AKI on CKD
Reading File
Finding Sources
Finding Sources
Searching PubMed
"acute kidney injury" AND "chronic kidney disease" AND "AKI on CKD"
Finding Sources
Searching PubMed
"acute kidney injury" AND "chronic kidney disease" AND progression
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to write a thorough answer. Let me compile everything.
AKI on CKD (Acute Kidney Injury Superimposed on Chronic Kidney Disease)
Definition and Conceptual Framework
AKI on CKD (also called "acute on chronic kidney injury") is the superimposition of AKI on pre-existing CKD. Baseline kidney function is already impaired, and an acute insult causes an additional, potentially reversible decrement in GFR. The relationship between AKI and CKD is bidirectional and self-reinforcing - CKD strongly predisposes to AKI, and AKI accelerates CKD progression toward ESRD:
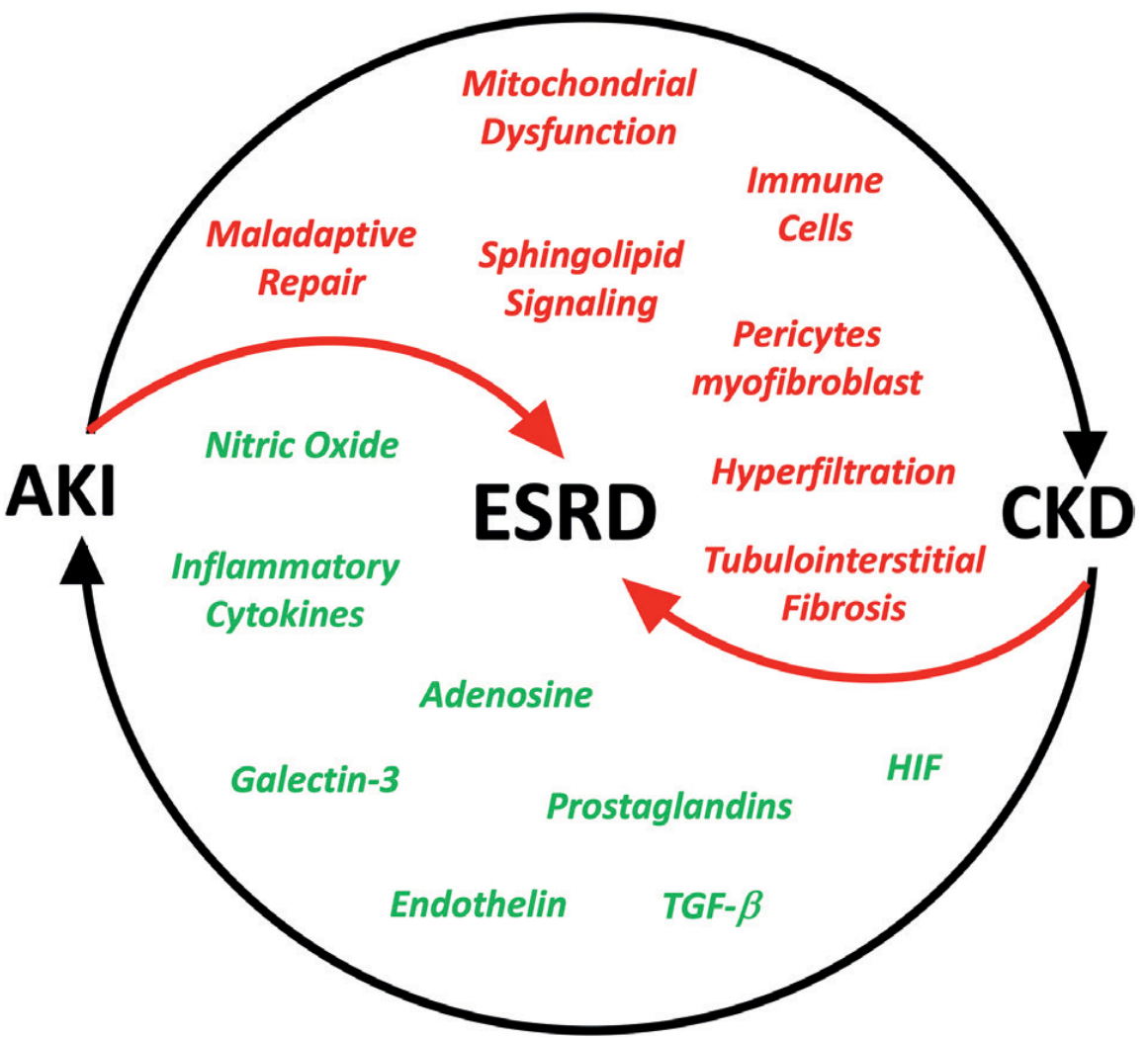
Fig. 28.12 - AKI to CKD to ESRD vicious cycle. Red arrows = maladaptive/profibrotic mechanisms; Green arrows = traditional mediators. (Brenner and Rector's The Kidney, 7th Ed.)
Why CKD Increases Susceptibility to AKI
CKD is one of the most important risk factors for developing AKI. Multiple mechanisms operate simultaneously:
| Mechanism | Consequence |
|---|---|
| Diminished renal functional reserve | Less capacity to tolerate further nephron loss |
| Impaired salt/water conservation | Predisposes to intravascular volume contraction |
| Decreased detoxification | Greater susceptibility to cytotoxic injury |
| Impaired nephrotoxin clearance | Prolonged exposure to drugs/toxins |
| Macrovascular and microvascular disease | Increased ischemic injury risk |
| Older age + comorbidity accumulation | Reduced autoregulation capacity |
- Brenner and Rector's The Kidney, block 16, line 1974
- Comprehensive Clinical Nephrology, 7th Edition, block 10, line 2621
Common precipitants in CKD patients include: NSAIDs, RAS inhibitors (with volume depletion), iodinated radiocontrast, aminoglycosides, excessive diuresis, GI fluid losses, heart failure decompensation, sepsis, and obstruction.
Epidemiology and Prognosis
AKI on CKD carries a substantially worse prognosis than either condition alone - it has a multiplicative (not simply additive) effect on ESRD risk.
-
Among 233,803 Medicare beneficiaries, AKI on a background of CKD carried an HR of 41.2 (95% CI 34.6-49.1) for developing ESKD vs. 13.0 without pre-existing CKD.
-
In patients with eGFR 30-44 mL/min/1.73 m² who needed dialysis for AKI, 42% developed ESKD within 30 days of discharge; for eGFR 15-29, this rose to 63% - compared to only 1.5% in CKD patients without AKI.
-
At 6 months post-discharge, patients with CKD + AKI had ESKD/death rates of 12.7%/19.7% vs. 1.7%/7.4% in CKD-only comparators (adjusted HR 1.30).
-
A meta-analysis of 13 cohort studies: pooled HR for new CKD after AKI = 8.8 (95% CI 3.1-25.5); pooled HR for ESKD = 3.1 (95% CI 1.9-5.0).
-
72.1% of patients with AKI and no pre-existing CKD developed CKD within 2 years; 25.2% of all ESKD cases had a prior AKI episode.
-
Brenner and Rector's The Kidney, block 12, lines 1291-1299
Recent evidence update (2025): Veltkamp et al. (Nephrol Dial Transplant, 2025) - systematic review confirming long-term risks of adverse kidney outcomes after AKI [PMID: 40424522].
Distinguishing AKI from CKD (and Identifying the Acute Component)
This is often a major clinical challenge. Key differentiating features:
| Feature | Suggests CKD | Suggests AKI or AKI on CKD |
|---|---|---|
| Prior creatinine values | Elevated baseline | Rising trend from known baseline |
| Kidney size (US) | Small, echogenic (atrophied) | Normal size (but some CKD causes have normal/enlarged kidneys: DM nephropathy, amyloid, HIV nephropathy, PCKD) |
| Anemia | Normocytic (EPO deficiency) | Usually absent unless pre-existing CKD |
| Hyperparathyroidism | Present | Absent |
| Peripheral neuropathy | Chronic feature | Not expected acutely |
| Urinary sediment | Broad waxy casts | Granular/muddy casts (ATN), RBC casts (GN) |
| Rate of rise of creatinine | Gradual | Rapid (days-weeks) |
Knowledge of prior serum creatinine concentrations is essential to quantify the reversible AKI component. Ultrasound is the most helpful initial imaging study - small echogenic kidneys indicate CKD but acute reversible components must still be actively sought. Normal-sized kidneys require more extensive evaluation.
- Comprehensive Clinical Nephrology, 7th Ed., lines 2197-2199 and 2156-2168
Pathophysiology of AKI-to-CKD Transition
After an AKI episode, multiple maladaptive mechanisms drive CKD progression:
- Nephron loss - irreversible tubular cell death reduces functional nephron mass
- Peritubular capillary rarefaction / vascular dropout - micro-CT studies show up to 45% reduction in vascular density at 4 weeks post-ischemia; reduced VEGF with upregulated ADAMTS1 impairs angiogenesis; hypoxia drives progressive fibrosis
- Cell cycle arrest and senescence - repetitive injury upregulates CDK inhibitors (p16^Ink4, p53-p21^Cip1/Waf1); senescent cells secrete TGF-β, cytokines, proteases promoting fibrosis ("senescence-associated secretory phenotype")
- Pericyte and myofibroblast activation - pericytes detach from capillaries and transition to interstitial myofibroblasts, producing collagen
- Sustained oxidative stress - post-AKI kidneys show persistent Ang II hypersensitivity via NADPH oxidase pathways (attenuated by apocynin); oxidant stress promotes a profibrotic response to Ang II
- Maladaptive tubular repair - incomplete re-differentiation, chronic KIM-1 expression becomes pro-inflammatory rather than protective
- Inflammation - persistent immune cell activation, cytokine production (TGF-β, IL-6), sphingolipid signaling
- Hyperfiltration - remaining nephrons undergo compensatory hyperfiltration, accelerating glomerular sclerosis
- Brenner and Rector's The Kidney, block 16, lines 129-200 (AKI-CKD transition mechanisms)
Management of AKI on CKD
Identify and Treat Precipitants
- Correct volume depletion (cautious fluid resuscitation given reduced reserve)
- Relieve obstruction (always exclude obstructive uropathy)
- Hold nephrotoxins: NSAIDs, aminoglycosides, contrast (use lowest dose, hydrate first)
- Consider relapse of underlying disease vs. superimposed AIN, renal vein thrombosis, or obstruction
- Withhold ACEi/ARB temporarily during acute illness, restart when stable
Supportive Care
- Fluid management - avoid both volume depletion and overload; titrate to euvolemia
- Electrolyte monitoring - CKD patients have less reserve against hyperkalemia and metabolic acidosis; more rapid decompensation expected
- Nutrition - maintain adequate protein and caloric intake; adjust for renal function
- Drug dosing - adjust all renally cleared drugs to eGFR level
Renal Replacement Therapy (RRT)
- Indications: refractory hyperkalemia, refractory acidosis, uremic symptoms, volume overload unresponsive to diuretics, symptomatic uremia
- In CKD patients with preadmission eGFR < 30, dialysis non-recovery is common - early nephrology involvement and long-term KRT planning is essential
- KDIGO recommends initiating dialysis based on clinical signs/symptoms rather than a specific GFR threshold
Post-AKI Follow-up (critical in CKD patients)
-
Review at 3 months post-AKI to reassess eGFR, proteinuria, and BP
-
Intensify CKD management: RAS blockade for proteinuria, BP control (target <130/80 in most guidelines), SGLT2 inhibitors (strong recent evidence for cardiorenal protection - JAMA meta-analysis 2026)
-
Avoid further AKI insults - educate patients on sick-day rules (hold ACEi/ARB/diuretics with GI illness)
-
Assess for ESRD trajectory and plan pre-emptive KRT if eGFR trending toward <15
-
Comprehensive Clinical Nephrology, 7th Ed., block 11, lines 3897-3914
Key Points Summary
| Domain | Key Fact |
|---|---|
| Definition | AKI (acute rise in creatinine/fall in urine output) superimposed on pre-existing CKD |
| KDIGO AKI staging | Stage 1: Cr ×1.5 or +0.3 mg/dL in 48h; Stage 2: Cr ×2; Stage 3: Cr ×3 or need for RRT |
| Risk amplification | CKD × AKI = HR 41.2 for ESKD vs. CKD without AKI |
| Most dangerous group | eGFR 15-29 + dialysis-requiring AKI → 63% ESKD within 30 days |
| Transition mechanisms | Vascular dropout, cell senescence, TGF-β fibrosis, Ang II hypersensitivity, hyperfiltration |
| Priority in management | Treat precipitant, hold nephrotoxins, avoid fluid extremes, plan for KRT if non-recovery likely |
| New evidence | SGLT2i reduce kidney disease progression regardless of albuminuria level (JAMA 2026) |
Sources: Brenner and Rector's The Kidney, 2-Volume Set; Comprehensive Clinical Nephrology, 7th Edition; National Kidney Foundation Primer on Kidney Diseases, 8e.
CKD staging
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
I now have all the information needed. Let me compile a comprehensive, well-structured answer.
CKD Staging - KDIGO 2012 CGA Classification
Definition of CKD
CKD is defined as abnormalities of kidney structure or function, present for >3 months, with implications for health. Diagnosis requires either:
- Functional criterion: GFR < 60 mL/min/1.73 m²
- Structural criterion (markers of kidney damage): albuminuria (UACR ≥30 mg/g), urine sediment abnormalities (hematuria, RBC/WBC casts), electrolyte/tubular disorders, histologic abnormalities, structural abnormalities on imaging, or history of kidney transplantation
The 3-month duration distinguishes CKD from AKI. The diagnosis does not require both functional and structural criteria - either alone is sufficient.
The CGA Staging System (KDIGO 2012)
The current KDIGO 2012 framework classifies CKD by three dimensions: Cause (C), GFR category (G), Albuminuria category (A) - collectively "CGA staging."
Example: A patient with IgA nephropathy, eGFR 34, UACR 367 mg/g is staged as "IgA nephropathy, G3b A3"
The original 2002 NKF-KDOQI system used GFR alone. KDIGO 2012 added albuminuria because epidemiologic data showed that both GFR and albuminuria are independent graded risk factors for CKD progression, cardiovascular events, and mortality. The combination of the two provides far better risk stratification.
GFR Categories (G Stages)
| Stage | eGFR (mL/min/1.73 m²) | Description | Clinical Action |
|---|---|---|---|
| G1 | ≥90 | Normal or high | Diagnose & treat cause; reduce CVD risk; start measures to slow progression |
| G2 | 60-89 | Mildly decreased | Estimate progression rate |
| G3a | 45-59 | Mildly to moderately decreased | Adjust drug dosages |
| G3b | 30-44 | Moderately to severely decreased | Evaluate and treat complications |
| G4 | 15-29 | Severely decreased | Prepare for KRT (transplant and/or dialysis) |
| G5 | <15 | Kidney failure | Initiate KRT if uremia present OR continue conservative management |
Note: G5D = dialysis-treated; G5T = transplant recipient. G1 and G2 alone do not qualify as CKD unless accompanied by markers of kidney damage.
The subdivision of stage 3 into 3a and 3b was introduced by NICE in 2008 (adopted into KDIGO 2012) because these groups have clinically important differences in complication burden, risk profile, and management needs.
Albuminuria Categories (A Stages)
| Category | Albumin Excretion Rate (mg/day) | UACR (mg/g) | UACR (mg/mmol) | Description |
|---|---|---|---|---|
| A1 | <30 | <30 | <3 | Normal to mildly increased |
| A2 | 30-299 | 30-299 | 3-30 | Moderately increased (old term: microalbuminuria) |
| A3 | ≥300 | ≥300 | >30 | Severely increased (old term: macroalbuminuria/proteinuria) |
Key actions: A2 triggers RAS blocker therapy + lower BP target; A3 triggers treatment of nephrotic syndrome if present.
KDIGO Heat Map - Prognosis by GFR + Albuminuria
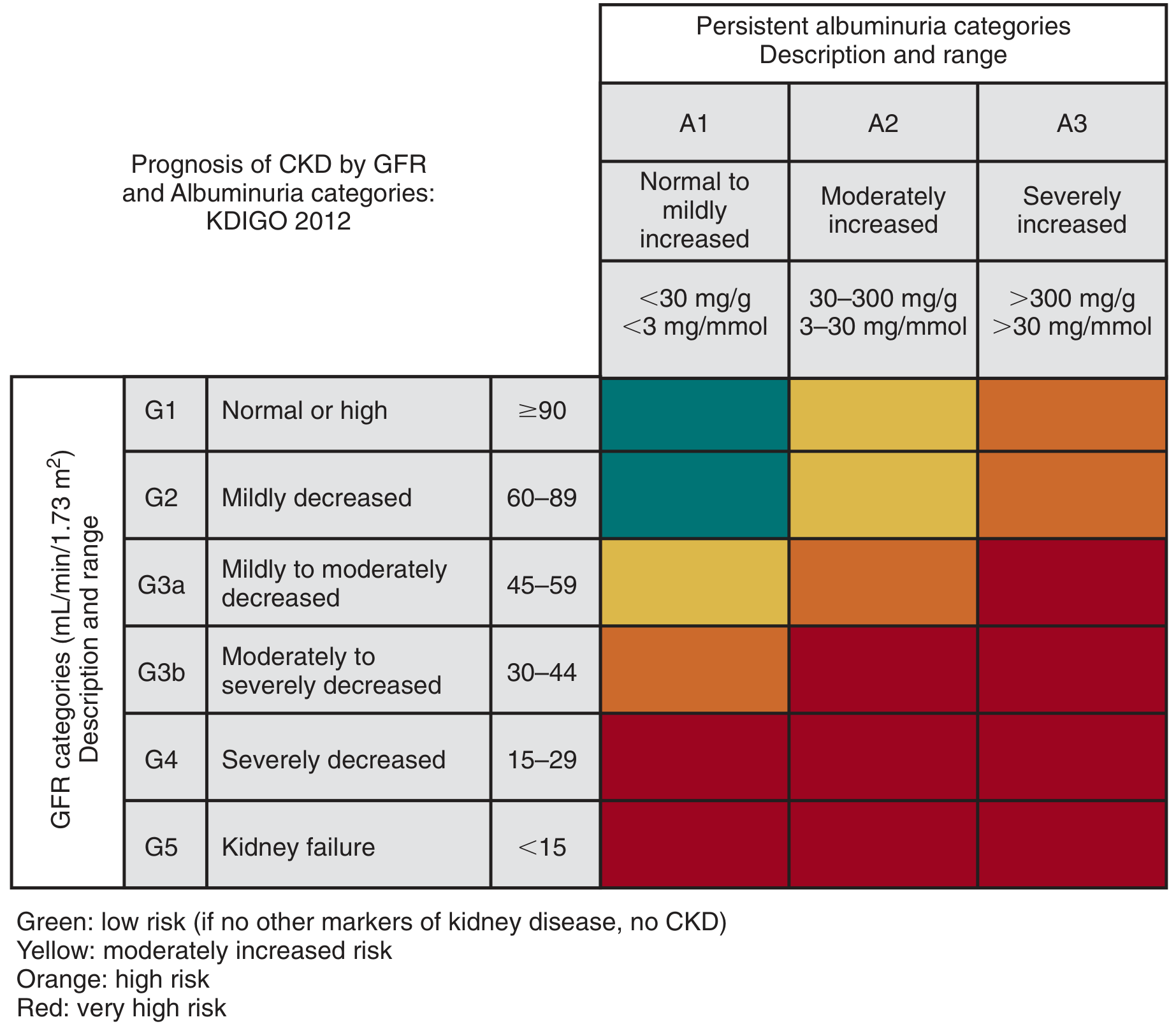
Colour coding:
- Green (G1-G2, A1): Low risk - if no other markers of kidney disease, does not qualify as CKD
- Yellow (G1-G2, A2; G3a, A1): Moderately increased risk
- Orange (G1-G2, A3; G3a, A2; G3b, A1): High risk
- Red (G3a, A3; G3b, A2-A3; G4, A1-A3; G5, A1-A3): Very high risk
Complications by Stage
| Stage | Key Complications / Issues |
|---|---|
| G1-G2 | Usually asymptomatic; focus on treating underlying cause and CVD risk reduction |
| G3a-G3b | Anemia (EPO deficiency), early metabolic acidosis, CKD-MBD begins, neuropathy, nutrition assessment |
| G4 | All above + hyperphosphatemia, hyperparathyroidism, hyperkalemia, fluid overload, accelerated CVD; prepare for KRT |
| G5 | Uremia, pericarditis, encephalopathy, severe metabolic derangements; initiate KRT or conservative management |
In stage 3 CKD, assess for anemia, neuropathy, nutrition, and bone-mineral metabolism. Patients with GFR <30 (G3b and below) should be referred to a nephrologist. Stage 4 patients should be proactively prepared for dialysis or transplantation.
- Textbook of Family Medicine, 9e, line 205
Cause Classification (C)
Causes are classified by:
- Presence or absence of systemic disease (primary vs. secondary nephropathy)
- Location of pathologic lesion within the kidney:
- Glomerular (e.g., IgA nephropathy, diabetic nephropathy, lupus nephritis)
- Tubulointerstitial (e.g., pyelonephritis, drug-induced AIN)
- Vascular (e.g., hypertensive nephrosclerosis, renovascular disease)
- Cystic (e.g., ADPKD)
- Transplant nephropathy
Key Points Summary
| Concept | Detail |
|---|---|
| System origin | NKF-KDOQI 2002 → KDIGO 2005 → KDIGO 2012 (current) |
| Minimum duration | >3 months |
| "CGA" staging | Cause + GFR category (G1-G5) + Albuminuria category (A1-A3) |
| G3 split rationale | G3a vs 3b have meaningfully different risk profiles and complications |
| G1-G2 alone | Do NOT qualify as CKD without a marker of kidney damage |
| Albuminuria addition | Both GFR and albuminuria are independent, graded predictors of ESKD, CVD, death |
| ESKD definition | G5 requiring KRT (dialysis or transplant) = G5D or G5T |
Sources: Brenner and Rector's The Kidney, 2-Volume Set; National Kidney Foundation Primer on Kidney Diseases, 8e; Comprehensive Clinical Nephrology, 7th Edition; Textbook of Family Medicine, 9e.
Calculate eGFR for creatine 2.88, Age 72 years and male
Running Command
python3 -c " import math # CKD-EPI 2021 (race-free) equation # eGFR = 142 × min…
eGFR Calculation Result
Formula used: CKD-EPI 2021 (race-free, KDIGO-recommended)
$$eGFR = 142 \times \min(S_{Cr}/\kappa,\ 1)^\alpha \times \max(S_{Cr}/\kappa,\ 1)^{-1.200} \times 0.9938^{Age}$$
For males: κ = 0.9, α = -0.302
Step-by-step
| Parameter | Value |
|---|---|
| Serum creatinine | 2.88 mg/dL |
| Age | 72 years |
| Sex | Male |
| Scr / κ (2.88 ÷ 0.9) | 3.20 |
| min(3.20, 1)^(-0.302) | 1.000000 |
| max(3.20, 1)^(-1.200) | 0.247640 |
| 0.9938^72 (age factor) | 0.639039 |
$$eGFR = 142 \times 1.0 \times 0.2476 \times 0.6390 = \mathbf{22.47\ mL/min/1.73\ m^2}$$
Result
eGFR = 22.47 mL/min/1.73 m²
CKD Stage G4 - Severely Decreased
Clinical Implications (CKD G4)
| Domain | Action |
|---|---|
| KRT planning | Refer for dialysis/transplant education now; construct AVF if HD planned (takes 8-12 weeks to mature) |
| Medications | Dose-adjust all renally cleared drugs; avoid NSAIDs, nephrotoxins, iodinated contrast |
| Hold/review | Metformin (hold if eGFR <30), direct oral anticoagulants need dose adjustment |
| Complications | Actively manage hyperphosphatemia, hyperparathyroidism, metabolic acidosis, hyperkalemia, anemia |
| BP target | <130/80 mmHg; optimize RAS blockade if proteinuric |
| SGLT2 inhibitors | Consider if diabetic or proteinuric (evidence of benefit down to eGFR ~20) |
| Nephrology | Should already be under specialist care; intensify follow-up frequency |
At G4, KDIGO recommends preparing for KRT when eGFR is approaching 15 mL/min/1.73 m² or there is evidence of progressive decline - this patient is approaching that threshold.
Metronidazole DF in CKD patient
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Searching the Web
metronidazole dose adjustment CKD renal impairment dialysis ESRD guidelines
Excellent - I now have comprehensive, authoritative data. Here is the full answer:
Metronidazole Dose Adjustment in CKD
Pharmacokinetic Basis
| Parameter | Detail |
|---|---|
| Absorption | Rapidly and completely absorbed orally; peak plasma level in 1-3 hours |
| Protein binding | Low (10-20%) |
| Metabolism | Primarily hepatic - oxidative metabolism + glucuronide conjugation |
| Half-life (parent drug) | ~7.5 hours (normal renal function) |
| Excretion | Metronidazole and its metabolites excreted mainly in urine |
| Key metabolites | Hydroxy-metronidazole (active, ~30% activity of parent) and metronidazole acetate |
The parent drug is hepatically cleared, so renal function has little effect on metronidazole pharmacokinetics itself. However, the polar metabolites are renally excreted and accumulate significantly in severe CKD/ESRD.
- Katzung's Basic & Clinical Pharmacology, 16th Ed., line 2700
Dose Adjustment Recommendations
CKD (not on dialysis)
| eGFR / CrCl | Recommendation |
|---|---|
| >10 mL/min | No dose adjustment required |
| <10 mL/min (not on dialysis) | Variable - most guidelines recommend no change; some suggest 50% dose reduction or 500 mg q12h given metabolite accumulation risk. Monitor for adverse effects. |
The FDA label states: "Decreased renal function does not alter the single-dose pharmacokinetics of metronidazole." No specific dose reduction is required based on renal function alone.
This patient (eGFR 22.47, CKD G4) falls comfortably in the >10 mL/min category - no dose adjustment needed.
Dialysis Patients
| Modality | Key Facts | Recommendation |
|---|---|---|
| Hemodialysis (HD) | HD removes 40-65% of metronidazole in a 4-8 hour session (depends on membrane type) | Administer dose after HD session; consider supplemental dose if timing cannot be separated from dialysis |
| CAPD (peritoneal dialysis) | Only ~10% removed per 7.5h session | No supplemental dose needed |
FDA label: "If the administration of metronidazole cannot be separated from the dialysis session, supplementation of metronidazole dose following hemodialysis should be considered."
Hepatic Impairment (contrast with renal)
Since metronidazole is hepatically cleared, this is where dose adjustment IS required:
- Severe hepatic impairment (Child-Pugh C): Reduce dose by 50%
- Plasma clearance is decreased and half-life prolonged significantly
ESRD Metabolite Accumulation - Clinical Warning
In ESRD patients receiving 500 mg IV metronidazole:
- Hydroxy-metronidazole Cmax: 2-fold higher than normal renal function
- Metronidazole acetate Cmax: 5-fold higher than normal renal function
These metabolites may contribute to neurotoxicity (peripheral neuropathy, encephalopathy, cerebellar dysfunction) with prolonged courses.
FDA recommendation: "Monitor for metronidazole-associated adverse events" in ESRD patients.
Practical Summary for This Patient (eGFR 22.47, CKD G4)
| Question | Answer |
|---|---|
| Dose adjustment needed? | No - standard dosing applies |
| Usual adult dose | 400-500 mg TDS (oral) or 500 mg q8h IV depending on indication |
| Monitoring needed? | Yes - watch for GI side effects and neurotoxicity (peripheral neuropathy) especially if course >7-10 days |
| If progresses to ESRD on HD | Give dose after dialysis; consider supplemental dose |
| If CAPD | No supplemental dose needed |
| Hepatic function | Check - if significant liver disease co-exists, reduce by 50% |
Key principle: Metronidazole is one of the few antibiotics that does not require renal dose adjustment in CKD because its clearance is hepatic. Dose reduction is only needed in severe hepatic failure, or as a precaution in anuric patients not on dialysis (where metabolites cannot be cleared at all).
- Sources: FDA Flagyl prescribing information; Katzung's Basic & Clinical Pharmacology, 16th Ed.; UNMC Antimicrobial Renal Dosing Guidelines; University Hospital antimicrobial dosing table
Is dose adjustment required for aciloc
Finding Sources
Searching the Web
ranitidine aciloc dose adjustment CKD renal impairment GFR hemodialysis
Reading File
Finding Sources
I now have all the information needed for a complete answer.
Aciloc (Ranitidine) - Dose Adjustment in CKD
Short answer: YES - dose reduction is required when CrCl/eGFR falls below 50 mL/min.
Pharmacokinetic Basis
| Parameter | Detail |
|---|---|
| Absorption | Well absorbed orally; peak levels in 1-3 hours; unaffected by food |
| First-pass metabolism | ~35-60% hepatic first-pass effect (reduces bioavailability) |
| Elimination | Combined renal excretion + hepatic metabolism |
| Renal contribution | ~70% of absorbed drug excreted unchanged in urine |
| Half-life (normal) | ~2-3 hours; prolonged in renal impairment |
| CYP interaction | Inhibits CYP mixed-function oxidase (warfarin, theophylline, phenytoin, lidocaine) |
Because ranitidine relies heavily on renal excretion, impaired kidney function leads to drug accumulation and prolonged half-life.
- Sleisenger and Fordtran's GI and Liver Disease, block 12, line 3336
Dose Adjustment Recommendations
| CrCl / eGFR | Standard Dose | Adjusted Dose |
|---|---|---|
| >50 mL/min | 150 mg BD or 300 mg OD | No adjustment |
| 25-50 mL/min | Normal | 150 mg BD → reduce to ~75% (150 mg once daily or 150 mg BD with caution) |
| 10-25 mL/min | Normal | 50% of usual dose → 150 mg once daily |
| <10 mL/min | Normal | 25% of usual dose → 75 mg once daily |
| Hemodialysis | — | Dialysis does not remove substantial amounts of H2RAs; no supplemental dose needed. Give usual adjusted dose. |
| CAPD | — | Same as CrCl <10 - no supplemental dose |
Key threshold: Dose reductions are recommended when creatinine clearance is below 50 mL/min.
- Sleisenger and Fordtran's GI and Liver Disease
For This Patient (eGFR 22.47 mL/min, CKD G4)
| Parameter | Value |
|---|---|
| eGFR | 22.47 mL/min/1.73 m² |
| CKD Stage | G4 |
| Applicable bracket | CrCl 10-25 mL/min |
| Recommended dose | 150 mg once daily (50% dose reduction) |
| Dialysis supplement | Not required |
Important Additional Notes
1. CYP450 Interaction Warning
Ranitidine inhibits hepatic CYP mixed-function oxidase - monitor for toxicity if co-prescribed with:
- Warfarin (INR can rise)
- Theophylline
- Phenytoin
- Lidocaine, quinidine
2. Compare with other acid-suppressants in CKD:
| Drug | Renal Adjustment? |
|---|---|
| Ranitidine (H2RA) | YES - reduce dose if CrCl <50 |
| Famotidine (H2RA) | YES - more aggressive reduction needed |
| Omeprazole / Pantoprazole (PPI) | No - hepatically metabolised, no renal adjustment required |
| Nizatidine (H2RA) | YES - similar to ranitidine |
PPIs undergo significant hepatic metabolism with no dose adjustment required for renal or even hepatic impairment - making them a safer and often preferred choice in CKD G4-G5 patients.
3. Market note: Ranitidine was withdrawn from several markets in 2020 due to NDMA (probable carcinogen) contamination concerns. Famotidine is the H2RA of choice if an H2RA is still needed. For a CKD G4 patient like the one in our previous discussion (eGFR 22.47), a PPI such as pantoprazole or omeprazole would typically be preferred over any H2RA - no dose adjustment needed and safer profile.
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease; FPNotebook Drug Dosing in CKD guidelines.
Does esmoprazole required dose adjustment
Finding Sources
Finding Sources
Cap bifilac in CKD
Searching the Web
Bifilac capsule composition ingredients probiotic strains
Finding Sources
Finding Sources
Searching the Web
probiotics CKD renal failure safety benefit gut microbiome uremia
Cap Bifilac in CKD
Composition of Bifilac Capsule
Each capsule contains 4 probiotic strains (patented Japanese TOA strains):
| Strain | Count per Capsule | Role |
|---|---|---|
| Streptococcus faecalis T-110 | 30 million CFU | Restores intestinal flora, inhibits pathogens |
| Clostridium butyricum TO-A | 2 million CFU | Produces butyrate, supports colonocyte health |
| Bacillus mesentericus TO-A | 1 million CFU | Produces enzymes, creates favourable gut pH |
| Lactobacillus sporogenes | 50 million CFU | Lactic acid producing bacteria, barrier integrity |
Dose Adjustment in CKD?
No dose adjustment required.
Bifilac is a non-systemically absorbed probiotic - the live bacteria act locally within the GI tract, are not renally excreted, and do not undergo renal clearance. CKD stage (any G1-G5) does not alter its pharmacokinetics.
Is Bifilac Safe in CKD?
Yes - and it may actually be beneficial. CKD creates a specific pattern of gut dysbiosis that probiotics can help correct:
The Gut-Kidney Axis in CKD
| CKD Effect on Gut | Consequence |
|---|---|
| Uremic toxin accumulation | Alters intestinal epithelial integrity ("leaky gut") |
| Dietary protein restriction | Reduces substrate for beneficial bacteria |
| Reduced GFR → urea diffusion into gut | Overgrowth of urease-producing bacteria; excess ammonia production |
| Dysbiosis | Increased production of indoxyl sulfate, p-cresol sulfate (protein-bound uremic toxins) → accelerate CKD progression |
| Chronic inflammation | Elevated IL-6, CRP, oxidative stress |
Benefits of Probiotics in CKD
| Benefit | Mechanism |
|---|---|
| Reduces uremic toxins | Less intestinal production of indoxyl sulfate and p-cresyl sulfate |
| Improves gut barrier integrity | Reduces endotoxemia and systemic inflammation |
| Decreases BUN/urea | Bacteria utilize urea nitrogen in the gut |
| Reduces inflammation | Lowers CRP, IL-6 |
| Prevents antibiotic-associated diarrhea | Especially relevant as CKD patients receive frequent antibiotics |
| May slow CKD progression | By reducing uremic toxin-mediated tubular injury |
Clostridium butyricum in Bifilac specifically produces butyrate - a short-chain fatty acid that is the primary energy source for colonocytes and helps repair the intestinal barrier disrupted by uremia.
Cautions in CKD (Specific Situations)
| Situation | Concern |
|---|---|
| Severely immunocompromised (transplant patients on high-dose immunosuppression) | Theoretical risk of bacterial translocation/bacteremia - use caution, especially with live Streptococcus faecalis strains |
| Active severe illness / sepsis | Avoid - risk of translocation |
| Concurrent antibiotics | Give Bifilac at least 2 hours apart from antibiotics to preserve viability |
| CKD G4-G5 on dialysis | Safe to use; no dose change needed |
Summary
| Question | Answer |
|---|---|
| Dose adjustment in CKD? | No |
| Safe in CKD? | Yes |
| Beneficial in CKD? | Potentially yes - via gut-kidney axis |
| When to be cautious? | Transplant/severely immunosuppressed patients |
| Timing with antibiotics? | Give 2 hours apart |
| Dialysis patients (HD/CAPD)? | Safe, no adjustment needed |
Bifilac is not only safe in CKD - it is a rational adjunct in CKD management given the well-documented gut dysbiosis in these patients, especially those on antibiotics or experiencing GI complaints.
Is pantoprazole safe in CKD
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
I also have the textbook confirmation from our previous session (Sleisenger & Fordtran) that PPIs undergo significant hepatic metabolism with no renal adjustment required. Combined with this new pharmacokinetic data, here is the complete answer:
Pantoprazole Safety in CKD
Short Answer
Yes - Pantoprazole is safe in CKD at all stages (G1-G5), including dialysis patients. No dose adjustment is required for renal impairment.
Pharmacokinetic Basis - Why No Renal Adjustment?
| Parameter | Pantoprazole |
|---|---|
| Mechanism | Irreversible H⁺/K⁺-ATPase (proton pump) inhibitor - prodrug activated by acid |
| Absorption | Enteric-coated; peak levels 2-5 hours after oral dose |
| Metabolism | Predominantly hepatic - CYP2C19 (major) + CYP3A4 (minor) |
| Renal excretion | Minimal - only inactive metabolites excreted in urine (~71% urinary, but as inactive sulphate and glucuronide conjugates) |
| Half-life | ~1-2 hours (short, but duration of acid suppression is prolonged due to covalent proton pump binding) |
| Effect of renal impairment | Negligible - parent drug clearance is entirely hepatic; inactive metabolite accumulation has no clinical consequence |
| Dialysis removal | Not significantly removed by hemodialysis or CAPD |
PPIs are prodrugs that require acid activation in the parietal cell canaliculus. They bind covalently to the H⁺/K⁺-ATPase. Their short plasma half-life is irrelevant to duration of acid suppression - acid secretion only resumes when new pump proteins are synthesized (18-24 hours). This mechanism is entirely independent of renal function.
- Yamada's Textbook of Gastroenterology, 7th Ed., line 437-443
- Sleisenger and Fordtran's GI and Liver Disease (confirmed: PPIs undergo significant hepatic metabolism; dose adjustments not required for renal impairment)
Dose in CKD - All Stages
| CKD Stage | eGFR | Pantoprazole Dose | Adjustment? |
|---|---|---|---|
| G1 | ≥90 | 40 mg OD (standard) | None |
| G2 | 60-89 | 40 mg OD | None |
| G3a | 45-59 | 40 mg OD | None |
| G3b | 30-44 | 40 mg OD | None |
| G4 | 15-29 (our patient) | 40 mg OD | None |
| G5 | <15 | 40 mg OD | None |
| Hemodialysis | — | 40 mg OD | None |
| CAPD | — | 40 mg OD | None |
Where Dose Adjustment IS Needed for Pantoprazole
| Condition | Adjustment |
|---|---|
| Severe hepatic impairment (Child-Pugh C) | Max 20 mg/day; do not exceed 40 mg |
| Renal impairment (any degree) | No change |
| CYP2C19 poor metabolizers | Standard dose; consider 50% reduction for long-term use once efficacy achieved |
| CYP2C19 ultrarapid metabolizers | May need dose increase (100% more) for H. pylori / erosive esophagitis |
The only clinically significant dose modification for pantoprazole is in severe liver disease, not in kidney disease.
Important Caution: Long-Term PPI Use in CKD
While no dose adjustment is needed, long-term PPI use in CKD carries some specific concerns worth monitoring:
| Adverse Effect | Relevance in CKD |
|---|---|
| Hypomagnesaemia | CKD patients may already have electrolyte disturbances; monitor Mg²⁺ |
| Hypocalcaemia / Bone fractures | CKD-MBD already predisposes to bone disease; PPIs further reduce Ca²⁺ absorption |
| CKD progression | Emerging epidemiological data suggests long-term PPIs may be independently associated with incident CKD and faster eGFR decline (mechanism: hypomagnesaemia-induced tubular injury, interstitial nephritis) |
| Acute interstitial nephritis (AIN) | Rare idiosyncratic reaction - if eGFR acutely worsens on PPI, consider AIN |
| Vitamin B12 deficiency | Long-term acid suppression impairs B12 absorption; relevant in dialysis patients |
| C. difficile infection | CKD patients are frequently hospitalised and antibiotic-exposed - PPIs increase C. diff risk |
- Yamada's Textbook of Gastroenterology, 7th Ed., line 443: "emerging evidence suggests there may be more adverse events particularly with long-term use...such as electrolyte imbalances, bone fractures, renal disease, and infections"
Bottom Line for This Patient (eGFR 22.47, CKD G4)
| Question | Answer |
|---|---|
| Safe to prescribe? | Yes |
| Dose? | Pantoprazole 40 mg once daily - standard dose, no adjustment |
| Better than ranitidine in this patient? | Yes - ranitidine requires 50% dose reduction at this eGFR; pantoprazole needs none |
| Long-term monitoring? | Check Mg²⁺, Ca²⁺ periodically; review ongoing need regularly |
| When to stop? | Use lowest effective dose for shortest necessary duration - especially in CKD where long-term risks exist |
This is a shared conversation. Sign in to Orris to start your own chat.