infants and young children |
| Deltoid (upper arm) | 2-3 finger widths below the acromion process | 2-3 mL | Easy access; smaller muscle |
| Ventrogluteal | Outer hip region (gluteus medius) | 5 mL | Safest IM site - away from major nerves and vessels; preferred in adults |
| Dorsogluteal | Buttock (upper outer quadrant) | 5 mL | Risk of sciatic nerve injury - AVOID in infants |
Uses:
- Vaccines (e.g., Hepatitis B, DPT)
- Antibiotics (e.g., penicillin, gentamicin)
- Analgesics (e.g., morphine)
- Hormonal injections (e.g., Depo-Provera)
Z-track technique:
- Pull skin 2-3 cm to the side before injecting
- Inject drug, wait 10 seconds, release skin
- Prevents drug from leaking back up into subcutaneous tissue
- Used for irritating drugs (e.g., iron dextran, hydroxyzine)
D. Intravenous (IV) Injection / Infusion
What it is:
- Drug injected directly into a vein
- Fastest route - immediate effect
- 100% bioavailability
Types of IV Administration:
- IV bolus (push) - rapid injection of small volume directly into vein
- IV infusion (drip) - large volume given over time via infusion set
Sites:
- Antecubital fossa (inside elbow)
- Forearm veins (cephalic, basilic, median cubital)
- Back of the hand
- For infants: scalp veins, dorsal foot veins
Indications:
- Emergency situations (shock, cardiac arrest)
- When large volumes of fluid are needed
- When drugs are too irritating for other routes
- For unconscious or NPO patients
Nursing Points:
- Use sterile technique at all times
- Check IV site for infiltration (swelling, pain - drug entering surrounding tissue) and phlebitis (redness, warmth, pain along vein)
- Flush IV line before and after drug administration
- Never mix incompatible drugs in the same line
- Monitor flow rate and site every 1-2 hours
TOPIC 15: EQUIPMENT - SYRINGES, NEEDLES, CANNULAS, INFUSION SETS
Syringes:
- Parts: Tip (where needle attaches), Barrel (graduated cylinder), Plunger
- Types by tip:
- Luer-lock tip: needle screws and locks on (safer, won't pop off)
- Slip tip: needle just pushes on (quick attachment)
- Sizes: 1 mL (insulin/ID), 3 mL, 5 mL, 10 mL, 20 mL, 50 mL
- Insulin syringe: calibrated in units not mL; always use insulin syringe for insulin
Needles:
- Parts: Hub, Shaft, Bevel (slanted tip)
- Gauge (G): Higher gauge = thinner needle
- ID: 26-27G | SC: 25-27G | IM: 21-23G | IV: 18-21G
- Length: ID: 1 cm | SC: 1.5-2.5 cm | IM: 2.5-3.8 cm
IV Cannula (Peripheral IV Catheter):
- A short flexible plastic tube inserted into a vein
- Color-coded by size:
- Pink (20G), Blue (22G), Green (18G), Grey (16G), Orange (14G - for rapid transfusion)
- Smaller gauge = larger bore = faster flow rate
Infusion Sets:
- Parts: Spike, Drip chamber, Roller clamp, Tubing, Injection port, Needle adapter
- Macrodrip set: 15 or 20 drops/mL - for standard IV fluids
- Microdrip set: 60 drops/mL - for precise rate control (pediatrics, critical drugs)
- Burette/Soluset: for pediatric IV infusions (measured small volumes)
- Blood/transfusion set: has a special filter (170-260 micron); 15 drops/mL
TOPIC 16: VIALS AND AMPOULES
Ampoules:
- Small glass containers with a narrow neck
- Single-dose only - must be discarded after opening
- Opening technique:
- Score the neck, wrap with gauze
- Break neck away from you (or use an ampoule opener)
- Draw up with a filter needle (to remove glass particles)
- Change to appropriate needle before injection
Vials:
- Rubber-stoppered glass or plastic containers
- Can be single-dose or multi-dose
- Some contain powder that must be reconstituted (dissolved in sterile water or saline)
- Drawing up technique:
- Clean rubber stopper with alcohol swab and let dry
- Inject air equal to volume of drug to be withdrawn (creates positive pressure)
- Invert vial and draw up required amount
- Check for air bubbles and expel
Preparing Injectable Medicines:
From ampoule:
- Check drug, dose, expiry
- Score and snap open ampoule
- Insert filter needle; draw up drug
- Replace with injection needle
- Expel air, check dose
From powder vial:
- Add the correct diluent (as specified - usually sterile water or normal saline)
- Gently swirl until completely dissolved (do NOT shake vigorously unless specified)
- Draw up required volume
- Label the vial with date, time, concentration if multi-dose
TOPIC 17: CARE OF EQUIPMENT - DECONTAMINATION AND DISPOSAL
Decontamination of Reusable Equipment:
- Cleaning: removal of visible dirt/organic matter (first step always)
- Disinfection: kills most (not all) microorganisms
- Sterilization: kills ALL microorganisms including spores (autoclaving, ETO gas, gamma radiation)
Disposal of Sharps (Syringes, Needles):
- Never recap a needle with both hands - use one-hand scoop technique if recapping is necessary
- Immediately discard needles into a puncture-proof sharps container (yellow bin)
- Never bend, break, or cut needles
- Sharps container should be sealed when 3/4 full (not completely full)
- Dispose according to biomedical waste management rules
Prevention of Needle-Stick Injuries (NSI):
- Most important prevention: Never recap with two hands
- Use safety-engineered needles (retractable, self-sheathing)
- Keep sharps containers within reach of work area
- Do not pass sharps hand-to-hand
- Wear gloves during all invasive procedures
- Never overload sharps containers
If Needle-Stick Injury Occurs:
- Immediately wash the wound with soap and water
- Allow it to bleed freely (do not squeeze or suck)
- Apply antiseptic
- Report to nurse in-charge/occupational health immediately
- Identify the source patient (HIV, Hepatitis B, C status)
- Start post-exposure prophylaxis (PEP) for HIV within 72 hours (ideally within 2 hours)
- Document the incident
- Follow up blood tests for the exposed healthcare worker
TOPIC 18: TOPICAL ADMINISTRATION
Definition: Application of drug directly to a body surface (skin or mucous membrane) for local or systemic effect
A. Application to Skin and Mucous Membrane:
- Ointments: Thick, greasy; apply thin layer with gloves; covers and protects skin
- Creams: Water-based, lighter; for moisturizing or anti-infective use
- Gels: Clear, water-based; quick-absorbing
- Lotions: Liquid preparation; apply by patting or dabbing
- Transdermal patches: Drug slowly absorbed through skin for systemic effect (e.g., nicotine patch, fentanyl patch, GTN patch)
- Rotate sites to prevent skin irritation
- Remove old patch before applying new one
B. Direct Application - Gargle and Throat Swabbing:
- Gargling: Patient gargles medicated solution (e.g., antiseptic, chlorhexidine) for throat infections
- Throat swabbing: Apply medicated preparation directly to throat mucosa using an applicator
C. Insertion into Body Cavities:
Rectal suppositories:
- Lubricate suppository and insert with gloved finger past internal anal sphincter (approx. 4 cm)
- Patient lies in left lateral (Sims) position
- Patient should retain for 15-30 minutes for full effect
- Useful when patient is vomiting, NPO, or unconscious
Vaginal suppositories/pessaries:
- Inserted into vaginal canal with applicator or gloved finger
- Patient should remain lying for 15-30 minutes after insertion
- Used for vaginal infections (antifungals, antibiotics)
D. Instillations:
Application of liquid drug drop by drop into body cavities:
Eye drops/ointment:
- Wash hands; have patient tilt head back
- Pull lower eyelid down to form a conjunctival sac
- Instill drops into the inner canthus (sac) - do NOT touch the eye with dropper
- Patient should close eye gently and apply light pressure over inner canthus (nasolacrimal duct) for 1-2 minutes (prevents systemic absorption)
- Wait 5 minutes between different eye drops
- Apply ointment: ribbon from inner to outer canthus
Ear drops (otic):
- Warm drops to body temperature (hold in hands for 1-2 minutes) to prevent dizziness
- Adults: Pull pinna up and back to straighten canal
- Children under 3: Pull pinna down and back
- Instill drops into the ear canal wall (not directly at eardrum)
- Have patient remain with treated ear up for 5-10 minutes; place cotton loosely
Nasal drops/spray:
- Have patient blow nose gently first
- Head tilted back (hyperextended) for nasal drops
- Instill drops; patient breathes through mouth
- Remain in position 5 minutes
Bladder instillation:
- Drug instilled into bladder via catheter
- Used for bladder infections, bladder cancer treatment
- Clamp catheter per protocol duration; then drain
E. Irrigations:
Washing/flushing a body cavity with a medicated or cleansing solution:
- Eye irrigation: Used to flush out chemicals or foreign bodies
- Ear irrigation: Used to remove cerumen (earwax) or foreign bodies - use warm water
- Bladder irrigation: Continuous or intermittent - to prevent/remove clots after surgery
- Vaginal irrigation (douche): Rare; only on medical order
- Rectal irrigation (enema): To empty bowel or deliver medication
F. Spraying:
- Nasal spray: For nasal decongestants, corticosteroids (e.g., fluticasone for allergic rhinitis)
- Throat spray: For local anaesthesia or antiseptic to throat
TOPIC 19: INHALATION ROUTE
Definition: Administration of drug in gaseous or aerosol form through the respiratory tract
Types:
- Nasal inhalation - drug inhaled through nose
- Oral inhalation - drug inhaled through mouth (most common)
- Endotracheal/Tracheal - in intubated patients (via ET tube)
Equipment:
Metered-Dose Inhaler (MDI):
- Most common; delivers measured amount of drug with each puff
- Requires coordination between pressing and inhaling
- Use a spacer device to improve drug delivery (especially for children and elderly)
Dry Powder Inhaler (DPI):
- Drug in powder form; activated by patient's inhalation
- No propellant needed
Nebulizer:
- Converts liquid drug into fine mist for inhalation
- Used for severe asthma, COPD, or when patient cannot use MDI
- Can deliver larger doses over a longer period
Steam inhalation:
- Hot steam loosens secretions in respiratory tract
- Used for colds, sinusitis, laryngitis
Oxygen therapy:
- Delivered via nasal prongs, face mask, Venturi mask, non-rebreather mask
- Maintains oxygen saturation (SpO2)
Purposes of Inhalation:
- Deliver bronchodilators (e.g., salbutamol for asthma)
- Deliver corticosteroids (e.g., budesonide for asthma control)
- Humidify airways
- Administer oxygen
- Loosen and clear secretions
MDI Procedure:
- Shake inhaler well
- Attach spacer if available
- Exhale completely
- Place mouthpiece in mouth (or just outside if no spacer)
- Start inhaling slowly; press canister once
- Inhale deeply and slowly
- Hold breath for 10 seconds
- Exhale slowly through nose
- Wait 1 minute between puffs
- Rinse mouth after steroid inhalers (to prevent oral candidiasis)
Recording and Reporting:
- Document drug name, dose, route, time, and patient's response
- Report any adverse effects (bronchospasm, palpitations, etc.)
TOPIC 20: OTHER PARENTERAL ROUTES
| Route | Meaning | Use |
|---|---|---|
| Epidural | Injection into the epidural space (between vertebral column and spinal dura mater) | Pain management (labor, post-op); e.g., epidural morphine |
| Intrathecal (spinal) | Injection into the subarachnoid space (where CSF is) | Spinal anesthesia; chemotherapy for CNS cancers; antibiotics for meningitis |
| Intraosseous (IO) | Injection into the bone marrow cavity | Emergency when IV access is impossible (cardiac arrest in children); very rapid absorption |
| Intraperitoneal (IP) | Injection into the peritoneal cavity | Chemotherapy for abdominal cancers (e.g., ovarian cancer); peritoneal dialysis |
| Intrapleural | Injection into the pleural space (between lung and chest wall) | Sclerotherapy for recurrent pleural effusion; local anesthetics |
| Intra-arterial | Injection directly into an artery | Chemotherapy directly to tumor (e.g., hepatic artery chemotherapy); thrombolytic therapy; diagnostic contrast injections |
QUICK REFERENCE SUMMARY TABLE: INJECTION COMPARISON
| Feature | Intradermal | Subcutaneous | Intramuscular | Intravenous |
|---|---|---|---|---|
| Tissue | Dermis | Fatty tissue | Muscle | Vein |
| Needle angle | 5-15° | 45-90° | 90° | 15-30° |
| Volume | 0.01-0.1 mL | 0.5-2 mL | Up to 5 mL | Variable |
| Needle gauge | 26-27G | 25-27G | 21-23G | 18-21G |
| Onset | Slowest | Slow | Medium-fast | Fastest (immediate) |
| Absorption | Very slow | Slow | Fast | Immediate (100%) |
| Key use | TB test, allergy testing | Insulin, heparin | Vaccines, antibiotics | Emergency, large volumes |
Source: Lippincott Illustrated Reviews: Pharmacology, 7th Edition | Goodman & Gilman's The Pharmacological Basis of Therapeutics, 14th Edition | Katzung's Basic and Clinical Pharmacology, 16th Edition
These notes cover every topic listed in your syllabus. Here are study tips:
- Learn the 10 Rights by heart - examiners love them
- Practice dose calculations using the formula daily
- Remember the Z-track technique for IM injections
- Never forget NSI protocol (wash + report + PEP within 72 hours)
- Memorize the ADME framework for pharmacokinetics
This is a shared conversation. Sign in to Orris to start your own chat.