Hypoglycaemia in 40 year old female with history of diabetes in mother under evaluation
Reading File
Finding Sources
Finding Sources
Searching PubMed
hypoglycemia evaluation non-diabetic adult causes
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive information. Let me compile the full clinical answer.
Hypoglycemia in a 40-Year-Old Female - Clinical Evaluation
Preliminary context: This is a non-diabetic (or previously undiagnosed) 40-year-old woman presenting with hypoglycemia, with a maternal family history of diabetes. The family history raises the possibility of MODY or early type 2 DM, but the primary issue right now is investigating why she is hypoglycemic. The full differential must be worked through systematically.
Step 1 - Confirm Hypoglycemia: Whipple's Triad
Before any workup, Whipple's Triad must be established:
- Symptoms and/or signs of hypoglycemia (autonomic: sweating, tremor, palpitations; neuroglycopenic: confusion, visual changes, seizure)
- Documented low plasma glucose < 55 mg/dL (3.0 mmol/L) on a lab-measured sample (not just a glucometer - whole blood reads ~15% lower than plasma)
- Resolution of symptoms after plasma glucose is raised
Do not pursue extensive investigation without Whipple's triad. Absence of symptoms during documented low glucose suggests artifactual hypoglycemia (e.g., delay in sample processing, polycythemia, leukocytosis). Collect blood in a fluoride-oxalate tube and analyze promptly.
- Washington Manual of Medical Therapeutics, p. 911
- Goldman-Cecil Medicine, p. 2495
Step 2 - Initial History-Directed Classification
| Feature | Points Toward |
|---|---|
| Symptoms after prolonged fast (12-14h) | Insulinoma, hormonal deficiency, gluconeogenesis defect |
| Symptoms 1-5h postprandially | Dumping, non-insulinoma pancreatogenous hypoglycemia, insulin autoimmune syndrome |
| Symptoms 2-3h after eating | Hyperinsulinism, glycogen storage disease |
| Hx of bariatric/gastric surgery | Post-bypass hyperinsulinism |
| Drug use (sulfonylureas, insulin, salicylates, alcohol, beta-blockers, quinine) | Drug-induced hypoglycemia |
| Chronic illness (liver, renal, adrenal) | Secondary hypoglycemia |
| Family history of diabetes (maternal) | MODY, early T2DM, GCK mutation carrier |
Goldman-Cecil Medicine, Table 211-1
Step 3 - Differential Diagnosis in This Patient
A. Hyperinsulinemic (most important to exclude)
| Cause | Key Feature |
|---|---|
| Insulinoma | Most common endogenous cause in adults; fasting hypoglycemia; insulin ≥3 µU/mL + C-peptide ≥200 pmol/L + proinsulin ≥5 pmol/L with glucose <55 mg/dL |
| Non-insulinoma pancreatogenous hypoglycemia (NIPHS) | Postprandial; no single tumor on imaging |
| Insulin autoimmune syndrome (Hirata's) | High-titer insulin antibodies; can be fasting or postprandial; rare; associated with sulfhydryl drugs (methimazole, carbimazole, captopril) |
| Factitious hypoglycemia | Exogenous insulin (C-peptide suppressed) or sulfonylurea (C-peptide elevated, screen for SFU in blood) |
| GCK/HNF mutations (MODY) | Relevant given maternal DM history - GCK-MODY causes mild stable fasting hyperglycemia, but some activating GCK mutations paradoxically cause fasting hypoglycemia |
B. Hormonal Deficiency
| Cause | Notes |
|---|---|
| Cortisol/ACTH deficiency | Addison's disease, pituitary failure; morning cortisol + ACTH stimulation test |
| Growth hormone deficiency | Reduces gluconeogenesis; measure IGF-1/GH |
| Hypothyroidism | Can impair gluconeogenesis/glycogenolysis |
C. Drug-Induced (must always ask explicitly)
- Sulfonylureas, insulin (even if patient denies - check SFU metabolites in blood)
- Alcohol (inhibits hepatic gluconeogenesis)
- Salicylates, quinine, beta-blockers, pentamidine, fluoroquinolones
D. Systemic/Organ Failure
- Severe hepatic insufficiency (check LFTs, liver synthetic function)
- Renal failure (kidneys contribute to gluconeogenesis; impaired insulin clearance)
- Sepsis, starvation, eating disorders
E. Family History Context - The MODY Angle
The mother's diabetes raises two important considerations:
- MODY (Maturity-Onset Diabetes of the Young): Autosomal dominant monogenic diabetes. If the patient herself has mild fasting hyperglycemia rather than hypoglycemia, GCK-MODY is the most common stable form. However, activating mutations in GCK are a rare cause of hypoglycemia (the glucose setpoint is shifted down). Other MODY types (HNF4A, HNF1A) can present with hypoglycemia in infancy/childhood.
- Risk of T2DM: First-degree family history of T2DM increases her own risk. However, T2DM itself would not explain hypoglycemia unless she is on antidiabetic medications.
Tietz Laboratory Medicine, p. Monogenic DM section
Step 4 - Diagnostic Approach (Ketone-Based Algorithm)
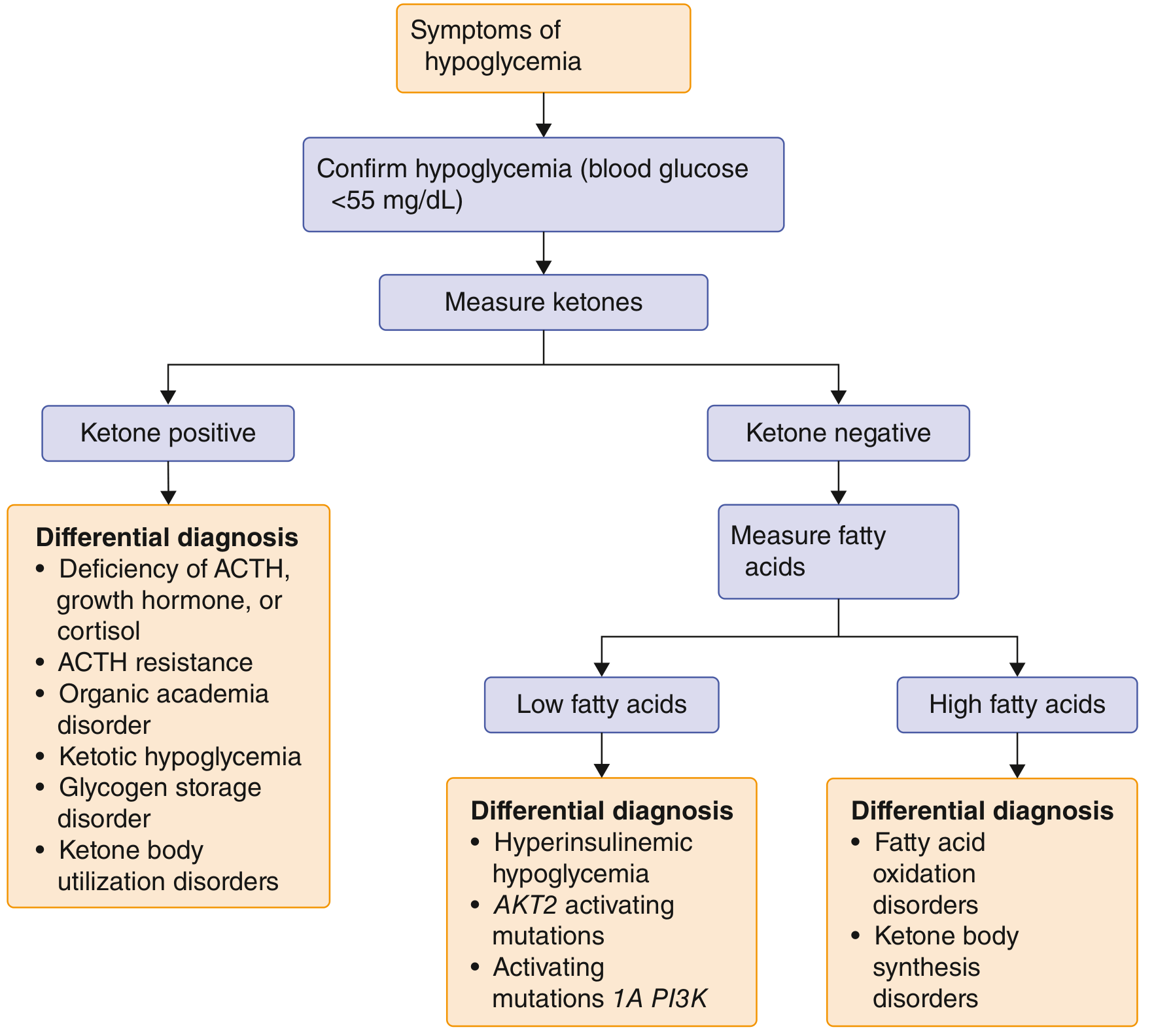
First branch - Measure beta-hydroxybutyrate (ketones) at the time of hypoglycemia:
- Ketone-positive (≥2.7 mmol/L): Points toward counter-regulatory hormone deficiency (ACTH, cortisol, GH), organic acidemia, or glycogen storage disorder. Hyperinsulinism is less likely.
- Ketone-negative (<2.7 mmol/L): Suppressed ketogenesis suggests hyperinsulinism (insulin suppresses lipolysis and ketogenesis). Measure fatty acids next.
- Low fatty acids → Hyperinsulinemic hypoglycemia (insulinoma, autoimmune, factitious)
- High fatty acids → Fatty acid oxidation disorder or ketone synthesis disorder
Step 5 - Laboratory Investigations
Immediate (during a hypoglycemic episode or at the conclusion of the fast):
| Test | Purpose |
|---|---|
| Plasma glucose (lab, fluoride tube) | Confirm <55 mg/dL |
| Serum insulin | ≥3 µU/mL = inappropriate |
| C-peptide | ≥200 pmol/L = endogenous insulin; suppressed in exogenous insulin use |
| Proinsulin | ≥5 pmol/L |
| Beta-hydroxybutyrate | <2.7 mmol/L suggests insulin-mediated |
| Sulfonylurea/meglitinide screen | Rule out factitious/drug-induced |
| Insulin antibodies | Rule out autoimmune insulin syndrome |
| IGF-1, IGF-2 | If non-islet cell tumor suspected |
Additional:
| Test | Purpose |
|---|---|
| Morning cortisol, ACTH stimulation test | Adrenal insufficiency |
| IGF-1/GH | GH deficiency |
| Thyroid function (TSH, FT4) | Hypothyroidism |
| LFTs, albumin, PT/INR | Hepatic cause |
| Renal function (eGFR, urea) | Renal cause |
| HbA1c | Overall glycemic context; low HbA1c despite documented hypoglycemia supports factitious or insulin autoimmune |
Step 6 - Provocative/Confirmatory Tests
72-Hour Supervised Fast (gold standard for fasting hypoglycemia)
Protocol (Goldman-Cecil Medicine, Table 211-3):
- Start after last meal; stop interfering medications
- Water permitted; patient active during waking hours
- Blood for glucose, insulin, C-peptide, β-hydroxybutyrate every 6 hours until glucose <60 mg/dL, then every 1-2 hours
- End the fast when: glucose ≤45 mg/dL with symptoms, or Whipple's triad already established with glucose ≤55 mg/dL, or 72 hours elapsed without hypoglycemia
- At end: collect glucose, insulin, C-peptide, proinsulin, β-hydroxybutyrate, SFU screen → give IV glucagon 1 mg → measure glucose at 10, 20, 30 min (positive response = rise ≥25 mg/dL indicates hyperinsulinism with preserved hepatic glycogen)
Important note: Healthy thin/lean women may have plasma glucose as low as 40 mg/dL during a 72-hour fast without symptoms - this does not confirm a hypoglycemic disorder if Whipple's triad is absent.
Mixed-Meal Test (for postprandial symptoms)
- If symptoms occur 1-5 hours after meals, collect glucose, insulin, C-peptide, proinsulin every 30 minutes for 300 minutes after a meal similar to what triggers symptoms
- Positive: neuroglycopenic symptoms + glucose ≤50 mg/dL
Goldman-Cecil Medicine, pp. 2495-2497
Step 7 - Imaging (once biochemical hyperinsulinism confirmed)
If endogenous hyperinsulinism confirmed (insulinoma most likely):
- Multiphasic pancreatic CT or MRI pancreas - first line
- Endoscopic ultrasound (EUS) - detects small tumors not seen on CT
- 68Ga-DOTATATE PET-CT - for neuroendocrine tumors
- Selective arterial calcium stimulation test - if imaging negative, localizes functional hyperinsulinism to a pancreatic region
Key Clinical Reasoning Points for This Patient
-
Mother's diabetes does not directly cause this patient's hypoglycemia - but raises two specific concerns:
- She may unknowingly be using her mother's antidiabetic medications (sulfonylurea screen mandatory)
- Rare activating GCK mutations cause hypoglycemia and run in families with a "diabetic" phenotype (siblings may have hyperglycemia while she has hypoglycemia due to a different mutation)
-
A 40-year-old woman - insulinoma incidence peaks in the 4th-6th decades; the triad of hypoglycemic episodes, especially fasting, should trigger a 72-hour fast
-
Factitious hypoglycemia must always be considered - exogenous insulin gives suppressed C-peptide with elevated insulin; SFU gives elevated C-peptide and positive drug screen
-
Adrenal insufficiency is often overlooked in women this age and can be insidious
Summary Workup Algorithm
Whipple's Triad confirmed?
↓ Yes
Measure at time of hypoglycemia:
Glucose + Insulin + C-peptide + Proinsulin + β-hydroxybutyrate + SFU screen
↓
β-OHB < 2.7 → Hyperinsulinism suspected
↓
72-hour fast (if fasting sx) or Mixed-meal test (if postprandial sx)
↓
Hyperinsulinism confirmed (Insulin ≥3 µU/mL, C-pep ≥200 pmol/L)?
→ Check insulin antibodies → if negative → imaging for insulinoma
→ C-peptide suppressed? → factitious (exogenous insulin)
→ SFU positive? → drug-induced
↓
β-OHB > 2.7 → Hormonal deficiency workup (cortisol, ACTH stim, GH, TFTs)
References:
- Washington Manual of Medical Therapeutics, p. 911 (Evaluation of hypoglycemia without diabetes)
- Goldman-Cecil Medicine, 2-Vol Set, pp. 2491-2497 (Differential diagnosis and evaluation protocol)
- Tietz Textbook of Laboratory Medicine 7th Ed., p. 1135 (Prolonged fast protocol)
Recent literature: A 2025 review (Looi & Lawler, J Clin Med) covers current evaluation and management of non-diabetic hypoglycemia in adults and may update some nuances in the Endocrine Society 2009 guidelines (PMID: 40648766).
Create a diagnostic flowchart/summary document for this hypoglycemia workup0
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.