Explain all the things about the white blood cells and red blood cells in complete blood count from different books
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
I now have comprehensive information from multiple textbooks. Let me compose a thorough, well-organized answer.
Complete Blood Count (CBC): White Blood Cells & Red Blood Cells
Synthesized from: Histology: A Text and Atlas with Correlated Cell and Molecular Biology; Henry's Clinical Diagnosis and Management by Laboratory Methods; Rosen's Emergency Medicine; Fitzpatrick's Dermatology; Sabiston Textbook of Surgery; Smith and Tanagho's General Urology
What is a CBC?
A Complete Blood Count (CBC) is one of the most commonly ordered laboratory test panels. It provides relative numbers and calculations obtained from erythrocytes (RBCs), leukocytes (WBCs), and thrombocytes (platelets) in a blood sample. Modern CBCs are performed by automated blood cell counters using flow cytometry — as a thin stream of suspended cells flows through narrow tubing, light detectors and electrical impedance sensors identify cell types based on their size and electrical resistance. Approximately 10,000 cells are counted per category, making the data highly accurate. Computer-assisted image-processing systems can further analyze cells automatically, though manual light microscopy remains necessary in some cases.
— Histology: A Text and Atlas, p. 728–729
Hematopoiesis — Origin of Blood Cells
All blood cells originate from hematopoietic stem cells (HSC) in the red bone marrow, diverging into two main progenitor lineages:
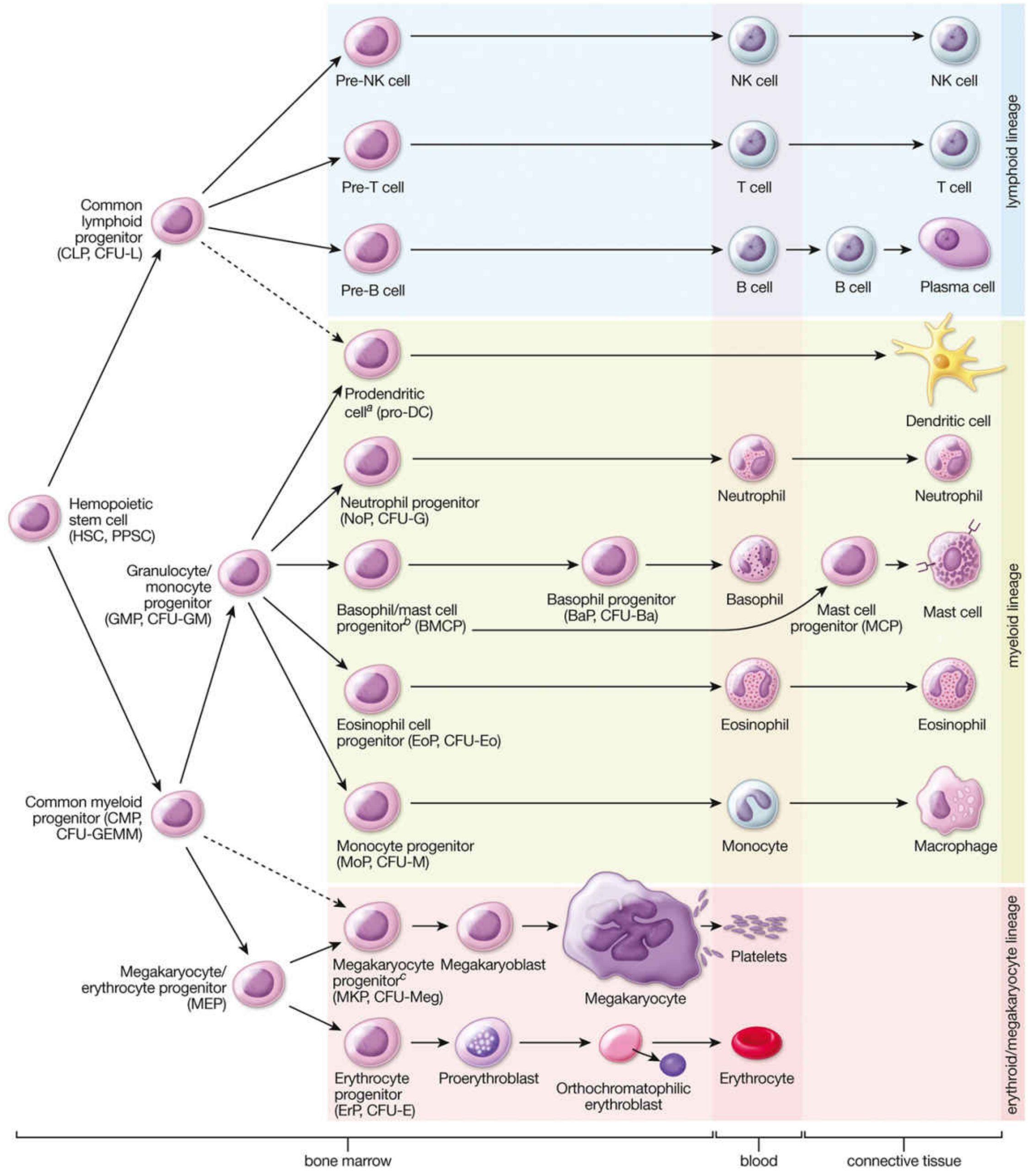
Figure: Hematopoiesis — from hematopoietic stem cells in bone marrow to mature blood and connective tissue cells. — Histology: A Text and Atlas, p. 731–732
| Lineage | Progenitor | Cells Produced |
|---|---|---|
| Myeloid | Common Myeloid Progenitor (CMP/CFU-GEMM) | Neutrophils, Eosinophils, Basophils, Monocytes, Erythrocytes, Platelets |
| Lymphoid | Common Lymphoid Progenitor (CLP/CFU-L) | T cells, B cells, NK cells, Plasma cells |
In adults, erythrocytes, granulocytes, monocytes, and platelets are formed in red bone marrow; lymphocytes are formed in both red bone marrow and lymphatic tissues.
— Histology: A Text and Atlas, p. 731–732
Part 1: White Blood Cells (Leukocytes) in CBC
1. Total WBC Count (Leukocyte Count)
| Parameter | Normal Range | Notes |
|---|---|---|
| WBC count | 4,500–11,000 cells/μL (4.5–11 × 10⁹/L) | Varies by age |
Leukocytosis (elevated WBC) may indicate:
- Infection, burns, bone fractures, other bodily injuries (inflammatory response)
- Strenuous exercise, stress, pregnancy and labor
- Glucocorticoid use (a common non-infectious cause)
- Hyperleukocytosis (>100 × 10⁹ cells/L) — commonly indicates leukemia
- In biliary disease: WBC >18,000/mm³ is classified as Grade II (moderate) acute cholecystitis per 2018 Tokyo Guidelines
Leukopenia (decreased WBC) may indicate:
- Radiation or chemotherapy
- Autoimmune diseases
- Bone marrow disease (aplastic anemia)
- Specific drugs: antipsychotics, antiepileptics, immunosuppressives
- HIV/AIDS
— Histology: A Text and Atlas, p. 728–729; Fitzpatrick's Dermatology, p. 2577; Sabiston Textbook of Surgery
2. WBC Differential (Leukocyte Differential)
The differential counts each type of WBC as a percentage and as an absolute count, providing critical information about immune system status.
"Absolute cell counts can provide valuable information. Low absolute neutrophil count can point to immunodeficiencies associated with neutropenia." — Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 1175
Neutrophils
| Parameter | Normal % | Absolute Count |
|---|---|---|
| Neutrophils (segmented) | 50–70% | 1,800–7,700/μL |
| Band cells (immature neutrophils) | 0–5% | also reported |
- First responders to bacterial infection and tissue injury; they phagocytose pathogens
- Elevated in acute bacterial infections, inflammation, stress response
- Low absolute neutrophil count (ANC) → points to neutropenia; associated with immunodeficiencies
- Hypersegmented neutrophils on smear → folate or vitamin B12 deficiency
- Large vacuoles in neutrophils → seen in Chediak-Higashi syndrome
- Neutrophils migrate out of circulation rapidly after entering from bone marrow, spending most of their life in tissues
— Histology: A Text and Atlas, p. 728; Henry's Clinical Diagnosis, p. 1175; Rosen's Emergency Medicine
Lymphocytes
| Parameter | Normal % | Absolute Count |
|---|---|---|
| Lymphocytes | 20–40% | 1,000–4,800/μL |
- Include T cells, B cells, and NK cells
- At minimum, regardless of age: >1,500 small lymphocytes/mm³ expected
- Because only ~10% of circulating lymphocytes are B lymphocytes, an absolute lymphocyte deficiency primarily reflects T-cell deficiency
- Lymphocytosis with abnormal morphology (increased cytoplasm, prominent nucleoli) → infectious mononucleosis
- Hairy cell lymphocytes → seen in hairy cell leukemia
- Small lymphocytes (<10 μm) are the predominant type assessed on CBC/differential
— Henry's Clinical Diagnosis, p. 1175; Rosen's Emergency Medicine
Monocytes
| Parameter | Normal % | Absolute Count |
|---|---|---|
| Monocytes | 2–8% | 200–900/μL |
- Largest circulating leukocyte; mature into macrophages and dendritic cells in tissues
- Low absolute monocyte count → seen in GATA2 deficiency
- Elevated in chronic infections, inflammatory conditions, and certain malignancies
— Henry's Clinical Diagnosis, p. 1175; Histology: A Text and Atlas, p. 728
Eosinophils
| Parameter | Normal % | Absolute Count |
|---|---|---|
| Eosinophils | 1–4% | 100–400/μL |
- Involved in allergic responses, parasitic infections, and tissue inflammation
- Elevated absolute eosinophil count → seen in:
- Eosinophilic granulomatosis with polyangiitis (Churg-Strauss): a count >1,000 cells/μL helps differentiate this from asthma and atopy
- Omenn syndrome, hyper-IgE syndrome (HIES), and other primary immunodeficiencies
- Eosinophilia is also associated with drug reactions and parasitic infestations
— Fitzpatrick's Dermatology, p. 2577; Henry's Clinical Diagnosis, p. 1175
Basophils
| Parameter | Normal % | Absolute Count |
|---|---|---|
| Basophils | 0–1% | 0–100/μL |
- Least common circulating WBC
- Involved in allergic reactions and hypersensitivity responses (release histamine and heparin)
- Elevated in myeloproliferative disorders (especially chronic myelogenous leukemia)
— Histology: A Text and Atlas, p. 728
3. CBC WBC Findings in Specific Diseases
| Finding on CBC/Smear | Associated Condition |
|---|---|
| Leukocytosis + biliary symptoms, WBC >18,000 | Grade II acute cholecystitis |
| Hyperleukocytosis >100 × 10⁹/L | Leukemia |
| Elevated absolute eosinophils >1,000/μL | Churg-Strauss (eosinophilic granulomatosis with polyangiitis) |
| Hypersegmented neutrophils | Folate / vitamin B12 deficiency |
| Large vacuoles in neutrophils | Chediak-Higashi syndrome |
| Immature WBCs, blasts with Auer rods | Leukemia |
| Increased WBC cytoplasm, prominent nucleoli | Infectious mononucleosis |
| Low ANC | Neutropenia / primary immunodeficiency |
| Low absolute monocytes | GATA2 deficiency |
| Absolute lymphocyte deficiency | Primarily T-cell deficiency |
— Multiple sources (as cited above)
Part 2: Red Blood Cells (Erythrocytes) in CBC
1. RBC Count
| Parameter | Normal Values |
|---|---|
| Men | 4.5–5.9 × 10¹²/L |
| Women | 4.0–5.2 × 10¹²/L |
Polycythemia (elevated RBC count):
- Primary polycythemia: intrinsic bone marrow overproduction (e.g., polycythemia vera, primary familial and congenital polycythemia [PFCP] — genetic)
- Secondary polycythemia: increased erythropoietin (EPO) production in response to chronic hypoxia, high altitude, or EPO-secreting tumor
Anemia (decreased RBC count) causes:
- Blood loss (external/internal hemorrhage) — note: in acute hemorrhage, Hgb/HCT lag behind actual RBC loss due to equilibration time
- Iron deficiency, vitamin B12 deficiency, poor nutrition
- Pregnancy, chronic disease
- Genetic disorders (e.g., sickle cell anemia)
- Autoimmune hemolytic anemia (e.g., Wiskott-Aldrich syndrome)
— Histology: A Text and Atlas, p. 729; Rosen's Emergency Medicine
2. Hemoglobin (Hgb)
| Parameter | Normal Values |
|---|---|
| Men | 13.5–17.5 g/dL (140–180 g/L) |
| Women | 12.0–15.5 g/dL (120–150 g/L) |
- Reflects the erythrocyte's ability to carry oxygen
- Along with hematocrit, it is one of the two major tests used to evaluate for anemia or polycythemia
- Hemoglobin disorders (e.g., sickle cell, thalassemias) are assessed in the context of CBC findings
— Histology: A Text and Atlas, p. 729
3. Hematocrit (HCT) / Packed Cell Volume (PCV)
- Measures the percentage of erythrocyte volume in the blood sample
- Determined by centrifugation of a blood sample
- Approximately 45% of blood volume is cells; 55% is plasma
- A key parameter alongside Hgb for anemia/polycythemia workup
4. Erythrocyte Indices
Four indices are routinely included in CBC to characterize RBC morphology and hemoglobin content:
| Index | What It Measures | Clinical Significance |
|---|---|---|
| MCV (Mean Corpuscular Volume) | Size of RBCs | Microcytic (iron deficiency, thalassemia) vs. Macrocytic (B12/folate deficiency) vs. Normocytic anemia |
| MCH (Mean Corpuscular Hemoglobin) | Amount of Hgb per average RBC | Reduced in hypochromic anemias |
| MCHC (Mean Corpuscular Hemoglobin Concentration) | Hgb concentration in RBC volume | Low in iron deficiency; high in hereditary spherocytosis |
| RDW (Red Cell Distribution Width) | Variation in RBC size (anisocytosis) | High in iron deficiency, mixed anemias |
— Histology: A Text and Atlas, p. 729–730
5. Peripheral Blood Smear — RBC Morphology
The smear provides additional information not captured by counts alone:
| RBC Finding | Associated Condition |
|---|---|
| Schistocytes / fragmented RBCs | Microangiopathic hemolytic anemia (TTP, DIC) |
| Teardrop cells (dacrocytes) | Myelophthisic disease (bone marrow replaced by fibrosis, tumor, granulomas) |
| Nucleated RBCs | Myelophthisic disease, severe hemolysis |
| Howell-Jolly bodies | Functional asplenia |
| Small platelets on smear | Wiskott-Aldrich syndrome |
— Rosen's Emergency Medicine; Henry's Clinical Diagnosis, p. 1175
6. Reticulocyte Count
- While not always part of the standard CBC, reticulocytes (immature RBCs) are often reported alongside
- Elevated reticulocyte count → active erythropoiesis (response to blood loss or hemolysis)
- Low reticulocyte count in the setting of anemia → inadequate bone marrow response (aplastic anemia, nutritional deficiency)
CBC Summary Reference Table
| CBC Component | What It Measures | Key Clinical Meanings |
|---|---|---|
| WBC count | Total leukocytes | Leukocytosis = infection/leukemia; Leukopenia = immunosuppression/bone marrow failure |
| Differential | % of each WBC type | Infection type, immune deficiency, malignancy |
| Neutrophils | Bacterial defense | ↑ infection; ↓ neutropenia/immunodeficiency; bands = immature = left shift |
| Lymphocytes | Adaptive immunity | Lymphocytosis = viral; lymphopenia = T-cell deficiency |
| Monocytes | Phagocytosis/antigen presentation | ↓ GATA2 deficiency |
| Eosinophils | Allergy/parasites | ↑ Churg-Strauss, atopy, parasites, primary immunodeficiencies |
| Basophils | Allergy/mast cell activation | ↑ CML, allergic reactions |
| RBC count | Erythrocyte number | ↑ polycythemia; ↓ anemia |
| Hemoglobin | O₂-carrying capacity | Primary anemia/polycythemia test |
| Hematocrit | % RBC by volume | Primary anemia/polycythemia test |
| MCV | RBC size | Classifies anemia type |
| MCH | Hgb per RBC | Hypochromia assessment |
| MCHC | Hgb concentration | Iron deficiency vs. spherocytosis |
| Platelet count | Thrombocytes | 150,000–400,000/mm³ normal |
Sources:
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 667, 728–732
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 1175
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Fitzpatrick's Dermatology, p. 2577
- Sabiston Textbook of Surgery
- Smith and Tanagho's General Urology, 19th Edition
This is a shared conversation. Sign in to Orris to start your own chat.