PCOS
Reading File
Finding Sources
Searching PubMed
"polycystic ovary syndrome"[MeSH Terms] AND management
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Polycystic Ovary Syndrome (PCOS)
Definition
PCOS is a heterogeneous endocrine disorder defined by the Rotterdam criteria - any two of the following three features, after exclusion of other causes:
- Oligo-ovulation or anovulation (manifested as oligomenorrhea or amenorrhea)
- Hyperandrogenism - clinical (hirsutism, acne, androgenic alopecia) or biochemical (elevated testosterone/DHEAS)
- Polycystic ovaries on ultrasound (≥12 follicles 2-9 mm per ovary, or ovarian volume >10 mL)
- Goldman-Cecil Medicine, p. 2560; Berek & Novak's Gynecology, p. 2050
Epidemiology
-
Affects 6-12% of women of reproductive age - the most common endocrine abnormality in this group
-
No obvious geographic or ethnic differences in prevalence
-
Typically first presents at puberty
-
>50% develop type 2 diabetes by age 40
-
Obesity both contributes to and is worsened by PCOS; rising obesity prevalence is increasing PCOS prevalence
-
Goldman-Cecil Medicine, p. 2560; Robbins & Kumar Basic Pathology, p. 731
Pathophysiology
The hypothalamic-pituitary unit is structurally intact but functionally deranged:
- Insulin resistance and compensatory hyperinsulinemia are central features, present across all racial/ethnic groups
- Hyperinsulinemia stimulates ovarian androgen production (theca cell stimulation)
- Abnormal LH:FSH ratio - LH is elevated, FSH relatively low, preventing dominant follicle selection and ovulation
- Arrested follicular development leads to multiple small subcortical cysts (not true cysts - they are atretic follicles)
- CYP17 and CYP19 dysregulation contribute to excess androgen biosynthesis
- The resulting excess androgens undergo peripheral aromatization to estrogens, which provide inappropriate positive feedback to the hypothalamus, perpetuating the cycle
- Insulin-like growth factors (IGFs) within the ovary amplify the derangement
Gross/histology (Robbins): Ovaries are usually twice normal size, studded with subcortical cysts 0.5-1.5 cm in diameter. Histology shows:
- Thickened, fibrotic ovarian capsule
- Cystic follicles lined by granulosa cells
- Hyperplastic luteinized theca interna
- Conspicuous absence of corpora lutea (due to anovulation)
A severely affected subset shows hyperthecosis - marked increase in androgen-producing cells in stromal, hilar, and thecal regions - with extreme obesity, acanthosis nigricans, severe hirsutism, and marked hyperinsulinemia.
- Robbins & Kumar Basic Pathology, pp. 733-737; Goldman-Cecil Medicine, p. 2560
Clinical Manifestations
| Feature | Notes |
|---|---|
| Menstrual irregularity | Oligomenorrhea, amenorrhea, or irregular/heavy bleeding |
| Hirsutism | Most common androgen excess sign |
| Acne | Androgenic |
| Androgenic alopecia | Female pattern hair loss |
| Obesity | Present in ~50-60%, but PCOS occurs in normal-weight women too |
| Infertility | Most common cause of anovulatory infertility |
| Acanthosis nigricans | Marker of severe insulin resistance |
The classic triad is amenorrhea + hirsutism + obesity, but significant variability exists - some patients are normal weight, not hirsute, and present only with irregular bleeding.
Diagnosis
Step 1 - Exclude other causes before applying Rotterdam criteria:
- Pregnancy
- Hypothyroidism / hyperthyroidism
- Hyperprolactinemia
- Non-classical congenital adrenal hyperplasia (17-OHP stimulation test)
- Cushing syndrome
- Androgen-secreting tumor (adrenal or ovarian)
- Hypothalamic/pituitary disorders
Step 2 - Laboratory workup:
- Total and free testosterone, DHEAS
- LH, FSH (LH:FSH ratio >3 is supportive but not required)
- Fasting glucose, HbA1c, oral glucose tolerance test
- Fasting lipid panel
- TSH, prolactin (to exclude other causes)
- 17-hydroxyprogesterone (if adrenal hyperplasia suspected)
Step 3 - Pelvic ultrasound for ovarian morphology
Note: "Elevated LH:FSH ratios and hyperinsulinemia are not required for either diagnosis or treatment." - Berek & Novak's Gynecology, p. 2050
Evaluation Algorithm (Dermatology - Fitzpatrick/Bolland):
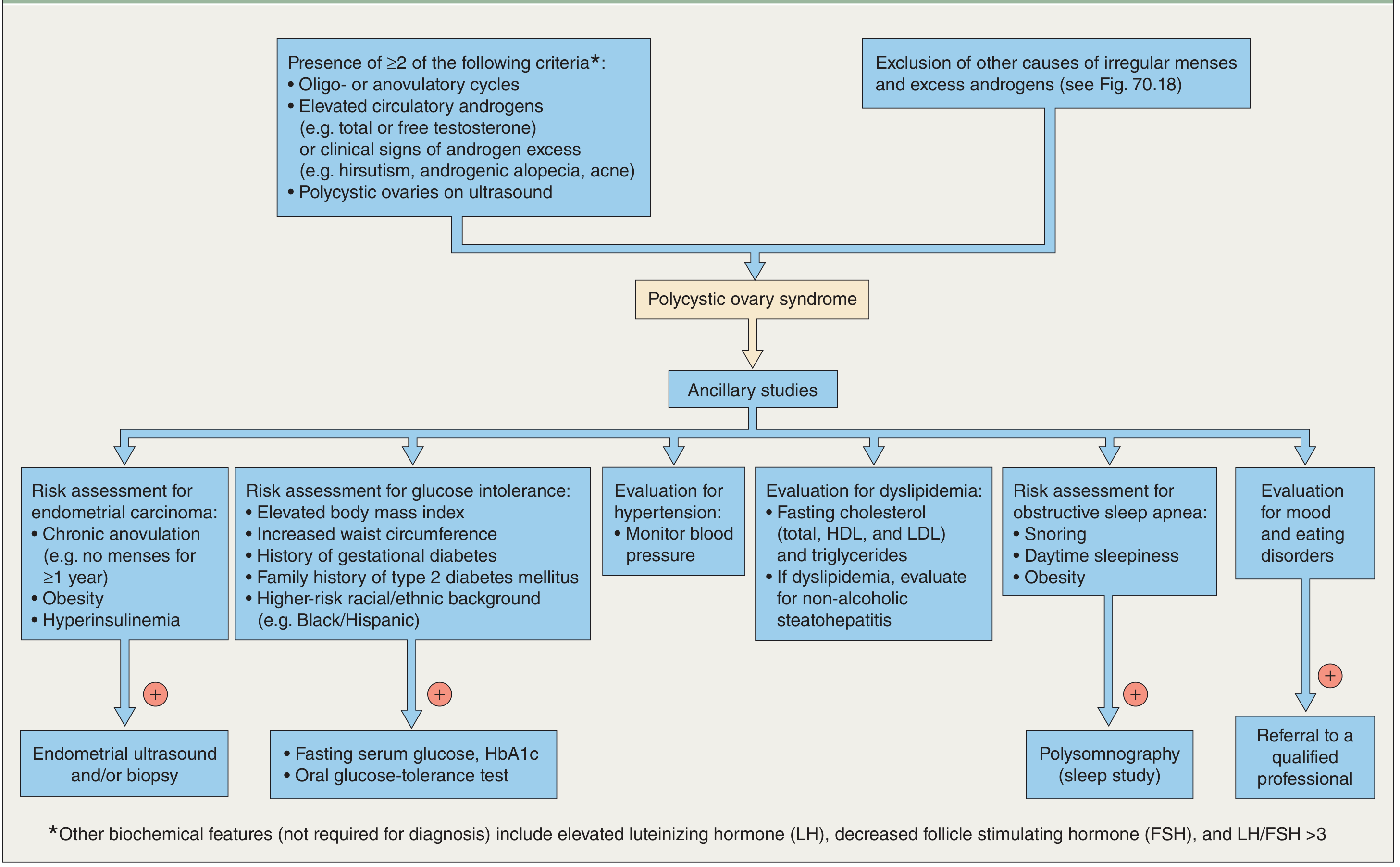
Long-Term Risks
| Complication | Mechanism |
|---|---|
| Type 2 diabetes | Insulin resistance; >50% by age 40 |
| Endometrial hyperplasia/carcinoma | Chronic anovulation = unopposed estrogen |
| Cardiovascular disease | Dyslipidemia, hypertension, insulin resistance |
| Metabolic syndrome | Central obesity, dyslipidemia, HTN, hyperglycemia |
| Obstructive sleep apnea | Associated with obesity and hyperandrogenism |
| Mood/eating disorders | Screening recommended |
| Pregnancy complications | Higher rates of GDM, preeclampsia, preterm birth (see PMID 38965226) |
Treatment
Treatment is individualized based on the patient's primary concern.
1. Lifestyle Modification (first-line for all)
- Even 5% weight loss improves menstrual regularity, androgen levels, and pregnancy rates
- Decrease daily caloric intake by ~500 kcal + regular physical exercise
- Improves both reproductive and metabolic abnormalities
2. Not Desiring Pregnancy
Goal: endometrial protection + symptom management
| Indication | Treatment |
|---|---|
| Cycle regulation / endometrial protection | Combined OCP (first-line) |
| If OCP contraindicated | Cyclic progesterone: medroxyprogesterone acetate (MPA) 5-10 mg/day × 10-14 days/month |
| Minimum: prevent endometrial hyperplasia | Progesterone withdrawal bleed ≥4×/year |
| Hirsutism/acne | OCP ± anti-androgens (spironolactone) |
| Insulin resistance / metabolic | Metformin 1500-2000 mg/day (improves insulin sensitivity, reduces androgens, may restore ovulation in 60-70%) |
3. Desiring Pregnancy - Ovulation Induction
First-line agents (preferred over metformin for ovulation induction):
Letrozole (aromatase inhibitor) - preferred first-line
- 5 mg on days 3-7 of cycle
- Mechanism: blocks estrogen synthesis → removes negative feedback → increased GnRH/FSH → follicle development
- Shorter half-life (48 hr) vs clomiphene (2 weeks), fewer side effects
Clomiphene citrate - 50 mg on days 3-7
- Mechanism: blocks hypothalamic estrogen receptors → increased GnRH pulsatility → FSH rise → follicular development
- 60-85% of PCOS women will ovulate; 15-20% pregnancy per cycle; ~50% pregnant by 6 months
Metformin - less effective for ovulation induction than letrozole/clomiphene, but useful adjunct especially with insulin resistance
Second-line/specialist-directed:
- Exogenous gonadotropins + hCG
- Laparoscopic ovarian drilling (diathermy or laser) - achieves unifollicular ovulation; reserved for those who fail medical therapy; carries risk of adhesions
Overall, ~75-80% of women conceive with letrozole or clomiphene therapy.
- Goldman-Cecil Medicine, pp. 2560-2563; Berek & Novak's Gynecology, pp. 2638-2651
Recent Evidence Updates
Two recent meta-analyses worth noting:
-
GLP-1 receptor agonists in PCOS with obesity (PMID 39178623): Meta-analysis (2024) confirms GLP-1 agonists (e.g., semaglutide, liraglutide) are effective for weight loss and hormonal regulation in PCOS women with obesity - an emerging treatment option beyond metformin.
-
Lifestyle interventions in PCOS (PMID 39861440): Systematic review (2025) reinforces lifestyle modification as a foundational treatment, improving metabolic and reproductive outcomes.
-
Pregnancy outcomes in PCOS (PMID 38965226): Systematic review/meta-analysis (2024) confirms significantly increased risk of gestational diabetes, preeclampsia, preterm birth, and miscarriage - counseling before fertility treatment is essential.
Sources: Goldman-Cecil Medicine International Edition (pp. 2560-2563) | Berek & Novak's Gynecology (pp. 2050-2651) | Robbins & Kumar Basic Pathology (pp. 731-737) | Dermatology 5e (Bolland) | Textbook of Family Medicine 9e
PMOS
Asking for Preferences
Searching the Web
PCOS renamed PMOS polycystic ovary syndrome new name 2025 2026
Searching PubMed
"polycystic ovary syndrome" rename terminology
You're absolutely right - this is very recent news. PCOS was officially renamed PMOS on May 12, 2026 - just 12 days ago.
PMOS: The New Name for PCOS
What Changed?
Polycystic Ovary Syndrome (PCOS) has been officially renamed Polyendocrine Metabolic Ovarian Syndrome (PMOS).
The renaming was announced on May 12, 2026 by a coalition of 56 patient and professional organizations, including the Endocrine Society and the International Androgen Excess and PCOS Society. The decision followed a 14-year consensus process led by researchers at Monash University, with input from more than 22,000 patients and health professionals across six continents, and was published in The Lancet.
Why Was the Name Changed?
The old name "polycystic ovary syndrome" was misleading in two key ways:
- "Polycystic" implied cysts - the small follicles seen on ultrasound are not true cysts, leading to widespread misunderstanding among patients and even clinicians
- "Ovary" implied an ovarian-only disease - when in reality PCOS/PMOS is a full-body, multi-system disorder affecting metabolism, weight, mental health, skin, cardiovascular health, and the reproductive system
The old name contributed to missed diagnoses and inadequate treatment because it framed the condition too narrowly.
What Does the New Name Mean?
| Part | Meaning |
|---|---|
| Poly | Multiple systems affected |
| Endocrine | Hormonal/endocrine disorder (androgens, insulin, LH/FSH) |
| Metabolic | Metabolic disease - insulin resistance, dyslipidemia, T2DM risk |
| Ovarian | Ovaries remain involved (anovulation, follicular arrest) |
| Syndrome | Constellation of features, not a single disease |
The new name better reflects the condition as a complex, chronic hormonal and metabolic disorder affecting over 170 million women worldwide (1 in 8).
What Didn't Change?
Importantly, the renaming is terminology only:
- Diagnostic criteria are unchanged (Rotterdam criteria - still requires 2 of 3: anovulation, hyperandrogenism, polycystic ovarian morphology)
- Treatment protocols are unchanged
- Both names (PCOS and PMOS) will appear in medical records, lab reports, and patient materials during the 3-year transition period
Everything covered in the previous PCOS summary still applies - the science, pathophysiology, management, and long-term risks are identical. The new name simply more accurately describes what the condition actually is.
This is a shared conversation. Sign in to Orris to start your own chat.