Topic : pulmonary function test
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary function tests" AND "spirometry"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
I now have all the content needed for a comprehensive response. Let me compile the full answer.
Pulmonary Function Tests (PFTs)
Pulmonary function tests are a battery of tests that assess the mechanical and gas-exchange properties of the lungs. They are the cornerstone of diagnosing, classifying, and monitoring respiratory disease.
1. Lung Volumes - The Foundation
Before understanding PFTs, it helps to visualize the lung volume compartments:
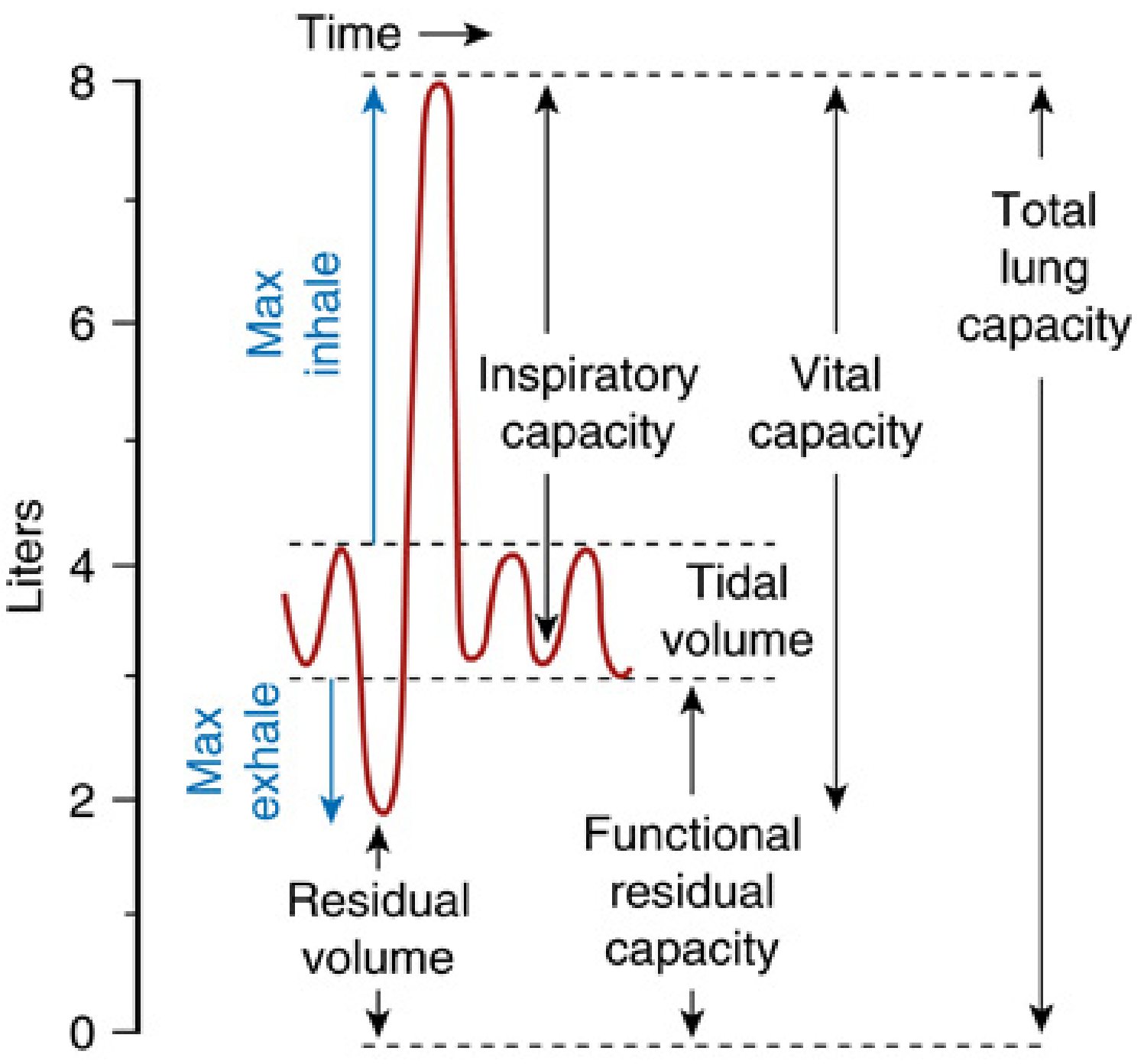
| Volume / Capacity | Definition | Typical Value (adult male) |
|---|---|---|
| Tidal Volume (TV) | Air moved in/out with each normal breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra air inhaled above TV | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra air exhaled below TV | ~1200 mL |
| Residual Volume (RV) | Air remaining after maximal exhalation | ~1200 mL |
| Functional Residual Capacity (FRC) | ERV + RV (volume at end of quiet expiration) | ~2400 mL |
| Vital Capacity (VC) | Maximum air exhaled after maximum inhalation | ~4800 mL |
| Total Lung Capacity (TLC) | All volumes combined | ~6000 mL |
RV and FRC cannot be measured by spirometry alone - they require helium dilution, nitrogen washout, or body plethysmography.
2. Spirometry - The Primary PFT
Spirometry measures the volume and flow of air during forced breathing maneuvers.
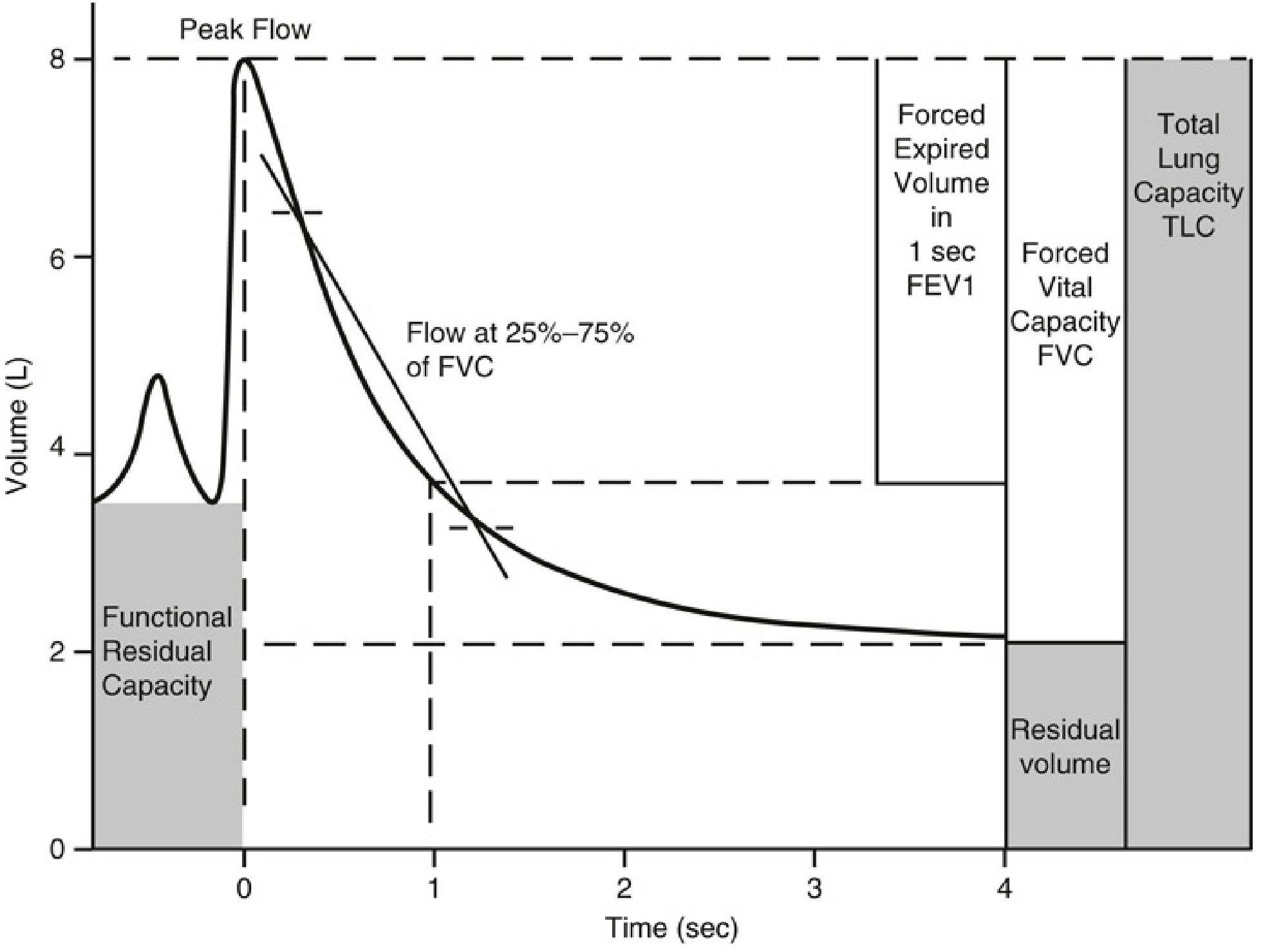
Key Spirometric Parameters
| Parameter | Description |
|---|---|
| FVC (Forced Vital Capacity) | Total air forcefully exhaled from TLC to RV |
| FEV1 (Forced Expiratory Volume in 1 sec) | Volume exhaled in the first second of the FVC maneuver |
| FEV1/FVC ratio | The most important ratio; normally >0.70 (or ≥ lower limit of normal, LLN) |
| FEF 25-75% | Mean forced expiratory flow in the middle half of FVC; reflects small airway function |
| PEFR (Peak Expiratory Flow Rate) | Maximum flow rate achieved during forced exhalation |
| MVV (Maximum Voluntary Ventilation) | Maximum air breathed in 12 seconds; reflects overall respiratory muscle strength |
ATS/ERS recommendation: Use the FEV1/VC ratio vs. LLN (5th percentile for age/sex/height/ethnicity) rather than a fixed cutoff of 0.70. Using 70% as a fixed cutoff misdiagnoses obstruction in men >40 and women >50, and over-diagnoses COPD in elderly asymptomatic non-smokers.
- Fishman's Pulmonary Diseases and Disorders, p. 603
3. The ATS/ERS Interpretation Algorithm
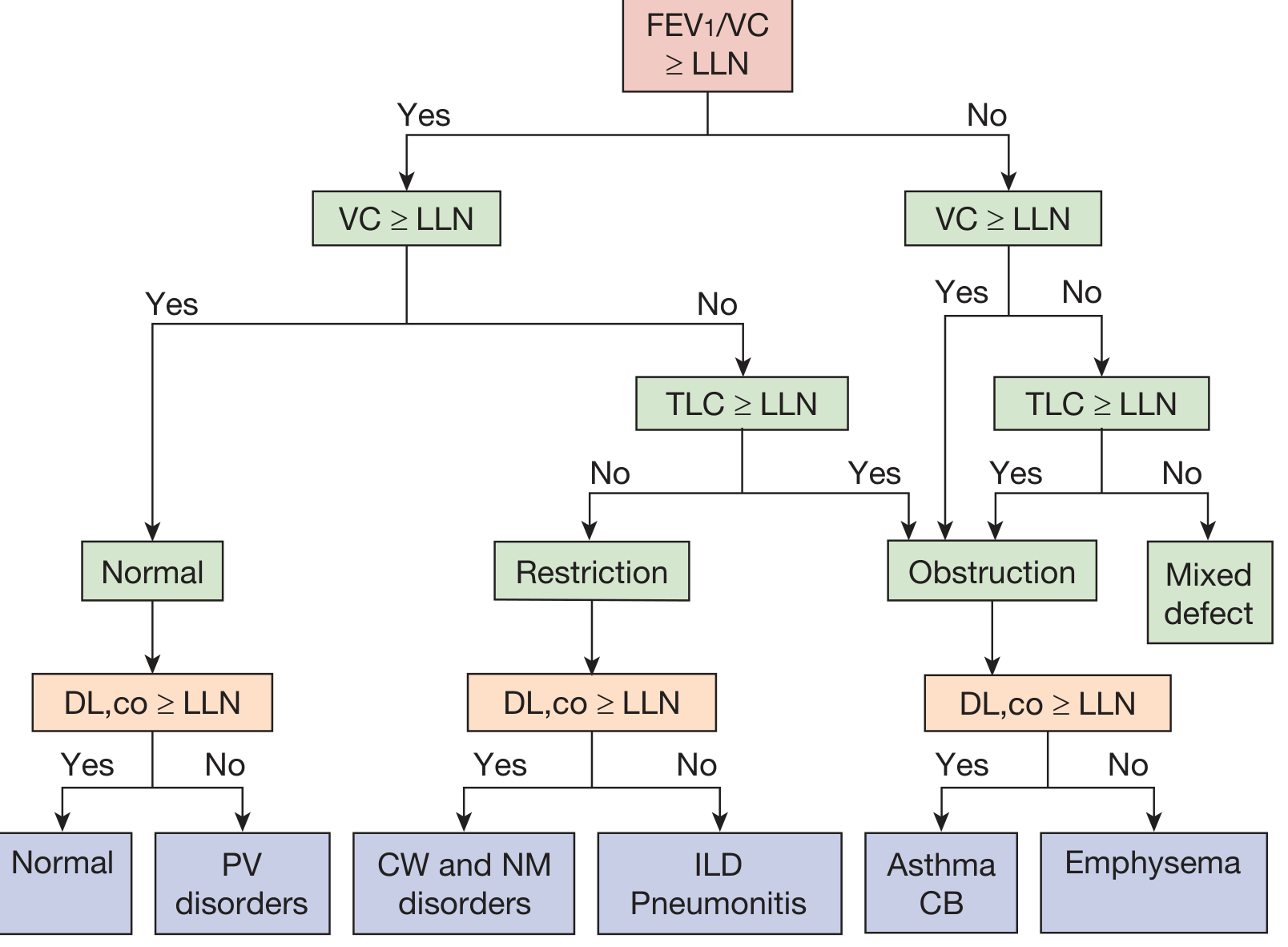
The recommended interpretation sequence:
-
Check FEV1/VC ratio vs. LLN
- If ≥ LLN → normal ratio (go to VC)
- If < LLN → obstructive physiology (go to VC)
-
Check VC vs. LLN
- Normal ratio + normal VC → Normal (then check DLCO)
- Normal ratio + low VC → check TLC: if TLC < LLN → Restriction
- Low ratio + normal VC + normal TLC → Obstruction (then check DLCO)
- Low ratio + low VC + low TLC → Mixed defect
-
Check DLCO
- Normal PFTs + low DLCO → Pulmonary vascular (PV) disorder (e.g., pulmonary embolism, pulmonary hypertension)
- Obstruction + normal DLCO → Asthma or chronic bronchitis
- Obstruction + low DLCO → Emphysema
- Restriction + normal DLCO → Chest wall (CW) or neuromuscular (NM) disorder
- Restriction + low DLCO → ILD or pneumonitis
- Fishman's Pulmonary Diseases and Disorders, p. 602-603
4. The Three Basic PFT Patterns
Obstructive Pattern
- Hallmark: Reduced FEV1/VC%
- Lung volumes: RV, FRC, and TLC typically all increased (air trapping)
- DLCO: Normal in asthma/chronic bronchitis; reduced in emphysema
Causes:
| Disease | Location | Mechanism |
|---|---|---|
| Chronic bronchitis | Large + small airways | Fibrosis, secretions, edema |
| Emphysema | Lung parenchyma | Loss of elastic recoil |
| Asthma | Large + small airways | Smooth muscle contraction, edema |
| Cystic fibrosis | Large + small airways | Fibrosis, retained secretions |
| Small-airway disease | Small airways (<2 mm) | Narrowing/stenosis |
| Upper-airway obstruction | Trachea/main bronchi | Anatomic/functional narrowing |
Bronchodilator response: A positive bronchodilator response is defined as an increase in FEV1 (or FVC) of ≥12% AND ≥200 mL after inhaled bronchodilator - supports asthma over COPD (though COPD can also show partial reversibility).
Methacholine challenge: A 20% fall in FEV1 (PC20) confirms airway hyperreactivity/asthma when spirometry is normal.
Restrictive Pattern
- Hallmark: Reduced TLC (definitive criterion); normal or elevated FEV1/VC%; reduced VC
- Subdivided by cause:
| Type | RV | FRC | DLCO |
|---|---|---|---|
| Parenchymal (ILD, fibrosis) | ↓ | ↓ | ↓ |
| Pleura/chest wall (effusion, kyphoscoliosis, obesity) | N | ↓ | N or ↓ |
| Neuromuscular (MG, ALS, phrenic nerve palsy) | ↑ (loss of expiratory force) | N | N |
Note: TLC reduction is the gold standard for restriction - a low VC alone is not sufficient, as obstruction can also reduce FVC.
- Fishman's Pulmonary Diseases and Disorders, p. 605-606
Mixed Obstructive-Restrictive Pattern
- Low FEV1/VC% (obstruction) plus reduced TLC (restriction)
- Seen in conditions like sarcoidosis, combined emphysema + pulmonary fibrosis, or advanced COPD with superimposed pleural disease.
- Fishman's Pulmonary Diseases and Disorders, p. 607
5. Summary Table - PFT Patterns
| Pattern | FEV1/FVC | FVC/VC | TLC | RV | DLCO |
|---|---|---|---|---|---|
| Normal | N | N | N | N | N |
| Obstructive (asthma/CB) | ↓ | N or ↓ | N or ↑ | ↑ | N |
| Obstructive (emphysema) | ↓ | ↓ | ↑ | ↑↑ | ↓ |
| Restrictive (ILD) | N or ↑ | ↓ | ↓ | ↓ | ↓ |
| Restrictive (CW/NM) | N | ↓ | ↓ | N or ↑ | N |
| Pulmonary vascular | N | N | N | N | ↓ |
| Mixed | ↓ | ↓ | ↓ | Variable | Variable |
- Symptom to Diagnosis: An Evidence-Based Guide, Table 15-8
6. Diffusing Capacity for CO (DLCO)
DLCO measures the functional capillary surface area available for gas exchange. Because CO has very high affinity for hemoglobin, its transfer is limited only by membrane thickness - not pulmonary blood flow. This makes DLCO a pure measure of the alveolar-capillary membrane.
Severity classification of DLCO reduction:
| Severity | DLCO (% predicted) |
|---|---|
| Mild | >60% but < LLN |
| Moderate | 40-60% |
| Severe | <40% |
DLCO < 60% predicted is associated with increased risk of postoperative pulmonary complications and is an indication for further preoperative risk assessment using exercise testing.
Causes of reduced DLCO: emphysema, ILD, pulmonary hypertension, pulmonary embolism, anemia (less hemoglobin to bind CO), pneumonectomy.
Causes of elevated DLCO: polycythemia, left-to-right shunt, mild/early asthma, pulmonary hemorrhage (alveolar blood binds CO).
- Miller's Anesthesia, 10e, p. 1304-1305
7. Flow-Volume Loops
The flow-volume loop plots airflow (y-axis) against volume (x-axis) and is particularly useful for diagnosing upper airway obstruction.
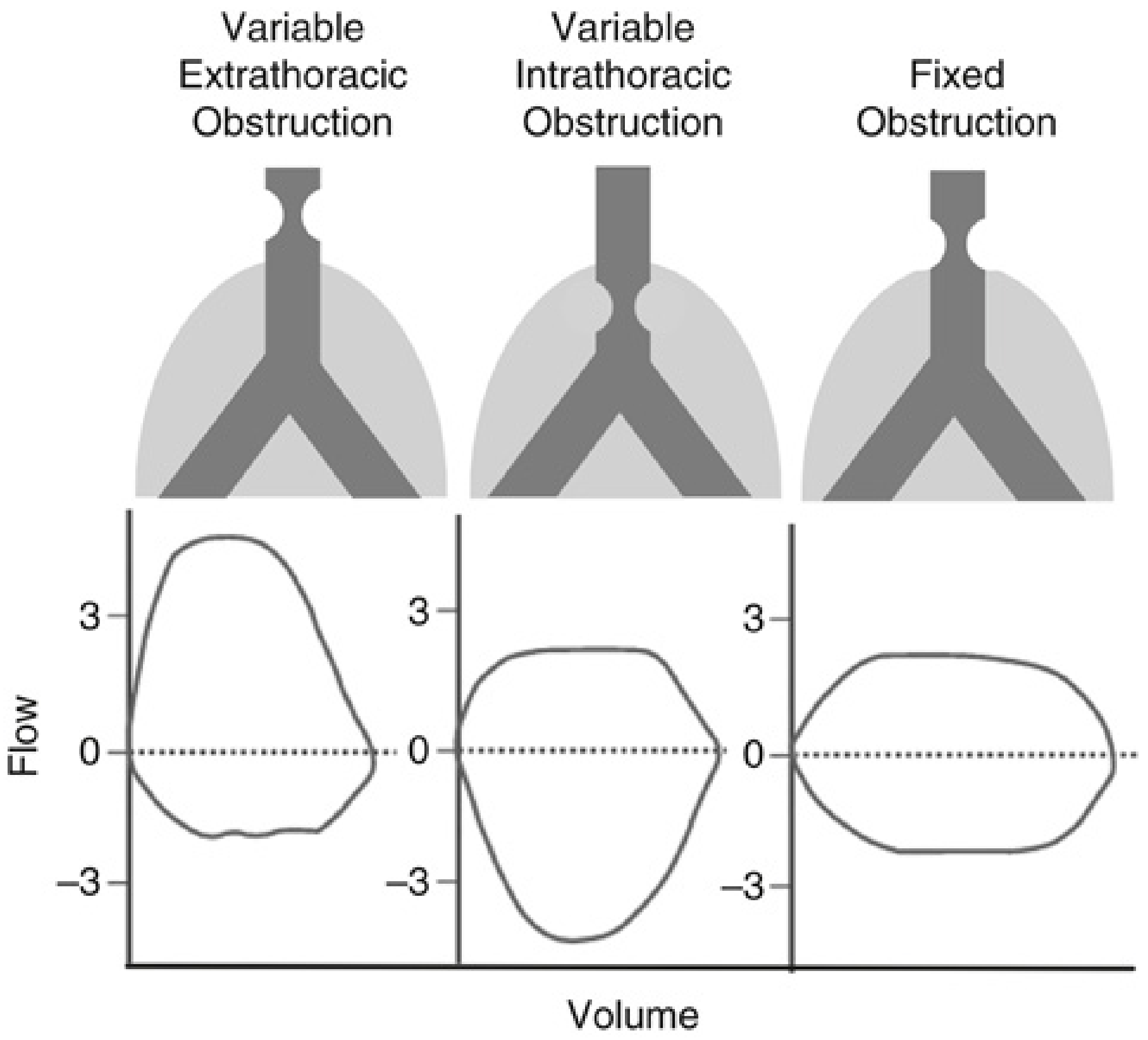
| Pattern | Inspiratory Loop | Expiratory Loop | Cause |
|---|---|---|---|
| Variable extrathoracic | Flattened (truncated) | Normal | Vocal cord dysfunction, tracheomalacia above thorax |
| Variable intrathoracic | Normal | Flattened | Tracheomalacia below thorax, endobronchial tumor |
| Fixed obstruction | Flattened | Flattened (equal both ways) | Fixed tracheal stenosis, bilateral vocal cord paralysis, tracheal ring |
Logic: Extrathoracic lesions worsen on inspiration (negative pressure sucks airway walls in). Intrathoracic lesions worsen on expiration (positive pleural pressure compresses them). Fixed lesions affect both phases equally.
- Miller's Anesthesia, 10e, p. 1305
8. Bronchodilator Reversibility Testing
After baseline spirometry, a short-acting bronchodilator (typically 400 mcg salbutamol) is administered, and spirometry is repeated after 15-20 minutes.
- Positive response: ≥12% AND ≥200 mL increase in FEV1 or FVC
- Strongly supports asthma
- Partial or absent reversibility does not exclude asthma (can vary day to day)
- COPD may show partial reversibility but rarely meets the full criteria
9. Special Tests
| Test | What It Measures | Clinical Use |
|---|---|---|
| Body plethysmography | TLC, FRC, RV (gold standard) | Definitive diagnosis of restriction or air trapping |
| Helium dilution / N2 washout | FRC, TLC, RV (by gas dilution) | Alternative to plethysmography; underestimates in severe emphysema |
| Airway resistance (Raw) / SGaw | Airway resistance/conductance | Useful when patient cannot perform forced maneuver |
| Methacholine challenge | PC20 (provocative concentration causing 20% FEV1 drop) | Confirms airway hyperreactivity in suspected asthma |
| Exercise testing (CPET) | VO2max, anaerobic threshold | Preoperative risk, dyspnea evaluation; VO2max <15 mL/kg/min = high surgical risk |
| Maximum inspiratory/expiratory pressures (MIP/MEP) | Respiratory muscle strength | Neuromuscular disease, weaning from ventilation |
10. Quick Clinical Applications
| Clinical Scenario | PFT Finding | Likely Diagnosis |
|---|---|---|
| FEV1/FVC < LLN, bronchodilator positive ≥12%+200 mL | Reversible obstruction | Asthma |
| FEV1/FVC < LLN, irreversible, DLCO ↓ | Fixed obstruction + impaired gas transfer | Emphysema/COPD |
| TLC ↓, FEV1% N/↑, DLCO ↓ | Restriction with impaired transfer | ILD (fibrosis, sarcoidosis) |
| Normal spirometry, isolated DLCO ↓ | Pure gas transfer defect | Pulmonary HTN, early emphysema, PE |
| Reduced VC + RV ↑ + MVV ↓ + NIF ↓ | Restriction with preserved RV | Neuromuscular disease |
| Truncated inspiratory loop | Variable extrathoracic obstruction | Vocal cord dysfunction |
Sources:
- Fishman's Pulmonary Diseases and Disorders, 2-Volume Set (Chapters 31), pp. 602-607
- Miller's Anesthesia, 10e, pp. 1303-1307
- Symptom to Diagnosis: An Evidence-Based Guide, 4e, Table 15-8
This is a shared conversation. Sign in to Orris to start your own chat.