Micturation reflex from guyton and halls
Micturition
- Progressive bladder filling until wall tension rises above a threshold
- A nervous reflex - the micturition reflex - that empties the bladder or creates a conscious urge to urinate
Physiological Anatomy
- The bladder consists of a body (collects urine) and a neck (funnel-shaped, connects to the urethra)
- The smooth muscle is the detrusor muscle - its fibers extend in all directions and, when contracted, raise bladder pressure to 40-60 mm Hg. Muscle cells are electrically fused, so an action potential spreads through the entire bladder at once
- The trigone is a triangular area on the posterior wall above the bladder neck; its mucosa is smooth (no rugae)
- The internal sphincter (in the bladder neck) maintains tonic tone to keep the posterior urethra empty until pressure exceeds a critical threshold
- The external sphincter passes through the urogenital diaphragm - it is voluntary skeletal muscle, controlled by the pudendal nerve
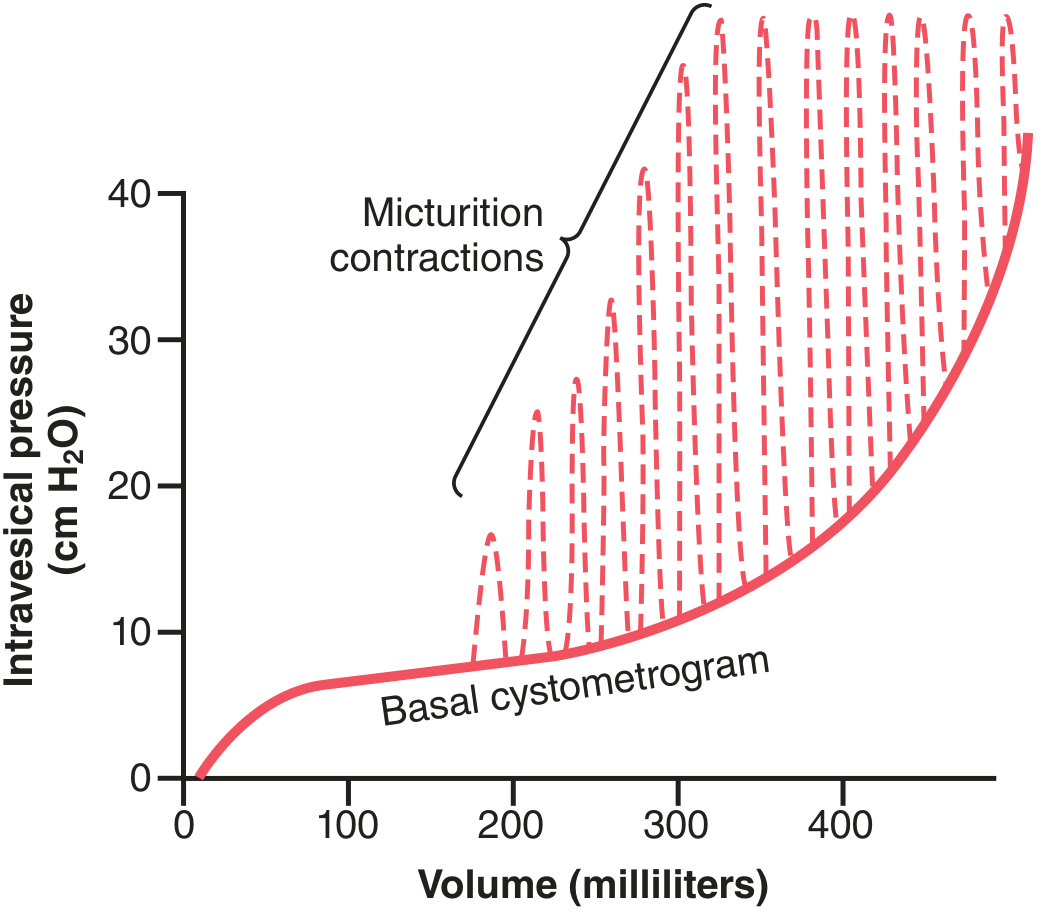
Cystometrogram and Pressure Changes
- 0-50 mL: pressure rises slightly
- 50-300 mL: pressure stays nearly constant (stress relaxation of the detrusor)
- >300-400 mL: pressure rises rapidly
The Micturition Reflex
- Sensory signals travel via pelvic nerves to the sacral segments of the spinal cord
- Reflexively back to the bladder via parasympathetic fibers through the same pelvic nerves
- Initial bladder contraction activates more stretch receptors → more sensory impulses → stronger reflex contraction → repeat
- This cycle builds progressively until the bladder contracts strongly
- After seconds to >1 minute, the reflex fatigues and the cycle ceases, allowing the bladder to relax
- Progressive, rapid increase in pressure
- A period of sustained pressure
- Return of pressure to basal tone
External Sphincter Inhibition
Higher Center Control
- They keep the reflex partially inhibited except when micturition is desired
- They can prevent voiding by tonic contraction of the external sphincter, even during an active reflex
- They can facilitate the sacral micturition centers when it is time to urinate, while simultaneously inhibiting the external sphincter
Abnormalities of Micturition
| Condition | Cause | Mechanism | Result |
|---|---|---|---|
| Atonic Bladder / Overflow Incontinence | Destruction of sensory nerve fibers (e.g., sacral crush injury, tabes dorsalis) | No stretch signals reach the cord; efferent fibers intact | Bladder fills to capacity, overflows drop by drop |
| Automatic Bladder | Spinal cord damage above the sacral region (sacral cord intact) | Micturition reflexes still occur but are uncontrolled by the brain; initially suppressed (spinal shock), then return | Periodic, unannounced bladder emptying |
| Uninhibited Neurogenic Bladder | Partial damage to spinal cord or brain stem interrupting inhibitory signals | Facilitative impulses keep sacral centers overexcitable; even small urine volumes trigger reflex | Frequent, relatively uncontrollable micturition |
Create a detailed diagram comparing normal vs. abnormal micturition reflexes
A detailed medical educational diagram comparing normal vs abnormal micturition reflexes. The diagram is divided into 4 panels arranged in a 2x2 grid on a clean white background with clear section headers. Panel 1 (top-left) - "NORMAL MICTURITION REFLEX": Shows a flowchart with anatomical labels. Bladder filling → stretch receptors in posterior urethra activate → pelvic nerves carry signals to sacral cord (S2-S4) → parasympathetic signals return via pelvic nerves → detrusor muscle contracts → pudendal nerve inhibits external sphincter → voiding occurs. Include a small cystometrogram curve showing normal basal pressure with dashed micturition spikes appearing around 200-300mL. Higher centers (cortex/brainstem) shown with bidirectional arrows indicating inhibition and facilitation. Color: green accents for normal pathway. Panel 2 (top-right) - "ATONIC BLADDER (Overflow Incontinence)": Shows the same arc but with a red X cutting the sensory/afferent limb. Label: "Sensory nerve fibers destroyed (e.g., sacral crush injury, tabes dorsalis)". Bladder shown greatly distended. Arrow showing urine dribbling out (overflow). Cystometrogram inset showing steadily rising pressure with NO reflex spikes, then overflow. Text labels: "No stretch signal reaches cord", "Efferent fibers intact but useless", "Bladder fills to capacity → overflow drop by drop". Red color scheme. Panel 3 (bottom-left) - "AUTOMATIC BLADDER (Cord Damage Above Sacral)": Shows spinal cord with a lesion above the sacral region (T1-L2 level marked with red damage symbol). Sacral cord (S2-S4) shown intact below. Arrows: micturition reflex arc intact at sacral level but disconnected from brain. Phase labels: "Phase 1 - Spinal shock: reflex suppressed (days to weeks)" and "Phase 2 - Reflex returns: unannounced periodic voiding". Cystometrogram inset showing initial flat line then return of reflex spikes. Orange color scheme. Panel 4 (bottom-right) - "UNINHIBITED NEUROGENIC BLADDER (Partial Brain/Cord Damage)": Shows partial damage to inhibitory pathways in spinal cord or brainstem (dashed broken lines from cortex). Facilitatory impulses shown as strong arrows overwhelming the system. Bladder shown contracting at very low fill volumes (~100-150mL). Cystometrogram inset showing reflex spikes starting very early and at high frequency even at low volumes. Label: "Inhibitory signals interrupted → sacral centers overexcitable → small volumes trigger reflex → frequent/urgent/uncontrollable micturition". Purple color scheme. At the bottom, a comparison table with rows: Lesion site | Afferent intact? | Efferent intact? | Higher control? | Clinical result — filled in for each of the 4 conditions. Overall style: clean medical textbook illustration, anatomical accuracy, color-coded pathways (green=normal, red=atonic, orange=automatic, purple=uninhibited), clear sans-serif labels, professional medical education quality.