I now have comprehensive content from authoritative sources. Let me compile the full answer.
Physiology of Labor, Partogram & Postpartum Period
PART A — PHYSIOLOGY OF LABOR
1. Definition & Onset of Labor
Labor is defined as sufficient uterine contractions in frequency, intensity, and duration to produce cervical effacement and dilation. It commences on average at 40 ± 2 weeks from the last menstrual period. — Morgan & Mikhail's Clinical Anesthesiology
Prodromal events (2–4 weeks before true labor):
- Lightening — presenting part settles into the pelvis; fundal height drops
- Braxton Hicks contractions — irregular, variable frequency and intensity
- Cervical effacement and softening
- Bloody show — cervical mucous plug (often blood-tinged) is expelled 1 week to 1 hour before true labor in most women; most women go into labor within 3 days of bloody show
False labor vs. true labor:
- False labor: irregular, short contractions that may actually assist cervical effacement
- True labor begins when Braxton Hicks contractions become coordinated, increasing to 25–60 mm Hg intensity and 15–20 minutes apart initially — Morgan & Mikhail
2. Initiation of Labor — Mechanisms
The exact trigger remains incompletely understood. Key factors:
- Uterine distension — stimulates myometrial sensitivity
- ↑ Myometrial oxytocin receptors — circulating oxytocin levels do not necessarily rise, but receptor density rapidly increases
- Prostaglandins (especially PGE₂ and PGF₂α) — synthesized by fetal membranes and decidua; central mediators of uterine contractility
- Progesterone withdrawal (functional) — progesterone maintains uterine quiescence; its declining influence at term removes inhibition
- Oestrogen rise — increases gap junctions between myometrial cells, promoting coordination of contractions
3. Uterine Contractions — Characteristics
- Active labor: contractions every 2–3 minutes, lasting ~1 minute, intensity ~40 mm Hg
- Adequate relaxation between contractions is critical — allows oxygenated blood into intervillous spaces and fetal compartment
- Frequent contractions 1–2 min apart may indicate abruptio placentae
- Monitoring: directly (intrauterine pressure catheter) or indirectly (tocodynamometer)
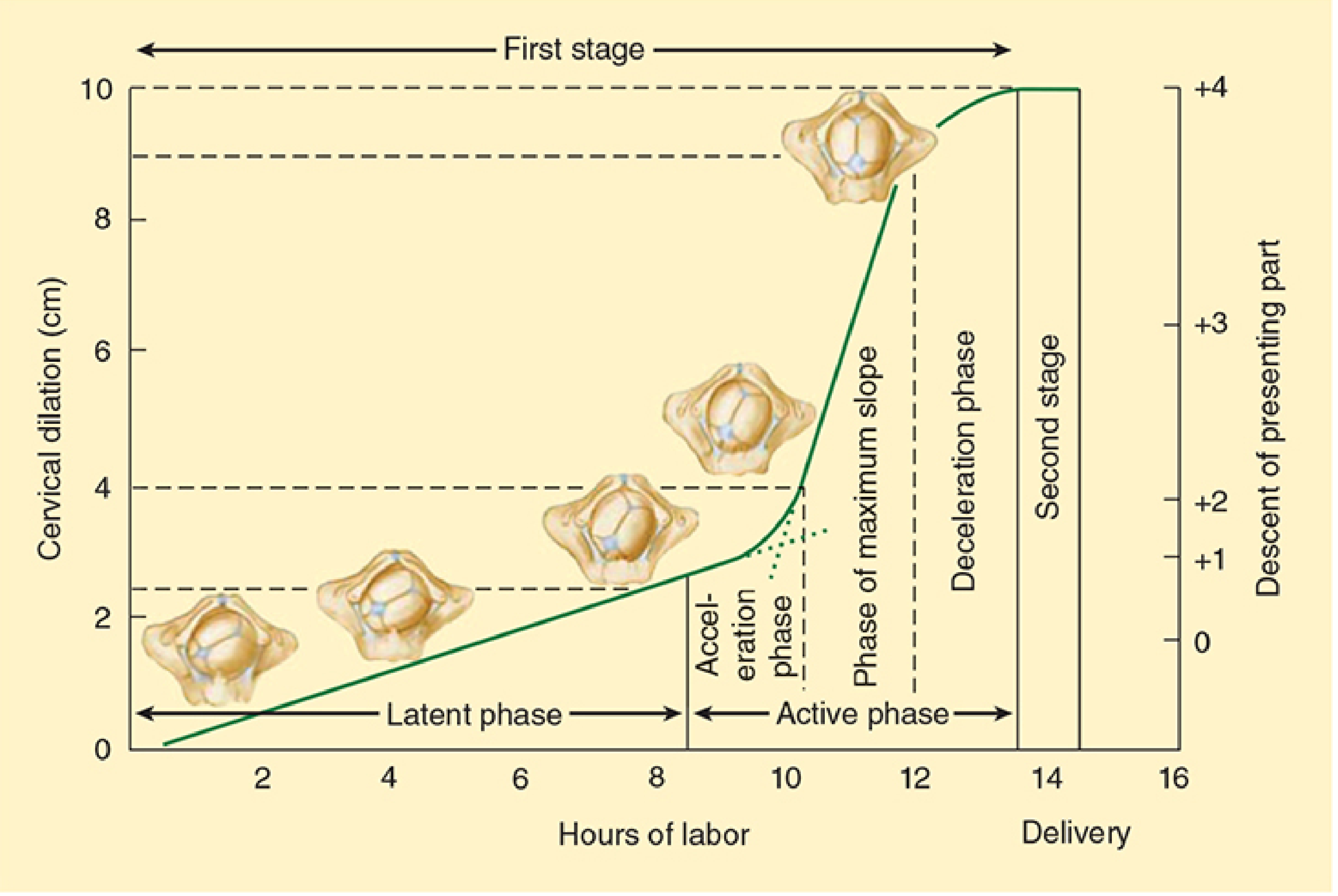
4. Stages of Labor
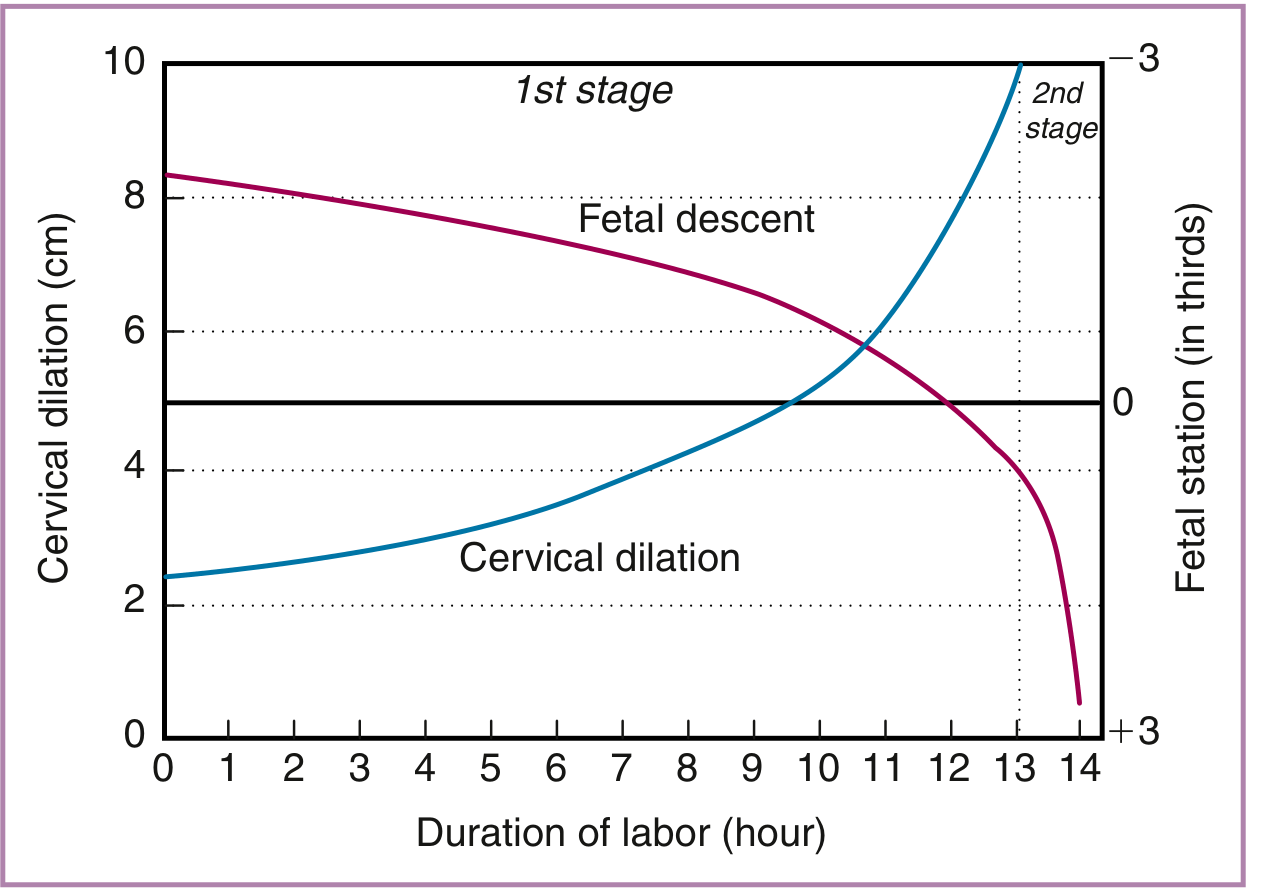
The normal labor curve showing latent phase, active phase, and fetal descent. — Morgan & Mikhail's Clinical Anesthesiology
| Stage | Onset | Completion |
|---|
| First (latent + active phases) | Onset of true labor | Complete cervical dilation (10 cm) |
| Second | Full dilation | Delivery of baby |
| Third | Delivery of baby | Delivery of placenta |
| Fourth (not universally counted) | Delivery of placenta | Contracted uterus, ~1–2 hrs |
First Stage
Latent phase:
- Cervical effacement and dilation from 0 to ~4–5 cm
- Rate typically ≤0.6 cm/hr
- Normal duration: <20 hours (nullipara); <14 hours (multipara)
- Contractions begin at 15–20 min apart
Active phase:
- Begins ~4–5 cm dilation; cervix dilates to 10 cm
- Contractions: 3–5 min apart
- Minimum dilation rate: ≥1.2 cm/hr (nullipara); ≥1.5 cm/hr (multipara) — Friedman's criteria
- Total first stage: 8–12 hours (nullipara); 5–8 hours (multipara)
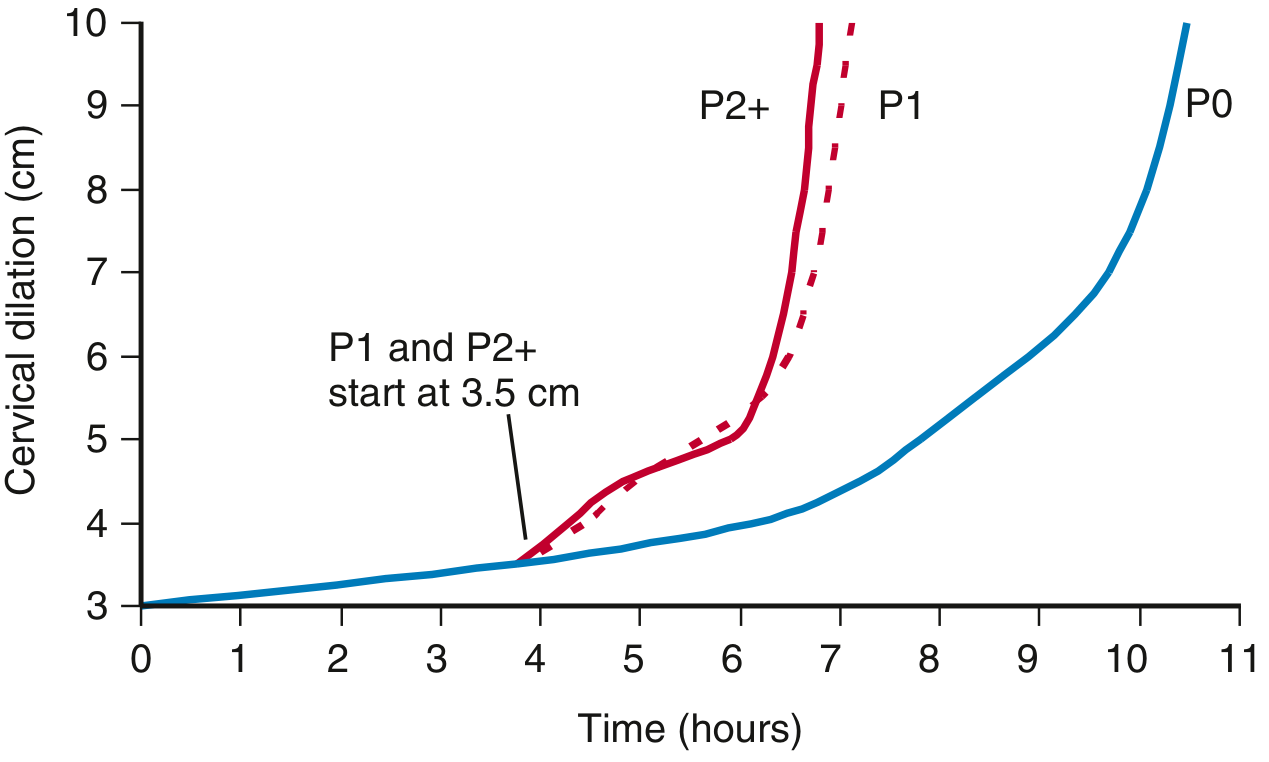
Zhang's updated labor duration data (National Collaborative Perinatal Project):
| Cervical Dilation | Parity 0 median (95th %) | Parity 1 | Parity 2+ |
|---|
| 4 → 5 cm | 0.9 h (4.5 h) | 0.7 h (3.3 h) | 0.7 h (3.5 h) |
| 5 → 6 cm | 0.6 h (2.6 h) | 0.4 h (1.6 h) | 0.4 h (1.6 h) |
| 6 → 7 cm | 0.5 h (1.8 h) | 0.4 h (1.2 h) | 0.3 h (1.2 h) |
| 7 → 8 cm | 0.4 h (1.4 h) | 0.3 h (0.8 h) | 0.3 h (0.7 h) |
| 8 → 10 cm | 0.8 h | 0.5 h | 0.4 h |
| Total 4 → 10 cm | 3.7 h (16.7 h) | 2.4 h (13.8 h) | 2.2 h (14.2 h) |
— Creasy & Resnik's Maternal-Fetal Medicine
Key insight: A 2-hour arrest cutoff is too short below 6 cm; a 4-hour limit is excessive after 6 cm. Modern practice adjusts thresholds by dilation.
P0 = nullipara, P1 = parity 1, P2+ = parity 2+. — Creasy & Resnik's Maternal-Fetal Medicine
Second Stage
- Full dilation → delivery of baby
- Contractions: 1.5–2 min apart, lasting 1–1.5 min
- Maternal bearing down greatly augments intrauterine pressure
- Duration: 20 min (multipara) to 50 min (nullipara) average
- Concern threshold (without epidural): >2 hours nullipara; >1 hour multipara
- With epidural: >3 hours nullipara; >2 hours multipara — Textbook of Family Medicine
Patterns of cervical dilation and fetal descent in nulliparas. — Creasy & Resnik's Maternal-Fetal Medicine
Third Stage
- Delivery of baby → delivery of placenta
- Typically 15–30 minutes
- Active management: oxytocin administration before placental delivery reduces uterine atony and postpartum haemorrhage (PPH)
5. Cardinal Movements of Labor (Vertex Presentation)
The fetal head negotiates the curved birth canal through a sequence of 7 cardinal movements:
| # | Movement | Description |
|---|
| 1 | Engagement | Biparietal diameter passes through pelvic inlet; fetal head at or below ischial spines (station 0) |
| 2 | Descent | Progressive downward movement through the pelvis; continues throughout |
| 3 | Flexion | Chin tucks to chest; reduces presenting diameter (suboccipitobregmatic ~9.5 cm vs. occipitofrontal ~11.5 cm); essential for negotiation |
| 4 | Internal rotation | Occiput rotates anteriorly from transverse to occiput anterior (OA) position to align with anteroposterior diameter of outlet |
| 5 | Extension | Head extends as it passes under the pubic symphysis; occiput, brow, face, and chin sequentially sweep over perineum |
| 6 | External rotation (restitution) | Head rotates back to align with fetal shoulders after delivery of head |
| 7 | Expulsion | Anterior shoulder, posterior shoulder, then body delivered |
— Roberts & Hedges' Clinical Procedures; Tintinalli's Emergency Medicine; Textbook of Family Medicine
Flexion is the most critical movement — it reduces the presenting diameter and allows easier descent.
6. Fetal Station
Descent of the presenting part is described relative to the ischial spines:
- Station 0 = presenting part at level of ischial spines
- −1, −2, −3 = above spines (cm)
- +1, +2, +3 = below spines; +3 = crowning
7. Effect of Labor on Maternal Physiology
(Morgan & Mikhail's Clinical Anesthesiology)
| System | Change During Labor |
|---|
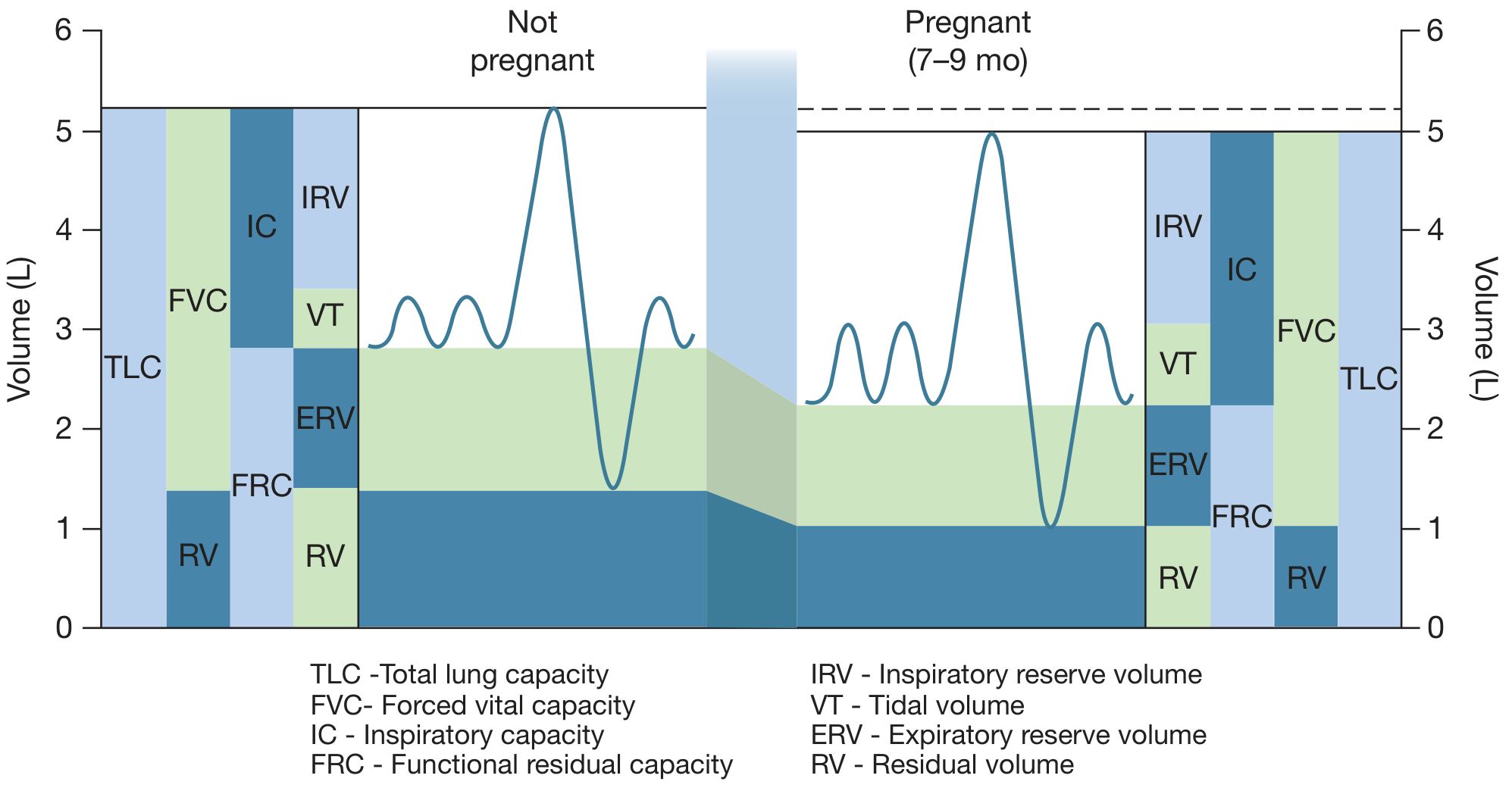
| Respiratory | Minute ventilation ↑ up to 300% during intense contractions; O₂ consumption ↑ additional 60% above T3 values; PaCO₂ may drop below 20 mm Hg with hyperventilation → transient maternal/fetal hypoxaemia between contractions; uterine blood flow ↓ with excessive hyperventilation |
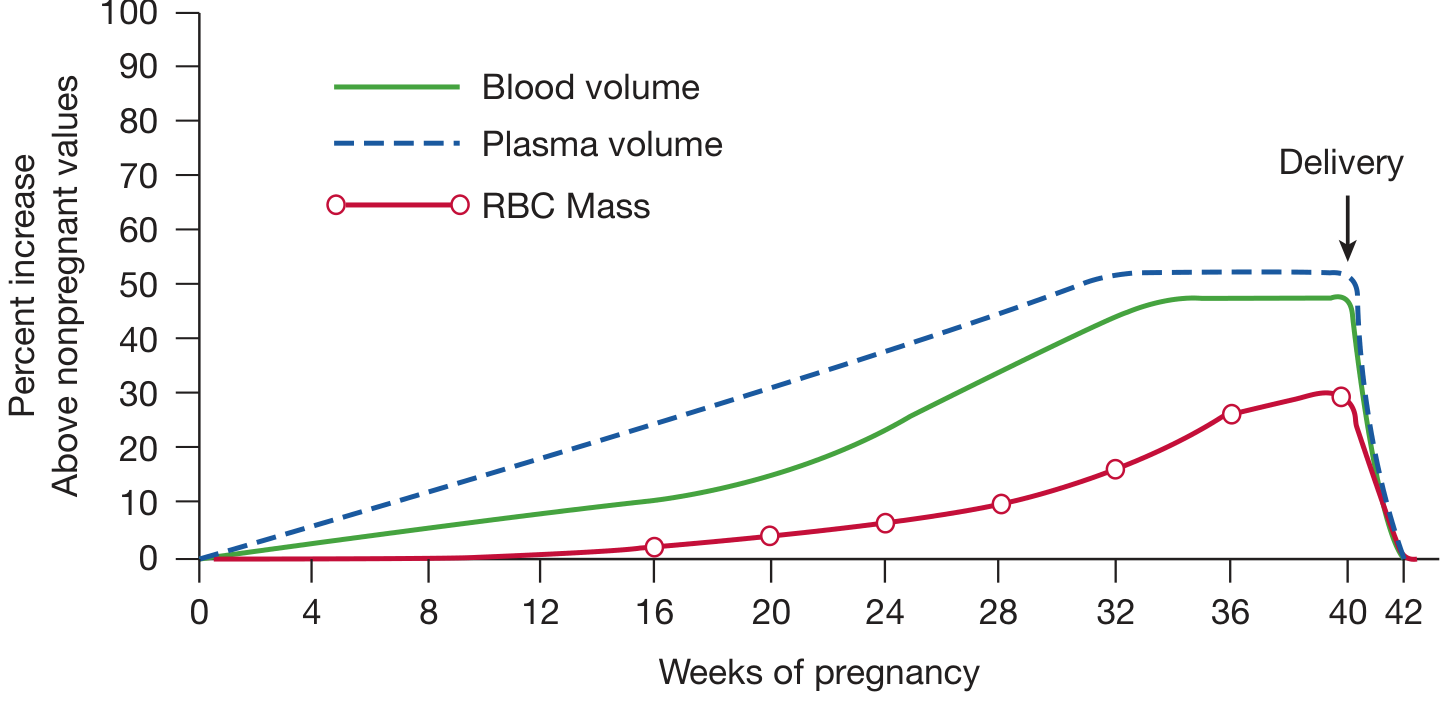
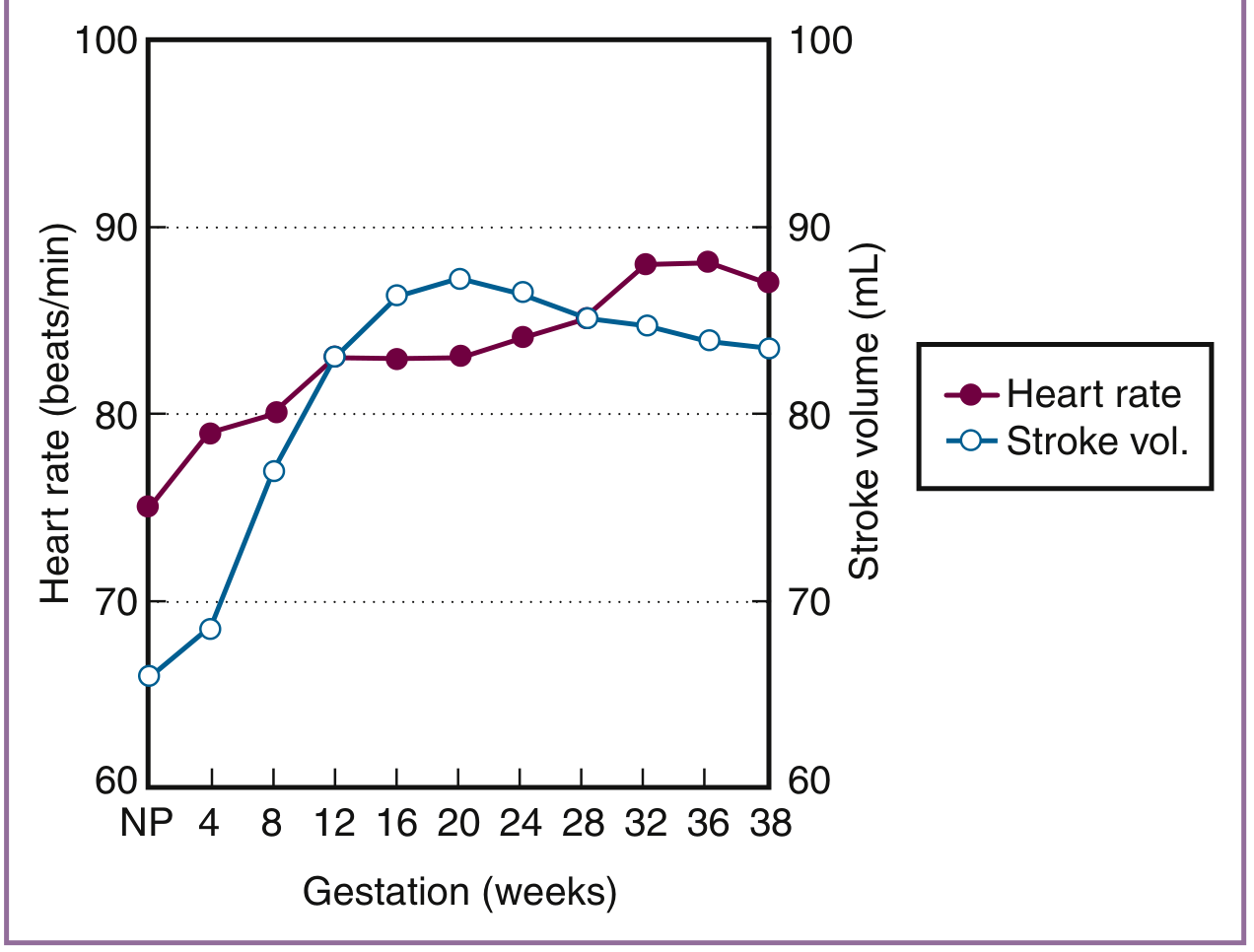
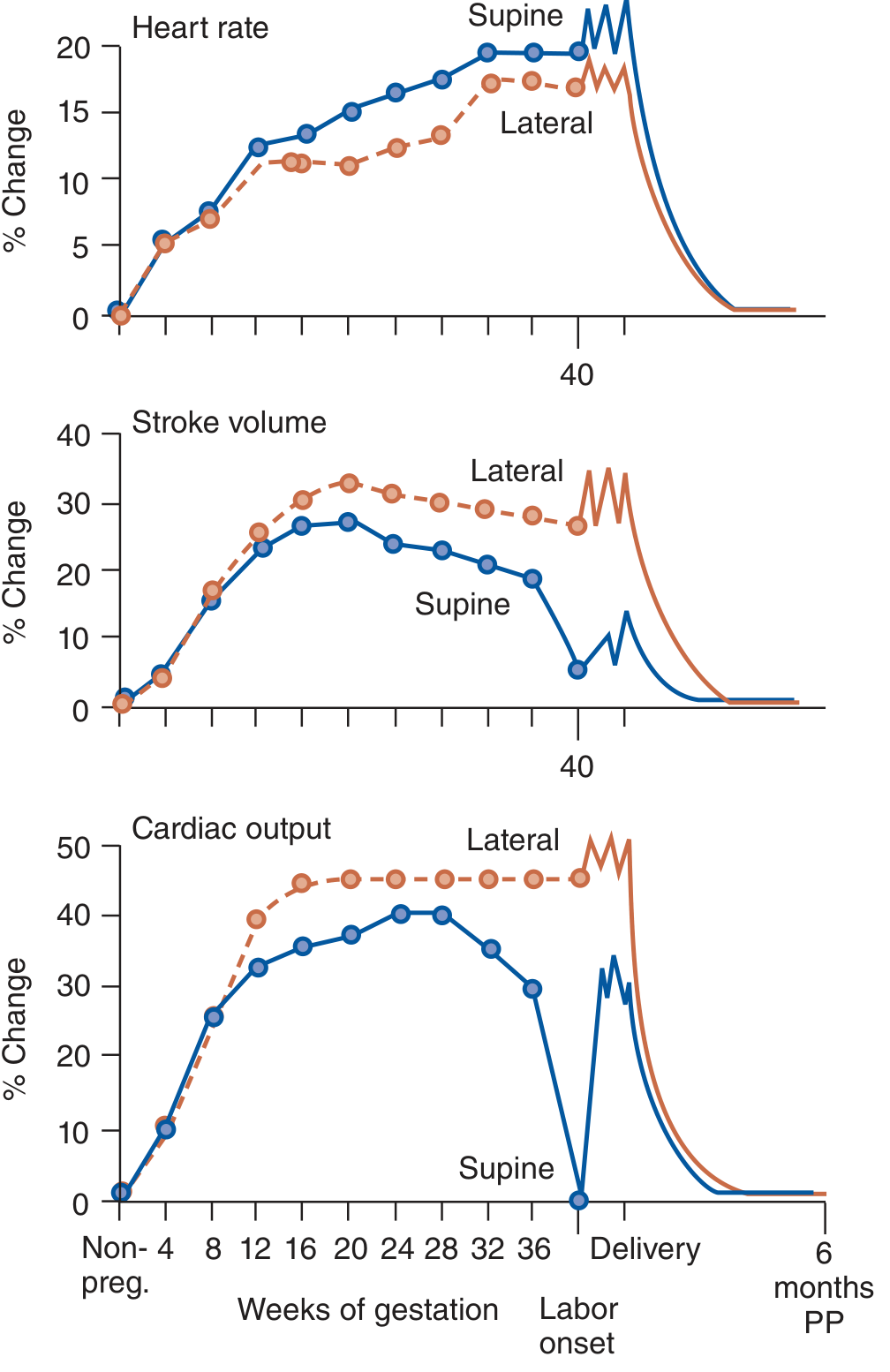
| Cardiovascular | Each contraction autotransfuses 300–500 mL → CO ↑ 45% above T3 values; immediately postpartum: CO rises up to 80% above late T3 values (IVC decompression + uterine autotransfusion) |
| Haematological | WBC may rise to 20,000/µL in first 24h postpartum (normal) |
| Pain | Stage 1 pain: visceral, from uterine contractions + cervical dilation (T10–L1); Stage 2: somatic, from perineal/vaginal distension (S2–S4) |
| Metabolic | Hyperventilation + pain → respiratory alkalosis; severe cases can cause tetany |
PART B — THE PARTOGRAM
1. Definition & Purpose
The partogram (partograph) is a graphical record of labor progress, maternal condition, and fetal well-being plotted over time. It was introduced by Friedman and popularised by Philpott & Castle, and subsequently adopted by the WHO.
A WHO multi-centre trial demonstrated that use of the partogram reduced:
- Prolonged labors
- Emergency caesarean deliveries
- Use of oxytocin augmentation
A Norwegian cluster-RCT comparing WHO vs. Zhang-based partograms found both reduced caesarean rates compared to historical controls. — Creasy & Resnik's Maternal-Fetal Medicine
2. Components of the WHO Partogram
Section 1 — Fetal Condition:
- Fetal heart rate (every 30 min; recorded as dots on graph, normal 110–160 bpm)
- Membranes and amniotic fluid (I = intact; C = clear; M = meconium; B = blood)
- Moulding (0 = bones separated; 1 = touching; 2 = overlapping but reducible; 3 = fixed overlap)
Section 2 — Progress of Labor (the Cervicograph):
- Cervical dilation — plotted on the Y-axis (0–10 cm); time on X-axis
- Fetal descent — plotted separately (station or fifths of head palpable abdominally)
- Alert line — drawn from 4 cm at 1 cm/hr; represents the slowest acceptable active-phase progress
- Action line — drawn 4 hours to the right of the alert line; crossing this line = indication for intervention (amniotomy, oxytocin augmentation, or operative delivery)
- Uterine contractions: frequency and duration plotted per 10-minute window
Section 3 — Maternal Condition:
- BP, pulse, temperature (hourly/4-hourly)
- Urine: volume, protein, acetone
- Drugs and IV fluids given
- Oxytocin dose if used
3. Interpreting the Partogram
| Finding | Interpretation |
|---|
| Cervical dilation curve left of alert line | Normal labor progress |
| Curve between alert and action lines | Slow progress — watchful waiting; consider amniotomy |
| Curve at or beyond action line | Abnormal labor — intervention required |
| Latent phase >20h (nullipara), >14h (multipara) | Prolonged latent phase |
| Active phase dilation <1.2 cm/hr (nullipara) <1.5 cm/hr (multipara) | Protracted active phase |
| Arrest of dilation for ≥2 hours in active phase | Secondary arrest — assess CPD, consider oxytocin/CS |
| Fetal descent <1 cm/hr (nullipara) <2 cm/hr (multipara) in 2nd stage | Protracted descent |
4. Dysfunctional Labor Patterns
| Pattern | Definition | Management |
|---|
| Prolonged latent phase | >20h nullipara; >14h multipara | Rest (therapeutic morphine), observation, ± oxytocin; NOT an indication for CS |
| Protracted active phase | <1.2 cm/hr (nullipara); <1.5 cm/hr (multipara) | Oxytocin augmentation; assess CPD, malposition |
| Secondary arrest | Cessation of dilation ≥2h during active phase | Assess adequacy of contractions (IUPC); amniotomy; oxytocin; high association with CPD |
| Protracted descent | <1 cm/hr (nullipara); <2 cm/hr (multipara) | Assess CPD, macrosomia, pushing effort |
| Arrest of descent | No change in station for ≥1h (2nd stage) | Oxytocin if contractions inadequate; operative delivery if CPD |
— Textbook of Family Medicine; Creasy & Resnik's Maternal-Fetal Medicine
5. Active Management of Labor
Developed at the National Maternity Hospital, Dublin — applied to nulliparas with:
- Singleton pregnancy
- Vertex presentation
- Regular contractions
Protocol:
- Diagnosis of labor = ≥1 of: bloody show, complete effacement, ruptured membranes
- Early amniotomy
- Oxytocin if dilation <1 cm/hr at 1h review — titrated to ≥7 contractions per 15 min
- Partogram used to time all interventions
Studies showed reduction in CS rate and prolonged labor. — Creasy & Resnik's Maternal-Fetal Medicine
PART C — POSTPARTUM PERIOD (PUERPERIUM)
1. Definition
The puerperium is the period during which the mother's altered anatomy, physiology, and biochemistry return to the non-pregnant state. It:
- Begins at the third stage of labor (delivery of placenta)
- Completes at approximately 6 weeks postpartum
— Textbook of Family Medicine
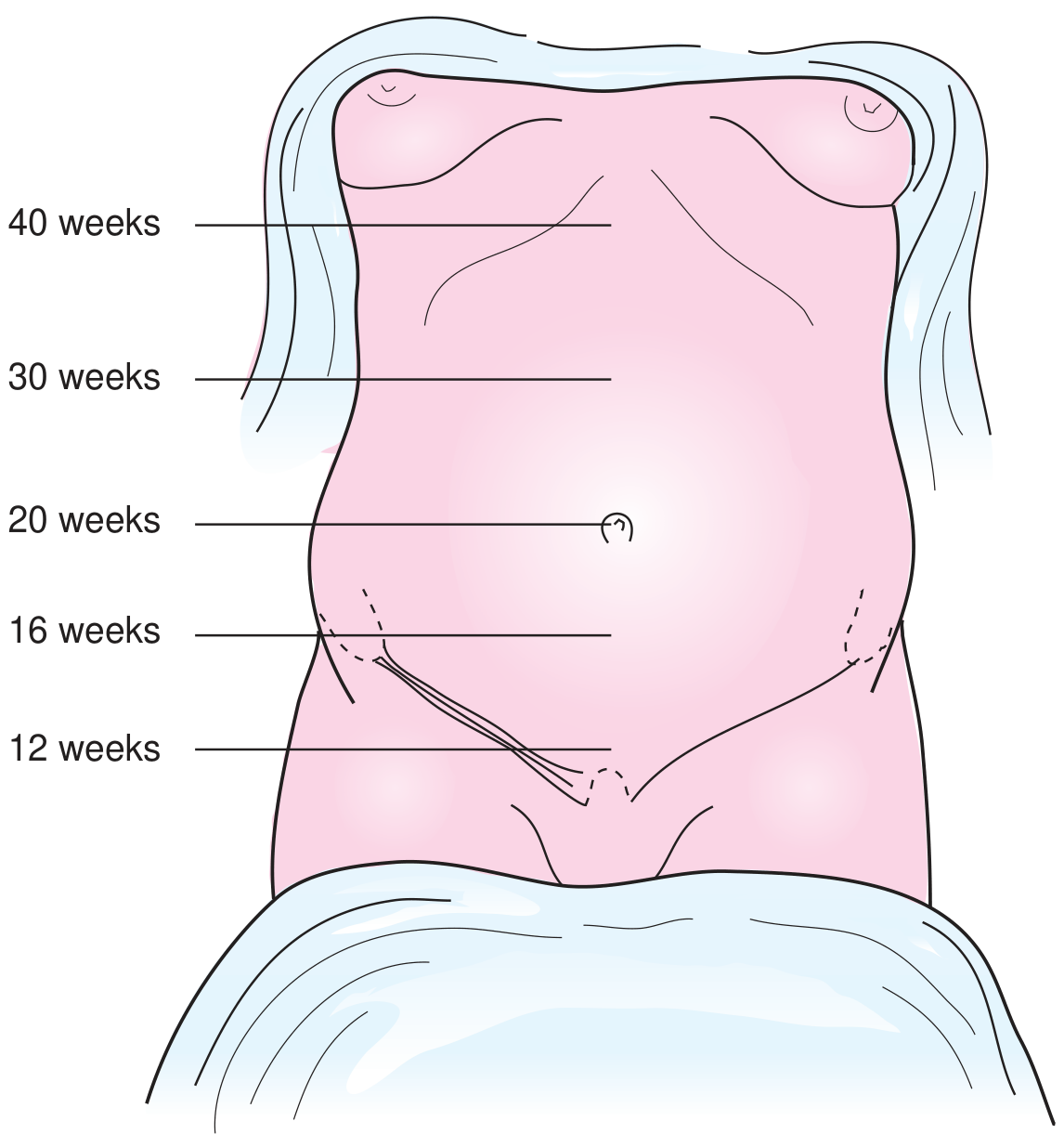
2. Uterine Involution
| Timepoint | Uterine Status |
|---|
| Immediately postpartum | Fundus at umbilicus, firm |
| 24 hours | Fundus at or just above umbilicus |
| 5–7 days | Firm, non-tender; midway between symphysis and umbilicus |
| 2 weeks | No longer palpable abdominally |
| 6 weeks | Returns to near pre-pregnancy size |
Involution is driven by uterine contractions ("afterpains") which can be painful and may require analgesia. Breastfeeding stimulates oxytocin release → promotes involution and reduces bleeding.
Subinvolution — failure of normal involution; causes include retained placental fragments, infection (endometritis).
3. Lochia
| Type | Timing | Appearance |
|---|
| Lochia rubra | Days 1–3 (to 4) | Grossly bloody, red |
| Lochia serosa | Days 4–10 | Pinkish-brown, serous; decreasing volume |
| Lochia alba | Days 7–10 onwards | Pale yellow-white; very low volume |
Total lochia duration: ~4–6 weeks but highly variable. Persistent heavy bleeding suggests retained placenta or subinvolution.
— Textbook of Family Medicine
4. Cardiovascular & Haematological Changes
- Pulse rate drops within the first 24 hours
- WBC increases markedly — up to 20,000/µL in first 24h (normal physiologic response)
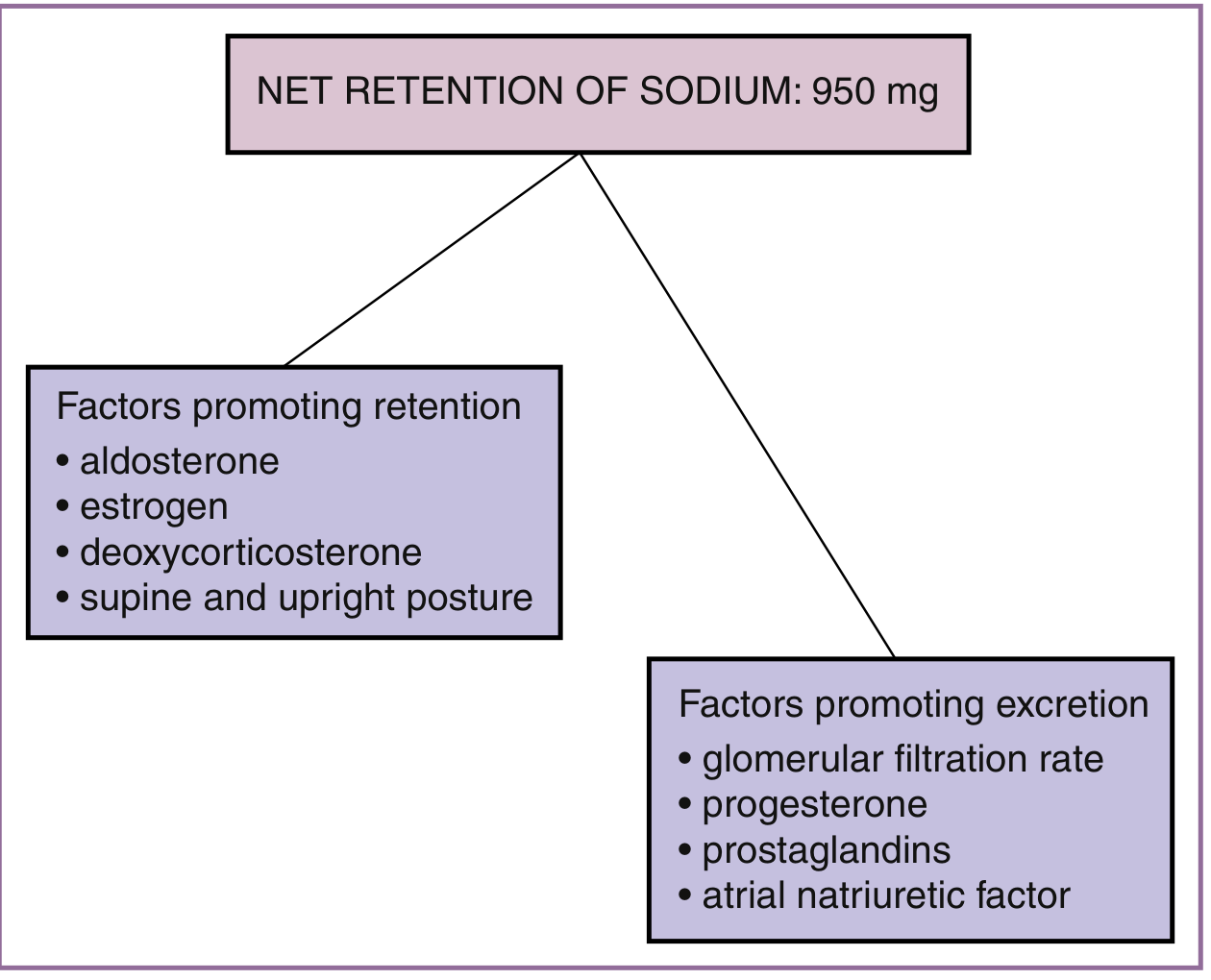
- Diuresis occurs — urine output temporarily increases, reflecting mobilisation of accumulated extravascular fluid (the ~8–9 L water gained in pregnancy)
- Haematocrit may be artificially elevated for a few days (diuresis reduces plasma volume before RBCs clear)
- Cardiac output peaks immediately postpartum (up to 80% above late T3 values) due to IVC decompression and autotransfusion, then declines over 2–6 weeks
- Greatest cardiac strain is immediately postpartum — relevant for women with cardiac disease
- May contain protein and glucose in urine transiently
5. Breastfeeding & Lactation
- Breastfeeding can be initiated immediately after delivery
- Benefits: promotes uterine involution, reduces PPH, provides infant nutrition and immunity
- Hormonal basis: high prolactin → milk production; suckling maintains prolactin; oestrogen and progesterone levels remain low during exclusive breastfeeding → amenorrhoea and ovulation suppression (lactational amenorrhoea method — ~98% contraceptive efficacy if fully breastfeeding, amenorrhoeic, <6 months postpartum)
- Most medications are secreted in breast milk — avoid meperidine (pethidine) in breastfeeding mothers (long half-life metabolite accumulates in neonates)
6. Postpartum Psychological Changes
(Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
| Condition | Timing | Features |
|---|
| Baby blues | Days 1–5, peaks day 3–4 | Tearfulness, mood lability, anxiety; self-limiting; no treatment required |
| Postpartum depression (PPD) | Within 4 weeks to 1 year; peaks at 4–6 weeks | Persistent low mood, anhedonia, poor bonding, sleep/appetite disturbance; prevalence ~10–15%; treat with CBT ± antidepressants |
| Postpartum psychosis | Within days to 2 weeks | Hallucinations, delusions, confusion, disorganised behaviour; rare (~1–2/1000); psychiatric emergency — admit |
Risk factors for PPD: prior depression, lack of social support, stressful life events, SUD, intimate partner violence.
7. Resumption of Menstruation & Ovulation
- Non-breastfeeding women: ovulation returns as early as 3–4 weeks postpartum; menstruation typically 6–8 weeks postpartum
- Breastfeeding women: ovulation and menstruation suppressed during exclusive breastfeeding (lactational amenorrhoea); first ovulation may precede first menstrual period
- Contraception should be discussed before or at the 6-week visit
8. Routine Postpartum Care
| Task | Timing |
|---|
| Uterine massage; monitor for atony/PPH | Every 15 min × 1 hour after delivery |
| Oxytocin 10 IU IM or IV infusion | Immediately after delivery (active management of 3rd stage) |
| Bladder care — encourage voiding | Prevent overdistension; rapid diuresis when oxytocin discontinued |
| Episiotomy care | Sitz baths; analgesia as needed |
| Full ambulation | As soon as possible post-delivery |
| Check BP, temperature, pulse, lochia | Regularly in 24h; then at 6-week visit |
| 6-week postnatal check | BP, weight, wound, emotional wellbeing, contraception counselling |
| Perineal laceration repair | 1st–2nd degree: local repair; 3rd–4th degree: formal repair in theatre |
9. Postpartum Haemorrhage (PPH)
- Primary PPH: ≥500 mL blood loss within 24h of delivery (≥1,000 mL for CS)
- Secondary PPH: abnormal bleeding between 24h and 12 weeks postpartum
- Causes (4 T's): Tone (uterine atony — most common, 80%), Trauma (lacerations, uterine rupture), Tissue (retained placenta), Thrombin (coagulopathy)
- First-line management: uterotonic agents (oxytocin, ergometrine, misoprostol, carboprost)
- If uterotonics fail after vaginal delivery: exploratory laparotomy — Textbook of Family Medicine
Quick Reference Summary
| Topic | Key Facts |
|---|
| True labor contractions | 25–60 mm Hg; initially 15–20 min apart |
| First stage duration | 8–12h (nullipara); 5–8h (multipara) |
| Active phase rate | ≥1.2 cm/hr nullipara; ≥1.5 cm/hr multipara |
| Second stage | 50 min average (nullipara); 20 min (multipara) |
| Cardinal movements | Engagement → descent → flexion → internal rotation → extension → external rotation → expulsion |
| Partogram alert line | 1 cm/hr from 4 cm |
| Partogram action line | 4 hours right of alert line |
| CO change in labor | ↑ 45% during contractions; ↑ up to 80% immediately postpartum |
| Lochia rubra | Days 1–4 (bloody) |
| Lochia serosa | Days 4–10 (pinkish-brown) |
| Lochia alba | Day 7–10+ (pale yellow-white) |
| Uterine involution | Not palpable abdominally by 2 weeks |
| PPD timing | Peaks 4–6 weeks; treat with CBT ± antidepressants |
| Menstruation resumes | 6–8 weeks (non-breastfeeding); delayed with exclusive breastfeeding |
Sources: Morgan & Mikhail's Clinical Anesthesiology 7e · Creasy & Resnik's Maternal-Fetal Medicine · Textbook of Family Medicine 9e · Roberts & Hedges' Clinical Procedures · Tintinalli's Emergency Medicine · Kaplan & Sadock's Comprehensive Textbook of Psychiatry