Paraganglioma
Reading File
Finding Sources
Searching PubMed
paraganglioma diagnosis treatment
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Finding Sources
I now have comprehensive information to write a detailed, authoritative response. Let me compile everything.
Paraganglioma
Definition and Origin
Paragangliomas (PGLs) are neuroendocrine neoplasms arising from paraganglionic cells of neural crest origin that are associated with the sympathetic and parasympathetic nervous systems. They occur at many anatomic sites throughout the body. Adrenal medullary pheochromocytomas are the most common type, accounting for 80-85% of all cases, with the remainder being extra-adrenal. Approximately 70% of extra-adrenal paragangliomas occur in the head and neck. - Robbins, Cotran & Kumar Pathologic Basis of Disease
Classification by Location
1. Sympathetic (Paravertebral) Paragangliomas
- Arise from paravertebral paraganglia (e.g., the organ of Zuckerkandl)
- Stain positively for chromaffin (catecholamine-producing cells)
- Often functional - secrete catecholamines
- Locations: adrenal medulla (pheochromocytoma), retroperitoneum, pelvis
2. Parasympathetic (Head and Neck) Paragangliomas
- Arise near the great vessels of the head and neck (aortico-pulmonary chain)
- Major subtypes:
- Carotid body tumor - most common head & neck PGL, at carotid bifurcation
- Jugulotympanic (glomus jugulare / glomus tympanicum) - ~50% of temporal bone PGLs
- Vagal paraganglioma - from the ganglion nodosum
- Laryngeal, orbital, nasopharyngeal, and other sites
- Only rarely produce catecholamines (~5%)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Epidemiology
- Rare, slow-growing, usually painless masses
- Most commonly arise in the 5th and 6th decades of life
- About 10% are multifocal (especially in familial cases)
- Approximately 5% secrete catecholamines (head and neck PGLs)
- Incidence is higher at high altitudes (possibly due to chronic hypoxic stimulation)
- Approximately one-third of head and neck PGLs are associated with germline mutations
Genetics and Hereditary Syndromes
This is one of the most genetically determined tumor types in medicine. Over 20 driver genes have been identified.
Succinate Dehydrogenase (SDH) Mutations - Most Common
Loss-of-function mutations in genes encoding SDH subunits (mitochondrial complex II) are the most frequent cause, occurring in both hereditary and sporadic forms. They alter cellular metabolism (a hallmark of neoplasia):
| Gene | Syndrome | Characteristics |
|---|---|---|
| SDHB | PGL4 | Highest malignancy risk (30-50% metastasis rate) |
| SDHC | PGL3 | Head & neck PGLs, low malignancy risk |
| SDHD | PGL1 | Head & neck PGLs, maternal imprinting (only penetrant if inherited from father) |
| SDHAF2 | PGL2 | Also maternally imprinted; skull base/neck |
| SDHA | - | Variable penetrance |
The SDHD and SDHAF2 loci exhibit a unique maternal imprinting pattern - the disease does not manifest when the pathogenic variant is inherited from the mother, but is highly penetrant when inherited from the father. - Goldman-Cecil Medicine
Other Hereditary Associations
- MEN2 (RET mutations) - adrenal pheochromocytoma predominant
- Von Hippel-Lindau (VHL) - pheochromocytoma / paraganglioma
- Neurofibromatosis type 1 (NF1) - ~3% develop catecholamine-secreting tumors (usually solitary adrenal pheochromocytoma)
- All are autosomal dominant
Pathology / Morphology
The carotid body tumor is the prototypical parasympathetic paraganglioma. It rarely exceeds 6 cm, arises close to or envelops the carotid bifurcation, and is red-pink to brown.
Histology (characteristic of all PGLs)
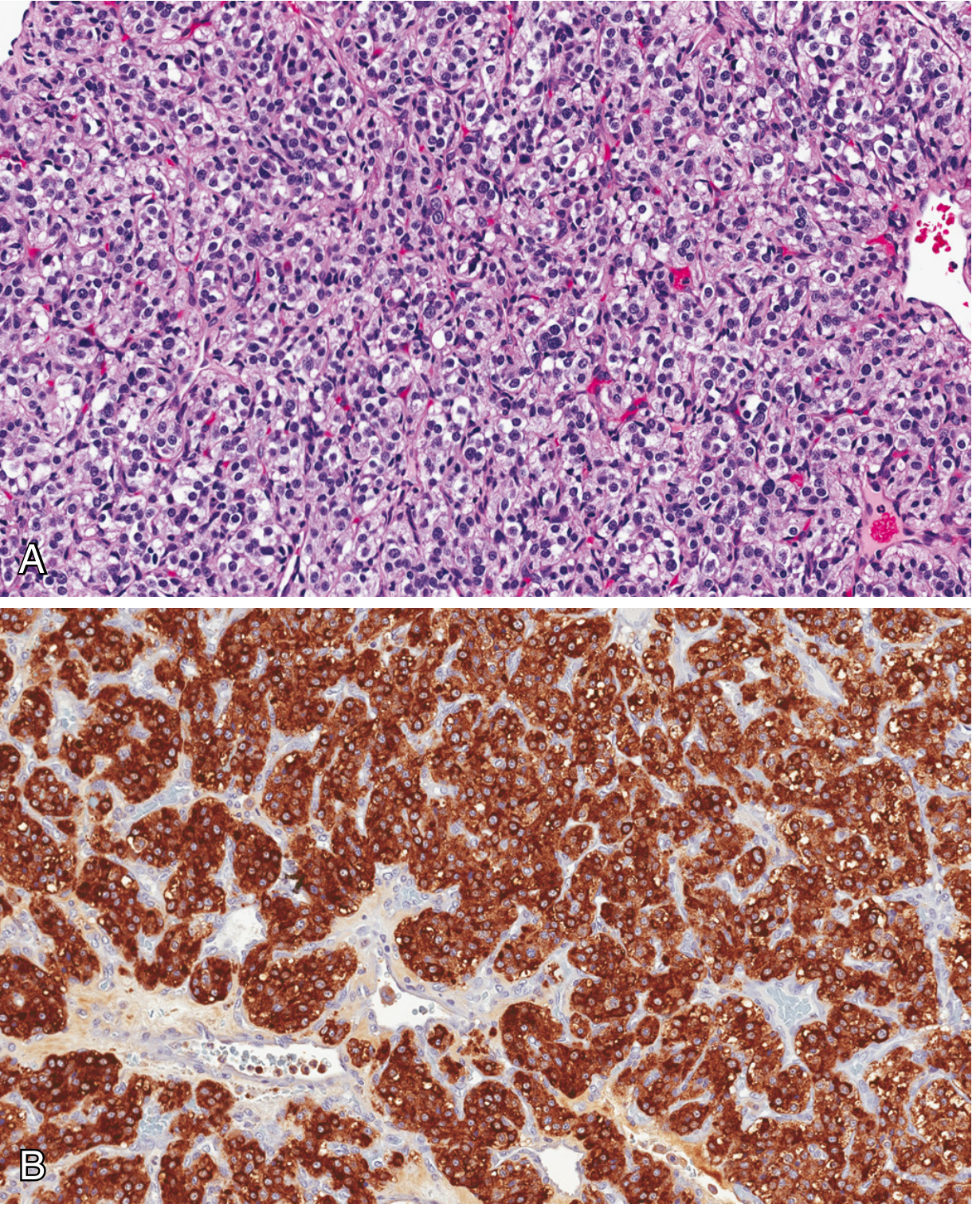
Fig. Carotid body tumor. (A) Low-power H&E showing characteristic zellballen (tumor clusters) separated by delicate vascular septa. (B) Immunohistochemistry showing chromogranin positivity. - Robbins & Cotran Pathologic Basis of Disease
Key histologic features:
- Zellballen pattern - nests of round-to-oval chief cells with abundant clear or granular eosinophilic cytoplasm, surrounded by delicate vascular septa
- Sustentacular cells - spindle-shaped supporting cells at the periphery of nests
- Chief cells: positive for chromogranin, synaptophysin, INSM1, CD56 (neuroendocrine markers)
- Sustentacular cells: positive for S-100 protein
- Little cellular pleomorphism; mitoses scant
- Electron microscopy: well-demarcated neuroendocrine granules (variable)
Important: Histologic features (mitoses, pleomorphism, vascular invasion) do NOT reliably predict malignant behavior. - Robbins, Cotran & Kumar
Clinical Features
Functional PGLs (sympathetic / catecholamine-secreting)
Classic "spell" presentation with:
- Forceful heartbeat, palpitations
- Headache (throbbing)
- Diaphoresis
- Pallor / peripheral vasoconstriction (cool hands/feet)
- Tremor
- Hypertension - sustained (~50%) or paroxysmal (~33%); ~15% normotensive
Spells last ~15-20 minutes and can be precipitated by postural change, medications (metoclopramide, β-blockers, anesthetics, corticosteroids), exercise, or increased intra-abdominal pressure. - Goldman-Cecil Medicine
Non-functional (Parasympathetic) Head and Neck PGLs
Symptoms from mass effect and local invasion:
- Pulsatile tinnitus (glomus tympanicum)
- Cranial nerve palsy (glomus jugulare, vagal PGL)
- Neck mass (carotid body tumor)
- Conductive hearing loss
- Pain
Diagnosis
Biochemical Testing (for functional PGLs)
| Test | Sensitivity | Specificity |
|---|---|---|
| Plasma free metanephrines | ++++ (>95%) | +++ |
| 24h urinary fractionated metanephrines | ++++ | ++ |
| Urinary total metanephrines | +++ | ++++ |
| Plasma catecholamines | +++ | ++ |
Plasma free metanephrines are the most sensitive initial test. Values 3x the upper limit of normal are highly diagnostic. - Harrison's Principles of Internal Medicine, 22nd ed.
Imaging
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CT | ++++ | +++ | First-line; best for bony involvement |
| MRI | ++++ | +++ | Best for soft tissue characterization; "salt-and-pepper" on T2 |
| ¹²³I-MIBG scintigraphy | ++ | ++++ | Functional; identifies extra-adrenal sites |
| ⁶⁸Ga-DOTATATE PET/CT | ++++ | ++++ | High sensitivity; especially head & neck PGLs |
| ¹⁸F-DOPA PET/CT | ++++ | ++++ | Excellent for extra-adrenal and metastatic disease |
- CT with high-resolution parameters is best for assessing bony involvement (temporal bone, skull base)
- MRI best demonstrates soft tissue character and vascular involvement
- Intra-arterial angiography: used pre-embolization; shows enlarged feeding arteries, early intense tumor blush, centripetal arteriolar architecture with AV shunts
Malignancy
All pheochromocytomas and paragangliomas should be considered potentially malignant. The terms "benign" and "malignant" are no longer recommended; "metastatic pheochromocytoma/paraganglioma" is now the preferred terminology when metastases are present. - Robbins & Cotran
- Metastases occur in ~10% of pheochromocytomas and ~20% of paragangliomas
- Common metastatic sites: lymph nodes, bone, liver, lung, peritoneum
- SDHB mutations carry the highest metastatic risk (30-50%)
- Up to 50% of metastatic PGLs are ultimately fatal, largely from infiltrative growth
- Carotid body tumors may metastasize to regional nodes and distant sites despite benign histology
Management
Pre-operative Preparation (Functional PGLs)
- Alpha-adrenergic blockade is mandatory before surgery to prevent hypertensive crisis
- Phenoxybenzamine (non-selective, irreversible) - traditional agent
- Selective alpha-1 blockers (doxazosin, prazosin) increasingly used
- Beta-blockers may be added only AFTER adequate alpha-blockade
- Adequate volume expansion
- Minimum 10-14 days of preparation before surgery
Surgery
- Surgical resection is the primary treatment for all resectable PGLs
- Approach depends on location:
- Carotid body/neck: open surgical excision; laryngoscopic or open approach for laryngeal PGLs (lateral thyrotomy, lateral pharyngotomy)
- Adrenal/retroperitoneal: laparoscopic or open adrenalectomy
- Temporal bone: specialized skull base surgery
- Pre-operative embolization (24-48 hours before surgery) significantly reduces intraoperative blood loss for highly vascular lesions; used as adjunct to surgery
Radiation Therapy
- Used when surgery is inappropriate or incomplete
- PGLs respond to radiation but incompletely
- Stereotactic radiosurgery for skull base/intracranial disease
Metastatic Disease
- ¹³¹I-MIBG therapy (100-300 mCi doses over 3-6 cycles) - treatment of choice for scintigraphically documented metastases
- Somatostatin receptor ligand therapy (PRRT with ¹⁷⁷Lu-DOTATATE)
- Chemotherapy (CVD regimen: cyclophosphamide, vincristine, dacarbazine)
- Targeted therapies (sunitinib, cabozantinib) under investigation
Key Concepts Summary
- 80-85% of all PGLs are adrenal pheochromocytomas; 70% of extra-adrenal PGLs are in the head and neck
- SDH gene mutations (SDHB, SDHC, SDHD, SDHAF2, SDHA) are the most common hereditary cause; SDHB carries the highest malignancy risk
- Zellballen architecture with chief cells (chromogranin+, synaptophysin+) and sustentacular cells (S-100+) is the histologic hallmark
- Histology cannot reliably predict malignancy - only metastasis confirms it
- Plasma free metanephrines are the most sensitive biochemical test
- ⁶⁸Ga-DOTATATE PET/CT and ¹⁸F-DOPA PET/CT have the highest sensitivity and specificity for imaging
- All functional PGLs require alpha-blockade before surgical resection
- Familial PGLs associated with SDHD/SDHAF2 exhibit maternal imprinting
Recent evidence (2024-2026): A 2026 systematic review and meta-analysis (PMID 37455341) compared direct percutaneous puncture versus transarterial embolization for head and neck paragangliomas, showing evolving approaches to preoperative tumor devascularization.
This is a shared conversation. Sign in to Orris to start your own chat.