I need very authentic information that is scarpa fascia outer layer or campers fascia outer layer? Tell me in detail the anterior abdominal wall layers
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything I need from 4 major surgical textbooks plus anatomical diagrams. Here is the complete, authentic answer:
Anterior Abdominal Wall Layers - Authoritative Answer
The Direct Answer to Your Question: Which is the Outer Layer?
Camper's fascia is the OUTER (superficial/fatty) layer.
Scarpa's fascia is the INNER (deep/membranous) layer.
This is confirmed unanimously by every major surgical and anatomy textbook. There is no ambiguity here.
"Below the umbilicus, the division between a fatty outer anterior layer, Camper's fascia, and a membranous inner layer, Scarpa's fascia, becomes apparent."
- Sabiston Textbook of Surgery, p. 1647
"The subcutaneous tissue of the lower abdominal wall is composed of two layers: a superficial fatty layer (Camper fascia) and a deep membranous layer (Scarpa fascia)."
- Campbell-Walsh-Wein Urology
"The superficial layer is the subcutaneous fascia of Camper ... The deep layer (the actual superficial body fascia) is the superficial abdominal fascia of Scarpa."
- THIEME Atlas of Anatomy
Complete Layers of the Anterior Abdominal Wall
The anterior abdominal wall is a hexagonal region bounded superiorly by the costal margin and xiphoid process, laterally by the midaxillary lines, and inferiorly by the pubic symphysis, inguinal ligaments, and iliac crests.
From superficial (outside) to deep (inside), the layers are:
Layer 1 - Skin
The outermost layer. Standard skin with dermis and epidermis.
Layer 2 - Subcutaneous Tissue (Superficial Fascia)
This is where the Camper/Scarpa distinction lies. It is divided into two sub-layers, but this division is only distinct below the umbilicus. Above the umbilicus, they are fused into a single indistinct layer.
2a - Camper's Fascia (Fatty/Superficial layer - OUTER)
- Named after Peter Camper (1722-1789), professor of anatomy, surgery, and medicine in Amsterdam
- Fatty, adipose-rich layer (panniculus adiposus)
- Thickness varies widely with body habitus
- Continuous inferiorly with the superficial thigh fascia, and extends into the scrotum in males (where it contributes to the dartos muscle fibers) and labia majora in females
- Contains the superficial epigastric vessels and superficial circumflex iliac vessels (tributaries of the femoral vessels)
- Contains lymphatic vessels draining to the inguinal lymph nodes
2b - Scarpa's Fascia (Membranous/Deep layer - INNER)
- Named after Antonio Scarpa (1747-1832), professor of anatomy and surgery in Modena
- A fibrous, membranous layer - not fatty
- Consists of compressed fibrous components of the deep superficial fascia
- Fuses with the anterior layer of fascia of the flank and back laterally
- Inferiorly, it attaches firmly to the fascia lata of the thigh (just below the inguinal ligament), forming a closed potential space - this is why urine from a ruptured urethra tracks upward into the abdominal wall rather than downward into the thigh
- Forms the fundiform ligament of the penis (or suspensory ligament of the clitoris)
- Continuous with Colles fascia of the perineum
"Scarpa fascia actually consists of compressed fibrous components of the superficial fascia."
- Mulholland and Greenfield's Surgery, 7th Ed.
Layer 3 - Deep (Investing) Fascia
A thin fascial layer (sometimes called fascia innominata) that invests the external oblique muscle. It fuses inferiorly with the inguinal ligament and pubis, and blends with the fascia lata of the thigh.
Layer 4 - Muscles and their Aponeuroses
The muscles are arranged in two groups:
Midline - Rectus Abdominis (paired)
- Runs vertically from the pubic symphysis/crest to the xiphoid process and 5th-7th costal cartilages
- Has 3 tendinous intersections along its length
- Enclosed in the rectus sheath formed by aponeuroses of the lateral muscles
Lateral - Three flat muscles (outside to inside):
| Muscle | Origin | Fiber Direction | Insertion |
|---|---|---|---|
| External Oblique | 8th rib | Inferomedial ("hands in pockets") | Linea alba, anterior iliac crest |
| Internal Oblique | Thoracolumbar fascia | Superomedial (at right angle to external) | Lower costal margin, xiphoid, linea alba |
| Transversus Abdominis | Costal margin, lumbar fascia | Horizontal (transverse) | Linea alba, xiphoid, pubic symphysis |
Layer 5 - Transversalis Fascia
A continuous fascial lining deep to the transversus abdominis. It is the main structural barrier at this level. The posterior rectus sheath below the arcuate line is actually formed by transversalis fascia (not muscle aponeuroses).
Layer 6 - Preperitoneal (Extraperitoneal) Fat and Areolar Tissue
A variable layer of adipose and loose connective tissue between the transversalis fascia and peritoneum. This is the space used in laparoscopic/robotic preperitoneal hernia repair (TEP procedure).
Layer 7 - Parietal Peritoneum
The innermost layer; the serous lining of the abdominal cavity.
Summary Table
| Layer | Name | Key Feature |
|---|---|---|
| 1 | Skin | Epidermis + dermis |
| 2 (outer) | Camper's fascia | Fatty, superficial |
| 2 (inner) | Scarpa's fascia | Membranous, deep |
| 3 | Deep fascia (fascia innominata) | Invests ext. oblique |
| 4a | External oblique + aponeurosis | Inferomedial fibers |
| 4b | Internal oblique + aponeurosis | Superomedial fibers |
| 4c | Transversus abdominis + aponeurosis | Horizontal fibers |
| 4d | Rectus abdominis (midline, enclosed in sheath) | Vertical strap muscle |
| 5 | Transversalis fascia | Deep muscular fascia |
| 6 | Preperitoneal fat | Potential surgical space |
| 7 | Parietal peritoneum | Serous lining |
(Schwartz's Principles of Surgery, 11th Ed., lists 9 distinct layers: skin, subcutaneous tissue, superficial fascia, external oblique, internal oblique, transversus abdominis, transversalis fascia, preperitoneal fat, peritoneum.)
Important Clinical Notes on Scarpa's Fascia
-
Urethral injury / pelvic fractures: Urine extravasation from a ruptured urethra spreads within the space deep to Scarpa's fascia and superficial to the deep (investing) fascia of the perineum. Because Scarpa's fascia is attached to the fascia lata of the thigh at the inguinal ligament, urine cannot track into the thigh - instead it spreads up onto the abdominal wall and into the scrotum.
-
Surgical closure: Scarpa's fascia is the layer that should be closed (with absorbable suture) during lower abdominal incision closure to reduce the dead space and lower seroma/hematoma formation, particularly in Pfannenstiel incisions.
-
Above the umbilicus: Camper's and Scarpa's fasciae are fused and indistinct above the umbilicus. The two-layer division only becomes anatomically meaningful below the umbilicus.
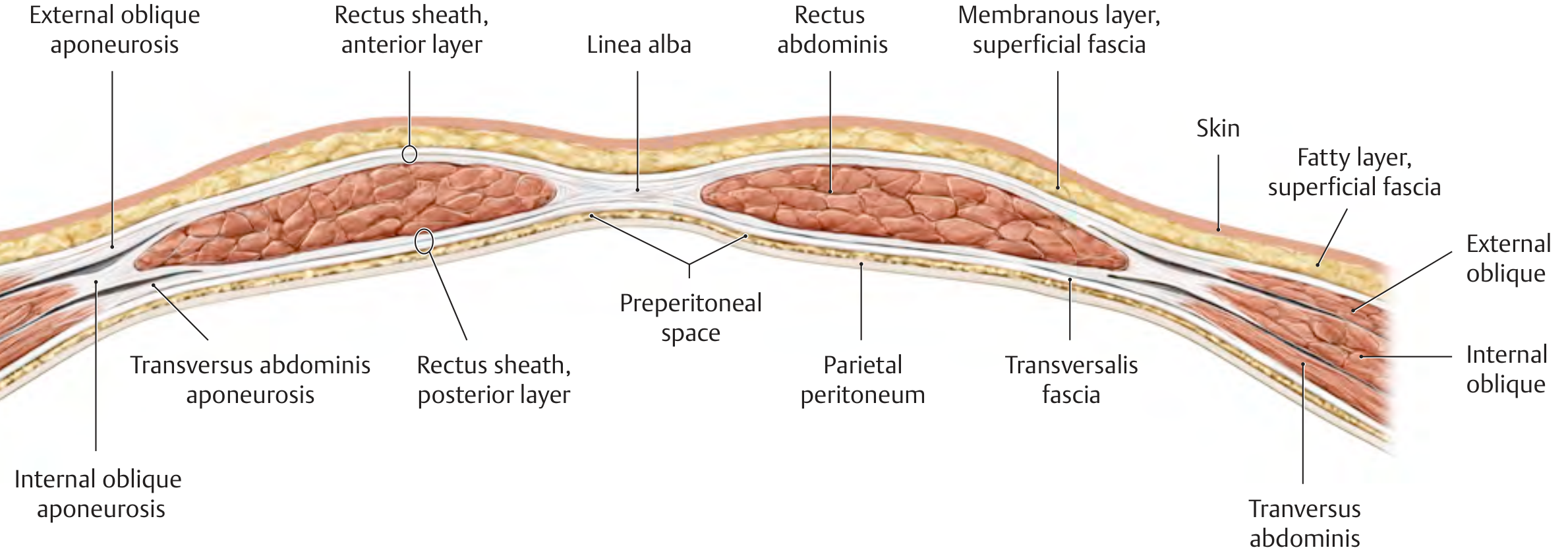
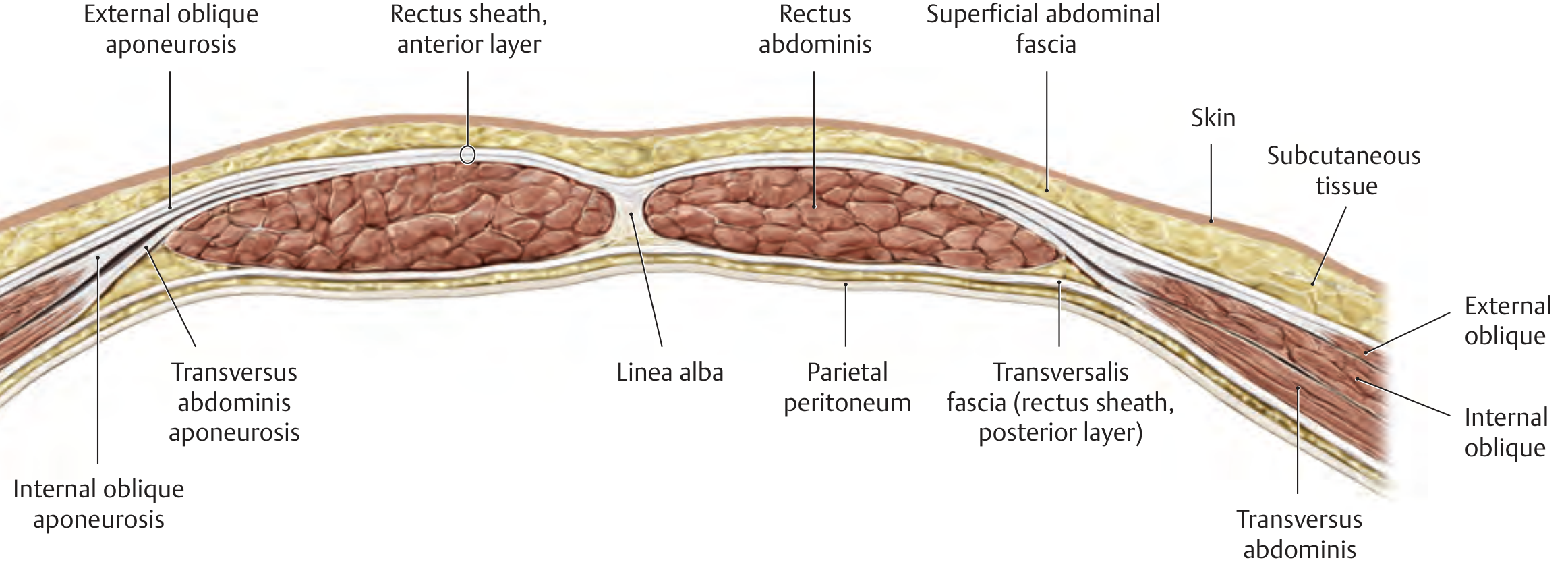
Anatomical Diagrams
Cross-section of the abdominal wall (THIEME Atlas of Anatomy), showing the layered structure with the fatty superficial layer (Camper's) outermost, membranous layer (Scarpa's) deep to it, then muscles, transversalis fascia, and peritoneum:
Sources consulted:
- Sabiston Textbook of Surgery, Chapter on Ventral Hernias
- Schwartz's Principles of Surgery, 11th Ed. - Surgical Anatomy of the Abdominal Wall
- Mulholland and Greenfield's Surgery, 7th Ed. - Superficial Fascia section
- THIEME Atlas of Anatomy - General Anatomy & Musculoskeletal System - Structure of the Abdominal Wall
This is a shared conversation. Sign in to Orris to start your own chat.