hf treatment
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"heart failure" AND treatment
Finding Sources
Searching PubMed
"heart failure" AND "pharmacological treatment"
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
I have the treatment algorithm image and comprehensive textbook content. I now have enough to write a thorough, well-cited response on heart failure treatment. Let me compile the answer.
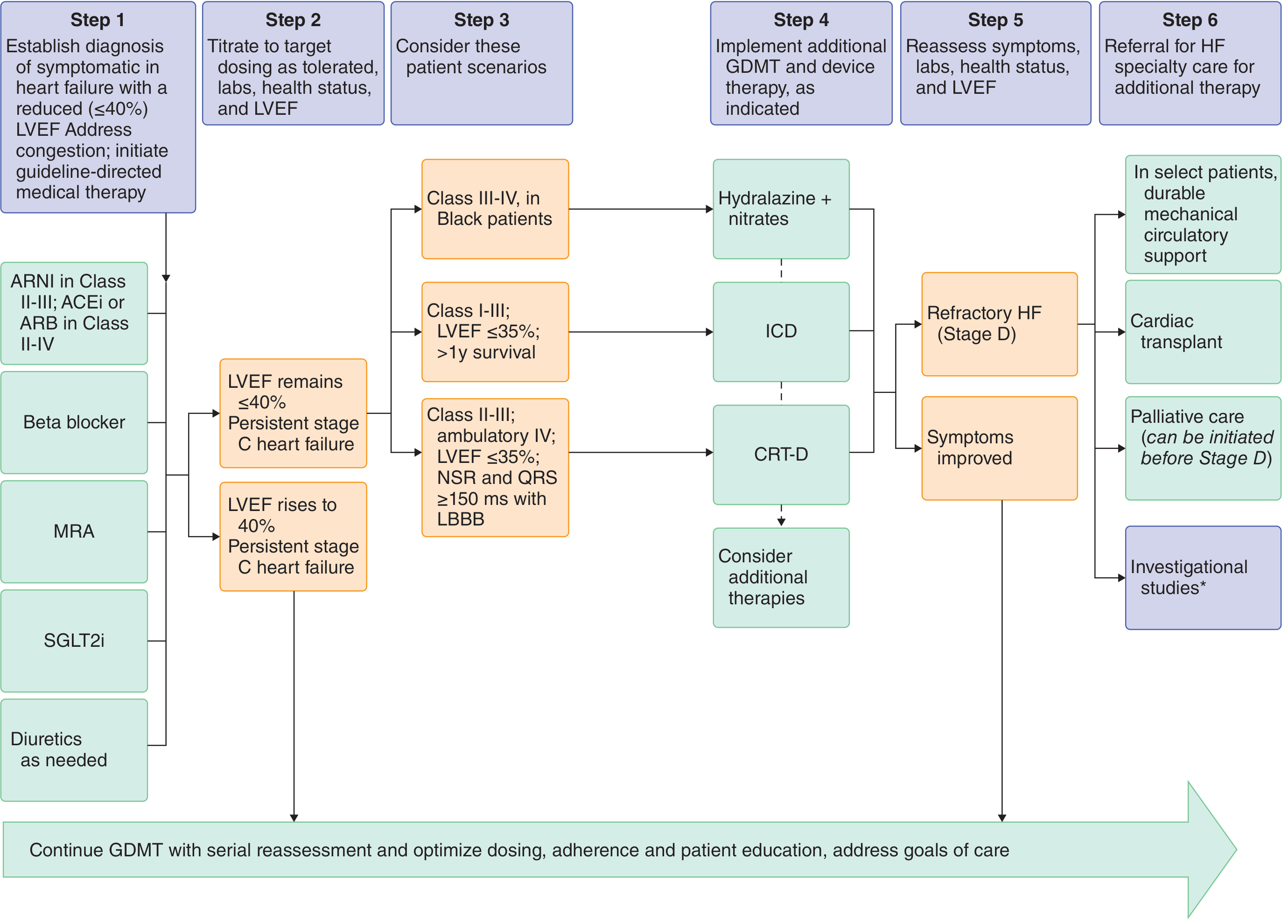
Heart Failure (HF) Treatment
Heart failure is classified primarily by ejection fraction: HFrEF (reduced EF, LVEF ≤40%), HFmrEF (mildly reduced, 41-49%), and HFpEF (preserved, ≥50%). Treatment strategies differ significantly.
HF with Reduced Ejection Fraction (HFrEF) - The "Fantastic Four"
Current evidence supports four foundational, life-saving drug classes that should be initiated as quickly as possible in any order, then up-titrated to target doses (Goldman-Cecil Medicine):
1. ARNI (Angiotensin Receptor - Neprilysin Inhibitor) - Preferred over ACE inhibitor/ARB
- Drug: Sacubitril/valsartan (Entresto)
- Indication: NYHA Class II-III (preferred); ACEi or ARB used for Class II-IV if ARNI not tolerated
- Key rule: Never combine with ACEi (risk of angioedema); must have 36-hour washout from ACEi before starting
- Reduces mortality, hospitalizations, and symptoms more than enalapril (PARADIGM-HF trial)
- Goldman-Cecil Medicine, p. 479
2. Beta-Blockers
- Drugs with proven benefit: Carvedilol, bisoprolol, metoprolol succinate (extended-release)
- Mechanism: Counteract chronic sympathetic overdrive; reduce heart rate, prevent hypertrophy and myocyte apoptosis
- Beta-blockers reduced all-cause mortality by ~27% in patients in sinus rhythm in pooled trial analysis
- "Start low, go slow" - titrate up every 2 weeks; avoid initiation during acute decompensation
- Contraindications: Asthma, 2nd/3rd degree AV block
- Goldman-Cecil Medicine, p. 483
3. Mineralocorticoid Receptor Antagonist (MRA)
| Drug | Starting Dose | Target Dose |
|---|---|---|
| Spironolactone | 25 mg once daily | 25-50 mg once daily |
| Eplerenone | 25 mg once daily | 50 mg once daily |
- Reduce morbidity and mortality in moderate-severe HF; aldosterone causes myocardial/vascular fibrosis beyond its renal effects
- Monitor: K+ at 1, 4, 8, 12 weeks; stop if K+ >6.0 mmol/L or creatinine >310 µmol/L
- Eplerenone causes less gynecomastia than spironolactone
- Goldman-Cecil Medicine, p. 485; Katzung's Basic and Clinical Pharmacology, 16e
4. SGLT2 Inhibitors
- Drugs: Dapagliflozin (Farxiga) or Empagliflozin (Jardiance)
- Indication: NYHA Class II-IV with LVEF ≤40%; first-line regardless of diabetes status
- Benefits: Improve survival, reduce hospitalizations, slow eGFR decline, reduce serum uric acid
- Contraindications: Prior DKA, eGFR <20 mL/min/1.73m²; use caution if eGFR <30
- Goldman-Cecil Medicine, p. 485
Diuretics - For Symptom Relief
- Loop diuretics (furosemide) are first choice for fluid overload - reduce preload and pulmonary congestion
- No mortality benefit on their own; used alongside the "fantastic four"
- Thiazides for mild failure only; loop agents for moderate-severe
- Monitor K+ (supplement if needed or add K+-sparing agent)
- Katzung's Basic and Clinical Pharmacology, 16e, p. 345
Additional Pharmacologic Options
| Drug | When to Use |
|---|---|
| Ivabradine | NYHA II-IV, LVEF ≤35%, sinus rhythm, HR ≥70 bpm despite maximally tolerated beta-blocker |
| Vericiguat (soluble guanylate cyclase stimulator) | Persistent NYHA II-IV despite full GDMT after recent HF hospitalization; start 2.5 mg → target 10 mg daily |
| Digoxin | Does not reduce mortality; reduces hospitalization risk; consider if symptomatic despite optimized therapy in sinus rhythm |
| Hydralazine + isosorbide dinitrate | Class III-IV Black patients who can't tolerate ARNI/ACEi/ARB; reduces mortality in this population |
Device Therapy (HFrEF)
ICD (Implantable Cardioverter-Defibrillator)
- LVEF ≤35%, NYHA Class I-III, >1 year expected survival on optimal GDMT
- Prevents sudden cardiac death from ventricular arrhythmia
CRT-D (Cardiac Resynchronization Therapy + Defibrillator) - Class I indication:
- LVEF ≤35%, sinus rhythm, LBBB with QRS ≥150 ms, NYHA Class II-III (or ambulatory IV)
- Improves LV function, symptoms, and reduces mortality
- His-bundle and left bundle branch pacing may match or exceed biventricular pacing outcomes
In patients meeting criteria for both CRT and ICD, a CRT-D device provides additional mortality benefit over ICD alone. - Goldman-Cecil Medicine, CRT section
HF with Preserved Ejection Fraction (HFpEF)
HFpEF is harder to treat - fewer mortality-reducing therapies exist:
- Diuretics: Symptom control (use cautiously - these patients are preload-dependent)
- SGLT2 inhibitors: Now recommended; EMPEROR-Preserved and DELIVER trials show reduced HF hospitalizations
- MRAs: May be useful
- ARNI: Reduces NT-proBNP and symptoms
- Beta-blockers / CCBs: Useful to control heart rate and blood pressure
- Treat underlying causes: Hypertension, obesity, AF, coronary disease
- Digoxin has little or no role in HFpEF - Katzung's Basic and Clinical Pharmacology, 16e, Table 13-4
Acute / Decompensated HF
- IV loop diuretics (furosemide) - cornerstone
- IV vasodilators (nitroprusside, nitroglycerin) - reduce preload/afterload in hypertensive AHF
- Avoid initiating beta-blockers until stabilized
- Inotropes (dobutamine, milrinone) for cardiogenic shock or low-output state
- Positive pressure ventilation (CPAP/BiPAP) for respiratory failure
- Avoid adaptive servo-ventilation (ASV) in patients with central sleep apnea + systolic HF (increased mortality in SERVE-HF trial)
Non-Pharmacologic Measures (All HF)
- Sodium restriction (<2 g/day) and fluid restriction in severe cases
- Daily weight monitoring - alert for >2 kg gain in 2 days
- Exercise rehabilitation - improves functional capacity and quality of life
- Treat precipitating/comorbid conditions: AF, hypertension, anemia, sleep apnea, diabetes
- Vaccination: Influenza, pneumococcal, COVID-19
GDMT Dosing Reference (HFrEF)
| Drug Class | Starting Dose | Target Dose |
|---|---|---|
| Sacubitril/valsartan | 24/26 mg twice daily | 97/103 mg twice daily |
| Carvedilol | 3.125 mg twice daily | 25 mg twice daily |
| Bisoprolol | 1.25 mg once daily | 10 mg once daily |
| Metoprolol succinate | 12.5-25 mg once daily | 200 mg once daily |
| Enalapril (if ARNI not used) | 2.5 mg twice daily | 10-20 mg twice daily |
| Lisinopril | 2.5-5 mg once daily | 20-35 mg once daily |
| Spironolactone | 25 mg once daily | 25-50 mg once daily |
| Dapagliflozin | 10 mg once daily | 10 mg once daily |
Source: Goldman-Cecil Medicine International Edition; Katzung's Basic and Clinical Pharmacology, 16e; Braunwald's Heart Disease; 2022 AHA/ACC/HFSA HF Guidelines
This is a shared conversation. Sign in to Orris to start your own chat.