Dental caries
Reading File
Finding Sources
Searching PubMed
"dental caries"[MeSH Terms] AND prevention
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive material from multiple textbooks plus recent PubMed evidence. Let me compile the full response.
Dental Caries
Definition
Dental caries is a dynamic, multifactorial, infectious disease of the calcified tissues of the tooth - enamel, dentin, and cementum. It results from the progressive dissolution of tooth mineral by organic acids produced when microbial biofilm (plaque) ferments dietary carbohydrates. The lesion progresses inward from the tooth surface toward the pulp.
- Sherris & Ryan's Medical Microbiology, 8th Ed.
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Pathogenesis (Cariogenesis)
The process unfolds in four sequential steps, illustrated below:
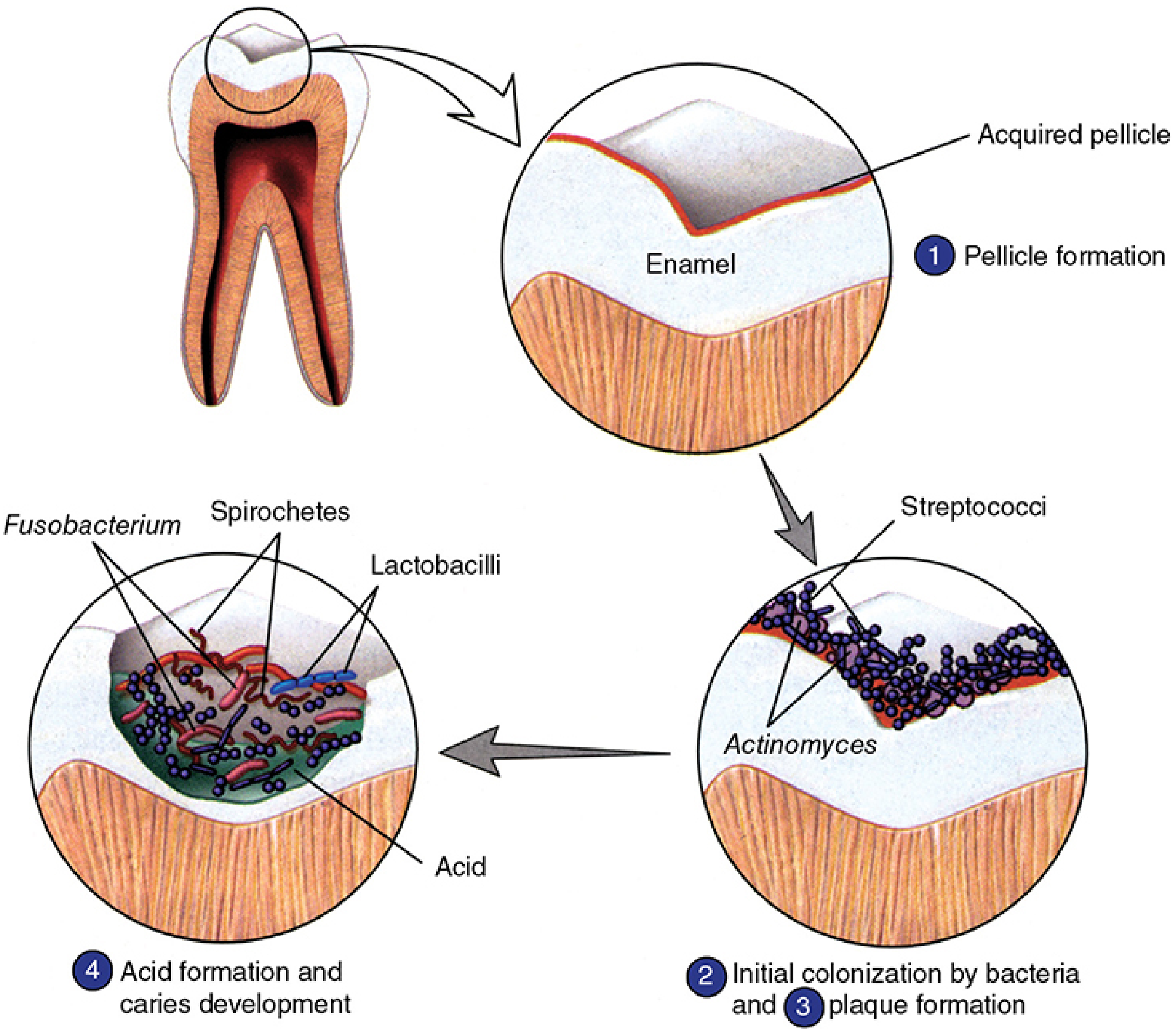
Step 1 - Acquired Pellicle Formation: A thin film of salivary glycoproteins deposits onto the clean enamel surface within minutes.
Step 2 - Initial Bacterial Colonization: Early colonizers (predominantly Streptococcus mutans, S. sanguis, S. mitis, Actinomyces spp.) adhere to the pellicle via ionic, hydrophobic, and lectin-like interactions.
Step 3 - Plaque Biofilm Maturation: Late colonizers (Gram-negative anaerobes - Porphyromonas, Prevotella, Fusobacterium, Treponema denticola) join within 2-4 days. S. mutans synthesizes high-molecular-weight extracellular glucan polymers from sucrose via glucosyltransferase enzymes, cementing the biofilm together. Mature plaque contains 300-400 bacterial species.
Step 4 - Acid Production and Demineralization: Glycolytic metabolism of dietary sugars (especially sucrose, glucose, fructose) generates lactic acid and other organic acids. pH drops below the critical threshold (~5.5 for enamel, ~6.0 for dentin), causing dissolution of hydroxyapatite crystals. The plaque microenvironment shields the acid from salivary buffering.
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28th Ed.
- Histology: A Text and Atlas (Wheater's), 8th Ed.
Key Organisms
| Organism | Role |
|---|---|
| Streptococcus mutans | Primary initiator; produces glucans, tolerates acid, synthesizes acid at low pH |
| S. sobrinus, S. salivarius, S. sanguis | Secondary contributors to acid pool |
| Lactobacillus acidophilus, L. casei | Drive active progression of established lesions |
| Actinomyces viscosus, A. naeslundii | Root surface caries; early biofilm formers |
Four Factors (Keyes' Triad + Time)
Scott-Brown's describes four interacting factors:
| Factor | Role |
|---|---|
| Dental plaque | Harbors acidogenic bacteria; creates a demineralizing microenvironment |
| Substrate | Refined carbohydrates (especially sucrose); naturally occurring sugars in fruit are also cariogenic |
| Dental tissues | Pits, fissures, inadequate contact points, and poor restoration margins favor plaque accumulation |
| Saliva | Cleansing, buffering, antibacterial (IgA, lysozyme, lactoferrin), and remineralization (calcium, phosphate, fluoride delivery) |
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Stages of Progression
-
Initial enamel lesion ("white spot"): Subsurface demineralization; enamel surface intact. Acid permeates enamel prism sheaths. Reversible with fluoride/remineralization. No cavitation.
-
Cavitation of enamel: Structural collapse once demineralization exceeds a threshold. Irreversible.
-
Dentin involvement: Caries spreads laterally at the amelodentinal junction, then along dentinal tubules. Bacterial invasion of tubules causes proteolysis and liquefaction foci.
-
Pulpal exposure (Pulpitis): Direct communication established between oral environment and vital pulp. Sensitivity to cold/sweet develops.
- Reversible pulpitis: Pain lasts seconds; stimulus-dependent.
- Irreversible pulpitis: Pain lasts minutes to hours; may be spontaneous.
-
Pulp necrosis and periradicular disease: Infection extends to periapical tissues - periapical abscess, periradicular periodontitis, cellulitis.
- Tintinalli's Emergency Medicine, 8th Ed.
Common Sites
- Pits and fissures of occlusal surfaces (most common)
- Interproximal surfaces (contact points)
- Gingival margins and exposed root surfaces (Actinomyces-driven)
- Smooth surfaces under plaque-retentive areas
Fluoride and Remineralization
Fluoride (optimal water concentration: 0.5-1.0 ppm) acts by three mechanisms:
- Substitutes fluoride ion for hydroxyl ion in hydroxyapatite → forms fluorapatite, which is less soluble in acid
- Direct antimicrobial effect on S. mutans (inhibits enolase, disrupts proton pump)
- Promotes remineralization of early subsurface lesions
- Histology: A Text and Atlas
Prevention
| Measure | Mechanism |
|---|---|
| Fluoride (water, toothpaste, varnish, gels) | Remineralization, acid resistance, antimicrobial |
| Dietary modification | Reduce free sugar frequency; limit sucrose exposure |
| Oral hygiene (brushing, flossing) | Mechanical disruption of plaque biofilm |
| Fissure sealants | Physical barrier over occlusal pits/fissures |
| Chlorhexidine | Antimicrobial plaque suppression |
| Saliva substitutes / stimulants | In xerostomia (Sjogren's, post-radiation) |
| Xylitol | Non-fermentable sugar; inhibits S. mutans |
A 2024 Cochrane systematic review on water fluoridation (PMID 39362658) confirmed water fluoridation reduces caries in children and adults, supporting its continued use as a public health measure.
- Park's Textbook of Preventive and Social Medicine
Treatment
| Stage | Treatment |
|---|---|
| White spot / initial enamel lesion | Fluoride application, remineralization, dietary counseling |
| Cavitated enamel/dentin caries | Excavation + restoration (composite, amalgam, glass ionomer cement) |
| Reversible pulpitis | NSAIDs ± acetaminophen; dental referral |
| Irreversible pulpitis | Root canal therapy (endodontic treatment) or extraction |
| Periapical abscess | Incision and drainage + antibiotics (amoxicillin first-line); root canal or extraction |
The American Dental Association recommends NSAIDs over opioids for dental pain, given the more favorable balance between pain relief and harm. Antibiotics do not reliably reduce pain in irreversible pulpitis without systemic signs of infection.
- Tintinalli's Emergency Medicine, 8th Ed.
Complications and Sequelae
- Pulpitis (reversible → irreversible)
- Pulp necrosis
- Periapical abscess / periradicular periodontitis
- Ludwig's angina (deep space infection - life-threatening)
- Osteomyelitis of the jaw
- Cavernous sinus thrombosis (rare)
- Tooth loss and edentulism (one of the leading causes globally of years lived with disability)
Epidemiology
Dental caries is among the most prevalent non-communicable diseases worldwide. The 2024 global meta-analysis on early childhood caries (PMID 39049051) confirms early childhood caries (ECC) remains a major global public health burden, particularly in low- and middle-income countries. Dental caries and periodontal disease are the two leading causes of tooth loss globally.
- Park's Textbook of Preventive and Social Medicine
This is a shared conversation. Sign in to Orris to start your own chat.