Arethrosclerosis
Reading File
Finding Sources
Searching PubMed
"atherosclerosis"[MeSH Terms] AND "pathogenesis"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of Atherosclerosis, drawn from Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease.
Atherosclerosis
Definition
Atherosclerosis is a chronic inflammatory disease of the arterial wall best understood as the vascular response to endothelial injury (the "response to injury" hypothesis). It is characterized by intimal lesions called atheromas (atherosclerotic plaques) - raised lesions composed of a soft, friable lipid core (mainly cholesterol and cholesterol esters with necrotic debris) covered by a fibrous cap. It underlies the pathogenesis of coronary, cerebral, and peripheral vascular disease, causing roughly half of all deaths in the Western world.
- Robbins & Kumar Basic Pathology, p. 314
Epidemiology
Although atherosclerosis is nearly universal in high-resource nations, risk reduction and improved therapies have sharply decreased morbidity and mortality over recent decades. However, the adoption of Western diets and lifestyles in lower-resource nations has increased the burden of ischemic heart disease globally. Death rates for coronary artery disease in Africa, India, and Southeast Asia now exceed those in the United States; Eastern European countries have rates 3-5 times higher than the US and 7-12 times higher than Japan.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 465
Risk Factors
| Category | Factors |
|---|---|
| Nonmodifiable | Genetic variation, family history, increasing age, male sex |
| Modifiable | Hyperlipidemia (high LDL, low HDL), hypertension, cigarette smoking, diabetes mellitus, obesity, physical inactivity |
| Novel/Emerging | Elevated CRP, hyperhomocysteinemia, lipoprotein(a), metabolic syndrome |
Roughly 20% of cardiovascular events occur in the absence of identifiable risk factors.
Family history is the single most important independent risk factor. The predisposition is usually polygenic, related to cumulative effects of many shared alleles.
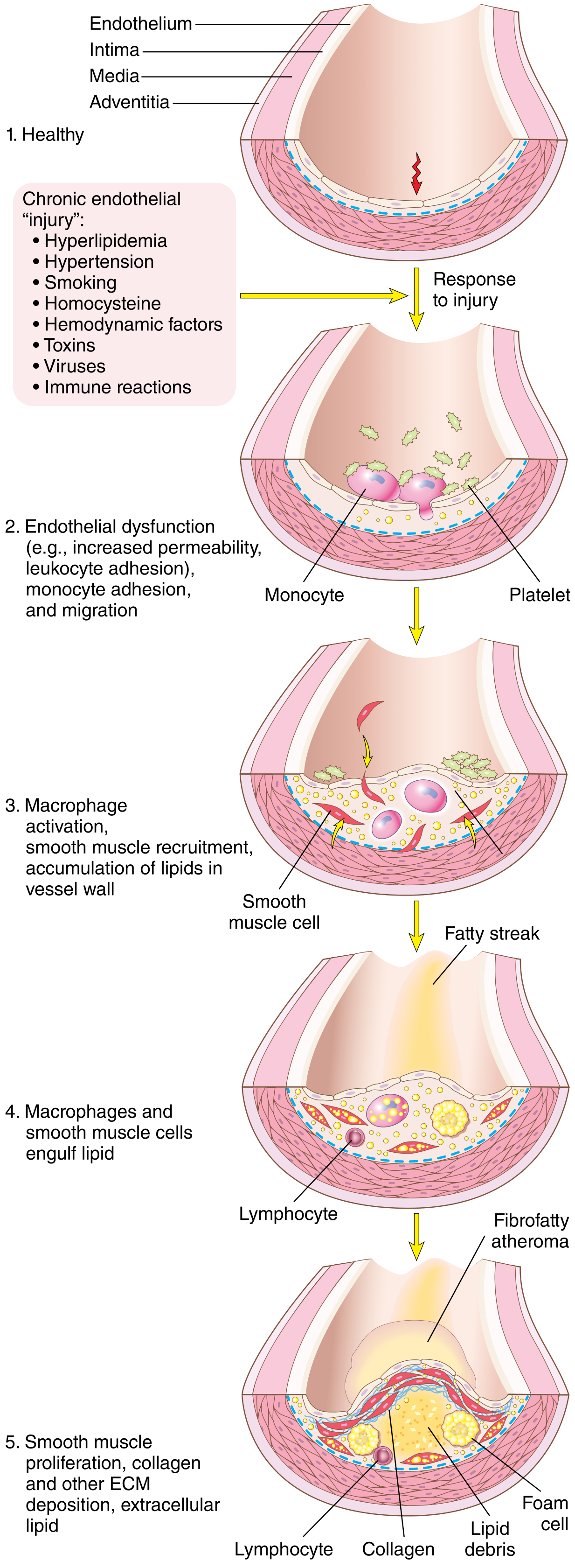
Pathogenesis
The central model involves a cascade of events triggered by endothelial injury:
- Endothelial cell (EC) injury - increased permeability, leukocyte adhesion, altered gene expression
- Lipoprotein accumulation in the vessel wall (especially oxidized LDL and cholesterol crystals)
- Monocyte adhesion to the endothelium, migration into the intima, and transformation into macrophages and foam cells
- Platelet adhesion
- Smooth muscle cell (SMC) recruitment from the media, with proliferation and ECM production
- T-cell recruitment
- Lipid accumulation extracellularly and within macrophages and SMCs
- Calcification of ECM and necrotic debris (late stage)
Key Mechanisms
Hemodynamic disturbances: Plaques form preferentially at branch points, ostia of vessels, and the posterior abdominal aorta - sites of turbulent, non-laminar flow. Laminar flow upregulates the transcription factor KLF2 (Kruppel-like factor-2), which promotes atheroprotective gene expression. Turbulent flow reverses this effect. Notably, some protective effects of statins also work via KLF2 upregulation.
Hypercholesterolemia: Elevated LDL is the dominant lipid risk factor. LDL that enters the vessel wall undergoes oxidative modification to oxidized LDL (oxLDL), which is:
- Taken up by macrophages via scavenger receptors, forming foam cells
- Directly cytotoxic to endothelial cells and SMCs
- A stimulus for local inflammatory cytokine production
- Chemotactic for additional monocytes
HDL acts protectively by "reverse cholesterol transport" - removing cholesterol from vessel walls.
Inflammation: Chronic low-grade inflammation is fundamental. Inflammatory cytokines (especially TNF) stimulate proatherogenic patterns of EC gene expression.
Morphology of Plaques
Fatty Streak (Early Lesion)
- Flat or slightly raised yellow intimal lesion
- Composed of lipid-laden macrophages (foam cells) and some intimal SMCs
- Appear in the aorta of children as young as 1 year; coronary arteries by age 10
- Not all progress to full plaques
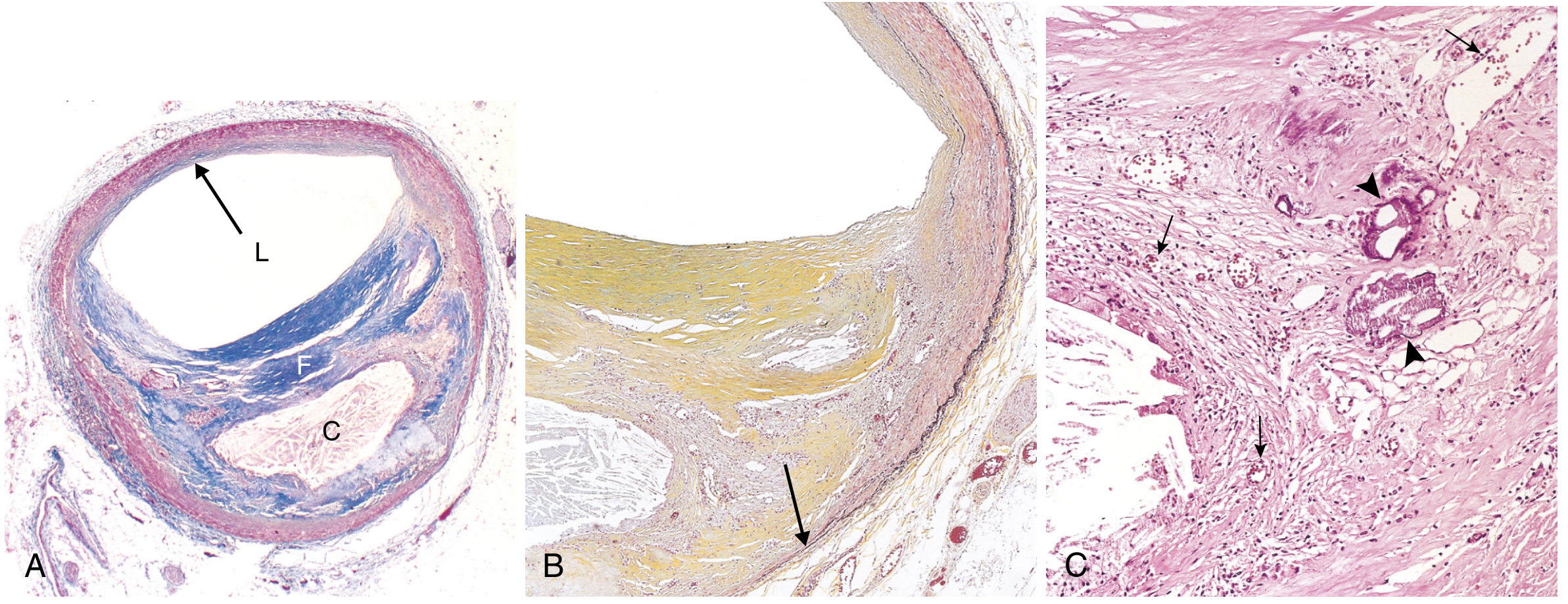
Fibrous Plaque (Advanced Lesion)
- Fibrous cap: collagen, SMCs, and scattered inflammatory cells
- Necrotic core: lipid debris, cholesterol crystals, foam cells, dead cells
- Shoulder regions: more cellular, with macrophages, T cells, and SMCs (most vulnerable area)
- Neovascularization from the vasa vasorum penetrates the base of the plaque
Clinical Consequences
1. Atherosclerotic Stenosis
- Gradual progressive luminal narrowing
- Symptoms appear when stenosis reaches approximately 70% occlusion in coronary arteries
- Causes stable angina (chest pain on exertion), bowel ischemia, intermittent claudication, and chronic ischemic encephalopathy
2. Acute Plaque Change (Most Dangerous)
Plaque changes fall into three categories:
- Rupture/ulceration/erosion of the fibrous cap - exposes thrombogenic substances, triggers acute thrombus formation
- Hemorrhage into the plaque - raptures overlying cap or intimal neovessels, expanding the plaque suddenly
- Vasospasm - induced by platelet aggregation products (thromboxane A2, serotonin)
Plaque rupture is the proximate cause of most acute coronary syndromes (unstable angina, NSTEMI, STEMI) and many strokes.
3. Aneurysm Formation
- Ischemia-induced atrophy of the media (pressure or diffusion barrier) with loss of elastic tissue
- Wall weakening leads to aneurysmal dilation and potential rupture
- Most common in the infrarenal abdominal aorta
4. Major Affected Sites and Clinical Manifestations
| Affected Vessel | Clinical Result |
|---|---|
| Coronary arteries | Myocardial infarction, stable angina, sudden cardiac death |
| Cerebral/carotid arteries | Stroke, TIA |
| Aorta | Abdominal aortic aneurysm |
| Peripheral (iliac, femoral, popliteal) | Peripheral artery disease, gangrene |
| Renal arteries | Renovascular hypertension, renal ischemia |
| Mesenteric arteries | Bowel ischemia |
Prevention and Management Principles
- Lipid lowering: Statins are the cornerstone; they lower LDL and have anti-inflammatory effects (partly via KLF2)
- Antihypertensives: Reduce endothelial shear stress and hemodynamic injury
- Antiplatelet agents: Aspirin reduces thrombotic complications
- Lifestyle: Smoking cessation, exercise, dietary modification
- Glycemic control: In diabetics reduces microvascular and macrovascular risk
- Emerging therapies: PCSK9 inhibitors for severe hypercholesterolemia, anti-inflammatory approaches (colchicine)
Sources: Robbins & Kumar Basic Pathology 10e, pp. 314-320; Robbins, Cotran & Kumar Pathologic Basis of Disease 10e, pp. 465-474
This is a shared conversation. Sign in to Orris to start your own chat.