Complete detail about shock from basics to clinical points of view as MBBS level
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive material from Robbins Pathology, Sabiston Surgery, Rosen's Emergency Medicine, Guyton & Hall Physiology, and other textbooks. I have everything needed to write a thorough MBBS-level guide on shock. Let me compile the full response now.
SHOCK - Complete MBBS Guide
Sources: Robbins & Cotran Pathologic Basis of Disease; Sabiston Textbook of Surgery; Guyton & Hall Textbook of Medical Physiology; Rosen's Emergency Medicine; Tintinalli's Emergency Medicine; Bailey & Love's Surgery; Katzung Pharmacology
1. DEFINITION
Shock is a state of circulatory failure that impairs tissue perfusion and causes cellular hypoxia. At the outset, the cellular injury is reversible; however, prolonged shock eventually leads to irreversible tissue injury and can be fatal. (Robbins & Cotran, p. 134)
A more operational definition from Sabiston Surgery: "Inadequate perfusion of tissue" - the most critical nutrient being oxygen, but blood carries countless other nutrients, buffers, cells, antibodies, and hormones that are all compromised in shock.
Key point from Rosen's EM: Shock can occur with a normal arterial blood pressure - not all hypotension is shock, and not all shock involves hypotension.
2. CLASSIFICATION OF SHOCK
2A. Traditional 4-Category Classification
| Type | Mechanism | Common Causes |
|---|---|---|
| Hypovolemic | Reduced preload (low blood/plasma volume) | Hemorrhage, vomiting, diarrhea, burns, trauma |
| Cardiogenic | Pump failure (reduced CO from heart) | MI (>40% myocardium dysfunctional), arrhythmia, cardiac tamponade, PE, valvular disease |
| Distributive | Vasodilation + maldistribution of blood flow | Sepsis, anaphylaxis, neurogenic (spinal cord injury) |
| Obstructive | Mechanical impedance to flow | PE, tension pneumothorax, cardiac tamponade |
(Rosen's EM; Mulholland & Greenfield Surgery)
2B. Robbins Pathology Classification (3 broad groups)
| Type | Clinical Example | Principal Mechanism |
|---|---|---|
| Cardiogenic | MI, ventricular rupture, arrhythmia, tamponade, PE | Failure of myocardial pump from intrinsic damage, extrinsic compression, or outflow obstruction |
| Hypovolemic | Hemorrhage, vomiting, diarrhea, burns, trauma | Inadequate blood or plasma volume |
| Septic | Overwhelming bacterial/fungal infections | Cytokine cascades; peripheral vasodilation; endothelial activation/injury; leukocyte damage; DIC |
Other less common types: Neurogenic (spinal cord injury - acute vasodilation from lost sympathetic tone) and Anaphylactic (IgE-mediated hypersensitivity - acute vasodilation and hypotension).
3. BASIC PHYSIOLOGY: WHAT DETERMINES CARDIAC OUTPUT?
Understanding shock requires understanding what maintains perfusion:
- CO = HR × SV (cardiac output = heart rate × stroke volume)
- SV is determined by: Preload, Afterload, Contractility
- MAP ≈ CO × SVR (mean arterial pressure = cardiac output × systemic vascular resistance)
- DO₂ = CO × CaO₂ (oxygen delivery = cardiac output × arterial oxygen content)
Shock occurs when DO₂ falls below tissue oxygen demand (VO₂). The body compensates initially, but progressive shock overwhelms all compensatory mechanisms.
4. CELLULAR/SUBCELLULAR PATHOPHYSIOLOGY
From Rosen's EM: "At the subcellular level, shock first affects the mitochondria. Mitochondria function at the lowest oxygen tension in the body but consume almost all the oxygen used by the body. More than 95% of aerobic chemical energy comes from mitochondrial combustion of fuel substrates."
When oxygen is inadequate:
- Aerobic metabolism fails
- Anaerobic glycolysis takes over → lactic acid accumulates
- ATP depletion → failure of Na⁺/K⁺-ATPase pump → cellular swelling
- Ca²⁺ influx → activation of destructive enzymes (phospholipases, proteases)
- Mitochondrial damage becomes irreversible
- Cell death - apoptosis then necrosis
Lactate is the earliest and most sensitive marker of cellular hypoperfusion. Lactate >4 mmol/L = severe shock with risk of multi-organ failure.
5. STAGES OF SHOCK (Guyton & Hall Physiology)
Stage 1: Compensated (Nonprogressive) Shock
The body activates negative feedback mechanisms to restore perfusion:
- Baroreceptor reflexes - powerful sympathetic stimulation of the circulation
- CNS ischemic response - extreme sympathetic drive when MAP falls below 50 mmHg
- Reverse stress-relaxation - blood vessels contract around diminished volume
- RAAS activation - renin → angiotensin II → vasoconstriction + Na⁺/water retention
- ADH (vasopressin) release from posterior pituitary - vasoconstriction + water retention
- Catecholamine release from adrenal medulla (epinephrine, norepinephrine) - tachycardia, vasoconstriction
- Volume restoration - absorption from intestinal tract, interstitial fluid redistribution, thirst, salt appetite
Sympathetic reflexes and catecholamines act within 30 seconds to a few minutes. RAAS and ADH take 10-60 minutes. Volume redistribution takes 1-48 hours.
Clinical signs: Tachycardia, cool peripheries, narrowed pulse pressure, anxiety - but BP is maintained.
Stage 2: Progressive Shock
Positive feedback (vicious cycles) overwhelm compensation:
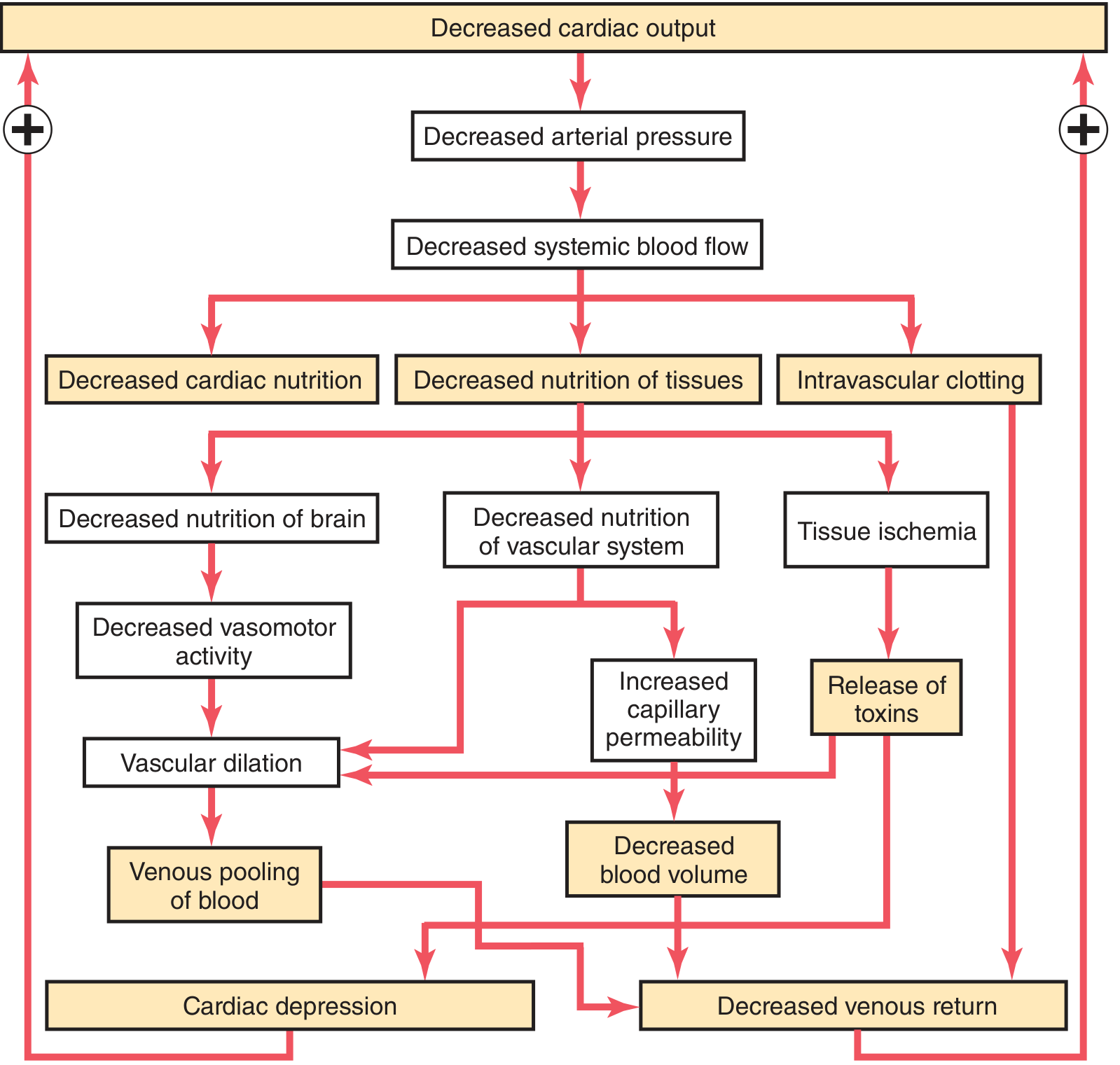
Key vicious cycles:
- Cardiac depression: Low coronary flow → weak myocardium → lower CO → lower coronary flow
- Vasomotor center failure: Cerebral ischemia → reduced vasomotor activity → vascular dilation → venous pooling → decreased venous return → lower CO
- Increased capillary permeability: Tissue ischemia releases toxins → capillary leak → decreased blood volume → lower CO
- Intravascular clotting: Stasis + activated coagulation → DIC → organ ischemia
Clinical signs: Hypotension, oliguria (<0.5 mL/kg/hr), confusion, cold clammy skin.
Stage 3: Irreversible Shock
- Progressive microvascular failure
- Ischemic bowel → absorption of endotoxins
- Lysosomal enzyme release from ischemic cells
- Cardiac failure refractory to treatment
- Multi-organ failure (MOF)
- Death
6. HEMORRHAGIC SHOCK - ATLS CLASSIFICATION
The ATLS (Advanced Trauma Life Support) classification of hemorrhagic shock is the standard clinical framework:
| Parameter | Class I | Class II | Class III | Class IV |
|---|---|---|---|---|
| Blood loss (%) | 0-15% | 15-30% | 30-40% | >40% |
| Blood loss (mL) in 70kg adult | <750 mL | 750-1500 mL | 1500-2000 mL | >2000 mL |
| Pulse (bpm) | <100 | >100 | >120 | >140 |
| Blood pressure | Normal | Normal | Decreased | Decreased |
| Pulse pressure | Normal | Decreased | Decreased | Decreased |
| Respiratory rate | 14-20/min | 20-30/min | 30-40/min | >35/min |
| CNS/Mental status | Slightly anxious | Mildly anxious | Anxious or confused | Confused or lethargic |
| Urine output (mL/h) | >30 | 20-30 | 5-15 | Negligible |
| Fluid resuscitation | Crystalloid | Crystalloid | Crystalloid + Blood | Crystalloid + Blood |
(Sabiston Textbook of Surgery, Table 33.1)
Important caveat (Sabiston): These classes are "problematic because they were not rigorously tested or proven and were admittedly arbitrarily generated." Heart rate, for example, is neither sensitive nor specific for hemorrhage - pain, anxiety, and drugs all alter it. Children compensate well until they crash suddenly; elderly patients decompensate earlier at lower volumes.
Pulse pressure narrows early in hemorrhagic shock due to catecholamine-mediated vasoconstriction raising diastolic BP. This is an early sign before systolic BP falls.
7. SEPTIC SHOCK - PATHOPHYSIOLOGY IN DEPTH
7A. Definition (Robbins & Cotran)
- Sepsis: Life-threatening organ dysfunction caused by a dysregulated host response to infection
- Septic shock: Subset of sepsis with profound circulatory, cellular, and metabolic abnormalities associated with greater mortality than sepsis alone
- SIRS: Sepsis-like condition from nonmicrobial insults (burns, trauma, pancreatitis)
7B. Epidemiology
-
750,000 cases/year in the US; incidence rising
- Mortality rate ~40% despite improvements in care
- Most common trigger: gram-positive bacteria > gram-negative bacteria > fungi
- At least half of cases have no specific organism identified
7C. Pathogenic Steps
1. Microbial triggers:
- PAMPs (pathogen-associated molecular patterns) - endotoxin (LPS) from gram-negatives, enterotoxin B from staph, M protein from streptococci
- DAMPs (damage-associated molecular patterns) from injured host cells
- Detected by TLRs (Toll-like receptors), G-protein-coupled receptors, C-type lectin receptors (Dectin-1 for fungi)
2. Cytokine storm:
- Activation of NF-kB → upregulation of TNF-α, IL-1, IL-6, IL-12, IL-18, IFN-γ
- HMGB1 (late mediator), CRP, procalcitonin elevated
- Reactive oxygen species (ROS), prostaglandins, PAF (platelet-activating factor) released
- Complement activated → anaphylatoxins C3a, C5a → further inflammation
3. Endothelial activation and injury:
- Cytokines loosen tight junctions → vascular leakage → protein-rich edema throughout body
- Upregulation of NO (from iNOS) → vasodilation → hypotension
- Microvascular dysfunction: heterogeneous capillary flow, loss of autoregulation → oxygen delivery/demand mismatch
4. Procoagulant state → DIC:
- Proinflammatory cytokines increase tissue factor from monocytes/endothelial cells
- Decrease of anticoagulants: thrombomodulin, protein C, TFPI
- Increased PAI-1 → impaired fibrinolysis
- NETs (neutrophil extracellular traps) activate both intrinsic and extrinsic coagulation
- Result: fibrin-rich thrombi in small vessels → tissue ischemia, plus consumption of clotting factors → paradoxical bleeding
5. Metabolic abnormalities:
- Insulin resistance + hyperglycemia (TNF, IL-1, stress hormones suppress insulin, promote gluconeogenesis)
- Hyperglycemia suppresses neutrophil bactericidal activity
- Elevated blood glucose, triglycerides, lactate
6. Counter-inflammatory immunosuppression:
- Oscillation between hyperinflammatory and immunosuppressed states
- Shift from Th1 (proinflammatory) to Th2 (anti-inflammatory) cytokines
- IL-10, soluble TNF receptor, IL-1 receptor antagonist
- Lymphocyte apoptosis, cellular anergy
- Clinically: increased susceptibility to secondary infections
7. Organ failure in septic shock:
- Lung: Capillary leak → ARDS (non-cardiogenic pulmonary edema)
- Kidney: Acute tubular necrosis (arteriolar spasm + ischemia)
- Liver: Centrilobular injury → elevated transaminases
- Heart: Direct myocardial depression by TNF-α, IL-1β, and excess NO from iNOS
- Coagulation: DIC in up to 50% of septic patients
8. CARDIOGENIC SHOCK
- Occurs when >40% of myocardium becomes dysfunctional
- Causes: MI (most common), myocarditis, arrhythmia, mechanical complications (papillary muscle rupture → acute MR, VSD), tamponade, PE
- Hemodynamically: low CO, high SVR, high PCWP (pulmonary capillary wedge pressure)
- Differentiating feature: jugular venous distention (JVD) + pulmonary edema (wet + cold patient)
Special features:
- Beck's triad for tamponade: hypotension + JVD + muffled heart sounds
- Kussmaul's sign in tamponade/constrictive pericarditis: JVP rises on inspiration
- Pulsus paradoxus >10 mmHg in tamponade
9. NEUROGENIC SHOCK
- Loss of sympathetic vasomotor tone following spinal cord injury (usually above T6)
- Features: hypotension + relative bradycardia (no compensatory tachycardia because sympathetic drive is lost) + warm, dry skin (vasodilated peripheries)
- Distinguished from hypovolemic shock by: bradycardia (not tachycardia), warm skin
- Treatment: volume replacement first (especially if concomitant hemorrhagic shock), then vasopressors (norepinephrine preferred to maintain SVR)
10. ANAPHYLACTIC SHOCK
- IgE-mediated hypersensitivity → mast cell degranulation → histamine, leukotrienes, prostaglandins
- Massive vasodilation + increased capillary permeability + bronchospasm
- Features: urticaria, angioedema, bronchospasm, hypotension, tachycardia
- Treatment: Epinephrine 0.5 mg IM (1:1000) into anterolateral thigh - first line
11. CLINICAL ASSESSMENT OF SHOCK
11A. History and Clinical Signs
- Vital signs: Tachycardia (earliest sign), hypotension (late), tachypnea
- Skin: Cold, clammy, pale in hypovolemic/cardiogenic; warm, flushed, well-perfused in early distributive/septic
- JVP: Low in hypovolemic/distributive; elevated in cardiogenic/obstructive
- Capillary refill time: >2 seconds suggests hypoperfusion
- Mental status: Confusion/agitation → cerebral hypoperfusion
- Urine output: Most reliable index of vital organ perfusion
- Normal: >1.0 mL/kg/hr
- Reduced: 0.5-1.0 mL/kg/hr
- Severely reduced: <0.5 mL/kg/hr = severe renal hypoperfusion
11B. Diagnostic Features by Shock Type
| Sign | Hypovolemic | Cardiogenic | Distributive | Obstructive |
|---|---|---|---|---|
| JVP | Low | High | Low/normal | High |
| Skin | Cold, clammy | Cold, clammy | Warm, flushed (early septic) | Variable |
| Lung sounds | Clear | Crackles/rales | Variable | Variable |
| HR | High | High | High | High |
| BP | Low | Low | Low | Low |
| Response to fluid | Good | Poor (may worsen) | Good initially | Poor until obstruction relieved |
11C. Laboratory Assessment
- Serum lactate: Most important - level >4 mmol/L = severe shock; target is trending down with treatment
- Base deficit: More negative than -4 mEq/L warrants presumptive diagnosis of shock
- A combination of worsening base deficit + increasing lactate + low urine output = persistent/worsening shock (Rosen's EM)
- CBC: Hematocrit (may be normal acutely in hemorrhage until hemodilution occurs)
- BMP: Creatinine (AKI), glucose, electrolytes
- Coagulation profile: PT/PTT/INR, fibrinogen, D-dimer (for DIC)
- Troponin, BNP/NT-proBNP: For cardiogenic shock
- Blood cultures (2 sets before antibiotics) in suspected septic shock
- Procalcitonin: Elevated in bacterial sepsis
- Arterial blood gas (ABG): Metabolic acidosis (low pH, low HCO₃, elevated lactate)
- Echocardiography (ECHO/POCUS): Bedside ultrasound to assess LV/RV function, pericardial effusion, IVC collapsibility (preload assessment)
11D. Monitoring Parameters
- MAP target: ≥65 mmHg (≥75 mmHg in known hypertensives)
- CVP (Central Venous Pressure): Guides fluid responsiveness (though limited value alone)
- ScvO₂ (Central venous O₂ saturation): <70% suggests inadequate DO₂
- Arterial line: For continuous BP monitoring when vasopressors are used
- Urinary catheter: Hourly urine output measurement
12. MANAGEMENT OF SHOCK - GENERAL PRINCIPLES
ABC Approach
A - Airway: Secure airway; intubate if GCS ≤8, respiratory failure, or anticipated deterioration
B - Breathing: High-flow O₂ (100% via non-rebreather mask), monitor SpO₂; prepare for mechanical ventilation
C - Circulation: IV access (two large-bore peripheral IVs), send bloods, start resuscitation
Fluid Resuscitation
- Initial bolus: 500 mL to 1 L crystalloid (Lactated Ringer's preferred over normal saline - evidence suggests balanced solutions are as good or better)
- Normal saline risks: hyperchloremic metabolic acidosis with large volumes
- For hemorrhagic shock: Balanced transfusion approach - PRBC : FFP : Platelets = 1:1:1 (damage control resuscitation)
- Permissive hypotension (target SBP 80-90 mmHg) until hemorrhage control in penetrating trauma (avoids "popping the clot")
- Avoid excessive crystalloid: "two hits" theory - resuscitation itself can cause ARDS and organ injury through inflammatory cascade
Vasopressors (when adequate fluid resuscitation fails to maintain perfusion)
| Drug | Mechanism | Dose | Indication |
|---|---|---|---|
| Norepinephrine | α₁ > β₁ (↑SVR + ↑CO) | 3-30 μg/min | First-line for septic shock; most types of shock |
| Vasopressin | V1 receptor (vasoconstriction) | 0.01-0.04 units/min | Adjunct to NE in refractory septic shock |
| Epinephrine | α₁ + β₁ + β₂ | 5-20 μg/min | Anaphylaxis (IM); adjunct in septic shock |
| Dopamine | DA > β₁ > α₁ (dose-dependent) | 5-20 μg/kg/min | Second-line (more arrhythmias than NE); avoid in cardiogenic shock |
| Dobutamine | β₁ > β₂ (↑CO, ↓SVR) | 2-15 μg/kg/min | Cardiogenic shock with low CO; septic shock with myocardial depression |
| Phenylephrine | Pure α₁ (↑SVR only) | 2-300 μg/min | Distributive shock; avoid when CO is already low |
(Rosen's EM, Table 127.2; Katzung Pharmacology)
Key point: Norepinephrine is superior to dopamine in both in-hospital and 28-day mortality; dopamine causes more arrhythmias and has worse outcomes in cardiogenic shock. Low-dose dopamine for renal protection is no longer recommended - it does not reduce mortality or decrease dialysis dependence.
13. MANAGEMENT BY SHOCK TYPE
13A. Hemorrhagic/Hypovolemic Shock
- Control bleeding - direct pressure, tourniquet, surgical hemostasis (most important step)
- Damage control resuscitation: PRBC + FFP + Platelets (1:1:1)
- Tranexamic acid (TXA): Give within 3 hours of injury (inhibits fibrinolysis)
- Warm fluids: Prevent hypothermia (hypothermia + acidosis + coagulopathy = "lethal triad")
- Avoid over-resuscitation with crystalloids
- Permissive hypotension in penetrating trauma
13B. Septic Shock (Hour-1 Bundle, Surviving Sepsis Campaign)
- Lactate measurement - remeasure if initial >2 mmol/L
- Blood cultures (2 sets) before antibiotics
- Broad-spectrum antibiotics within 1 hour - early antibiotic administration is the single most impactful intervention
- 30 mL/kg IV crystalloid for hypotension or lactate ≥4 mmol/L
- Vasopressors (norepinephrine first) if MAP <65 mmHg during/after fluid resuscitation
- Source control - drain abscess, remove infected device
- Steroids: Hydrocortisone 200 mg/day IV if vasopressor requirement persists
- Tight glycemic control (target glucose 140-180 mg/dL)
- DVT prophylaxis, stress ulcer prophylaxis
13C. Cardiogenic Shock
- Identify and treat cause: Emergent PCI for AMI, cardioversion for arrhythmia, pericardiocentesis for tamponade
- Inotropes: Dobutamine (first line - improves contractility without major vasoconstriction)
- Vasopressors: Norepinephrine for hypotension
- DO NOT give large fluid boluses (worsens pulmonary edema)
- Mechanical circulatory support: IABP (intra-aortic balloon pump), Impella, ECMO in refractory cases
- Avoid dopamine in cardiogenic shock (increased mortality)
13D. Obstructive Shock
- Tension pneumothorax: Needle decompression (2nd ICS, MCL) → chest drain
- Cardiac tamponade: Pericardiocentesis (needle aspiration) → pericardial window if recurrent
- Massive PE: Anticoagulation, thrombolytics (if cardiac arrest or hemodynamic compromise), surgical embolectomy
13E. Anaphylactic Shock
- Epinephrine 0.5 mg IM (1:1000) into anterolateral thigh - immediately
- IV fluids (aggressive resuscitation - up to 4-8 L may be needed)
- H1 antihistamine (diphenhydramine/chlorphenamine)
- H2 antihistamine (ranitidine/famotidine)
- Corticosteroids (prevent biphasic reaction)
- Salbutamol for bronchospasm
- Remove/avoid trigger
14. MORPHOLOGICAL CHANGES IN ORGANS (Pathology)
(Robbins & Cotran Pathologic Basis of Disease)
Kidneys
- Acute tubular necrosis (ATN) - most consistent finding
- Arteriolar spasm → cortical ischemia → tubular cell death
- Clinically: oliguria → anuria → rising creatinine
- May progress to AKI requiring dialysis
Lungs
- ARDS (Acute Respiratory Distress Syndrome) - "shock lung"
- Mechanism: Capillary leak → protein-rich alveolar edema → impaired gas exchange
- CXR: bilateral diffuse infiltrates ("white out")
- Requires mechanical ventilation with lung-protective strategy (low tidal volumes)
Adrenal Glands
- Lipid depletion of cortical cells (stressed adrenals use up stored cholesterol)
- In severe/prolonged shock: adrenal cortical insufficiency (relative adrenal insufficiency)
- Rationale for hydrocortisone in refractory septic shock
Liver
- Centrilobular (zone 3) necrosis - center of lobule is most oxygen-dependent
- Elevated transaminases (ALT, AST) in shock
- Impaired synthetic function (coagulopathy), impaired lactate clearance
GI Tract
- Ischemic enterocolitis - mucosal ulceration
- Loss of gut barrier function → bacterial translocation → feeds septic cycle
- "Gut" is the motor of MOF (multiple organ failure)
Brain
- Ischemic encephalopathy - watershed area infarcts (between ACA/MCA and MCA/PCA territories)
- Clinically: confusion, agitation, coma
Heart
- Contraction band necrosis - characteristic of catecholamine-mediated injury
- Subendocardial ischemia (most vulnerable region)
15. MULTI-ORGAN FAILURE (MOF)
The end stage of progressive, uncompensated shock:
- Sequential or simultaneous failure of ≥2 organ systems
- Order of typical failure: Lungs (ARDS) → Kidneys (ATN/AKI) → Liver → Coagulation (DIC) → CNS → Heart
- Mortality increases with number of organs failing: 1 organ ~30%, 3 organs >80%, 5 organs ~100%
- Pathogenesis: Ischemia-reperfusion injury + systemic inflammation + microvascular thrombosis + immunosuppression
16. SPECIAL SITUATIONS
The "Lethal Triad" of Trauma
Hypothermia + Acidosis + Coagulopathy - each worsens the others in a vicious cycle; all three must be corrected simultaneously in hemorrhagic shock management.
Permissive Hypotension
In penetrating trauma with uncontrolled hemorrhage, targeting SBP of 80-90 mmHg (rather than normal) avoids "popping the clot" and diluting clotting factors before surgical hemostasis. Not appropriate in head trauma (brain needs higher MAP).
Obstructive vs Cardiogenic
Both have elevated JVP and low CO. Key differences: obstructive shock responds to removing the obstruction; cardiogenic requires addressing cardiac function.
Children in Shock
Greater body water composition → better compensation → only tachycardia until sudden decompensation. Normal systolic BP in a child does NOT rule out significant hemorrhage.
Elderly in Shock
Beta-blockers blunt tachycardia; patients on ACE inhibitors have blunted RAAS response; baseline reduced cardiac reserve means decompensation occurs earlier at lower blood loss.
17. QUICK REVISION - HIGH-YIELD POINTS FOR EXAMS
- Definition: Shock = inadequate tissue perfusion leading to cellular hypoxia
- Earliest sign of shock: Tachycardia (not hypotension)
- Best early laboratory marker: Serum lactate (>4 mmol/L = severe shock)
- Urine output normal: >1 mL/kg/hr; severe hypoperfusion: <0.5 mL/kg/hr
- ATLS Class III shock = BP falls (30-40% blood loss) - before this, BP is maintained by compensation
- Pulse pressure narrows before systolic BP falls (early sign of hemorrhagic shock)
- Neurogenic shock: Hypotension + bradycardia + warm skin (unlike other types)
- Septic shock first-line vasopressor: Norepinephrine (superior to dopamine)
- Cardiogenic shock: DO NOT give fluids; dobutamine (inotrope) is key
- Anaphylaxis: Epinephrine IM (not IV initially, not subcutaneous)
- Surviving Sepsis Campaign - Hour 1 Bundle: Lactate, blood cultures, antibiotics, fluids, vasopressors
- DIC occurs in up to 50% of septic shock patients
- Organ most sensitive to ischemia in shock: Kidney (ATN) and brain
- "Shock lung" = ARDS - bilateral infiltrates, non-cardiogenic pulmonary edema
- Lethal triad in trauma: Hypothermia + Acidosis + Coagulopathy
- Irreversible shock: Lysosomal enzyme release + ischemic bowel → endotoxin absorption
- Base deficit more negative than -4 mEq/L = presumptive shock diagnosis
- Compensatory mechanisms timed: Catecholamines (seconds to minutes) → RAAS/ADH (10-60 min) → volume redistribution (1-48 hours)
- Low-dose dopamine for renal protection is NOT recommended (no mortality benefit)
- Hydrocortisone (200 mg/day) in septic shock if vasopressors are still required despite adequate resuscitation
REFERENCES
- Robbins, Cotran & Kumar Pathologic Basis of Disease, 10th ed., p. 134-137
- Guyton & Hall Textbook of Medical Physiology, p. 299-306
- Rosen's Emergency Medicine, 9th ed., Chapter 3
- Sabiston Textbook of Surgery, Chapter 33
- Tintinalli's Emergency Medicine, Chapter 20
- Katzung Basic and Clinical Pharmacology, 16th ed.
This is a shared conversation. Sign in to Orris to start your own chat.