Define SCOLA for surgery resident
Reading File
Finding Sources
Searching the Web
SCOLA surgery resident definition surgical assessment
Reading File
Searching the Web
SCOLA "Surgical Council on Resident Education" OR "subcutaneous onlay laparo-endoscopic" hernia
Loading Image
Here is a complete definition of SCOLA for a surgery resident:
SCOLA - Subcutaneous Onlay Laparoscopic Approach
SCOLA stands for Subcutaneous Onlay Laparoscopic Approach - a minimally invasive (MIS) anterior technique for simultaneous repair of ventral hernias and diastasis recti, first described by Claus et al. in 2018.
Concept
Traditional repair of midline diastasis recti required open surgery by plastic surgeons (transverse lower abdominal incision + plication + dermolipectomy). SCOLA offers a laparoscopic alternative, particularly suited to patients who do not need dermolipectomy.
Key Technical Points
| Step | Detail |
|---|---|
| Port placement | 3 ports along the Pfannenstiel line: 11 mm midline suprapubic + 2 × 5 mm lateral |
| Working space | Dissection stops at the anterior aponeurosis of rectus abdominis; CO₂ insufflation of the subcutaneous space (up to 10 mmHg) |
| Dissection extent | Cranially to xiphoid, laterally to ribs |
| Umbilicus | Umbilical stalk is transected and re-created at closure |
| Hernia repair | Sac opened, contents reduced, defect closed with running barbed suture; diastasis plicated |
| Mesh | Polypropylene onlay mesh secured with glue, sutures, or tacks |
| Drain | Left in place at end of procedure |
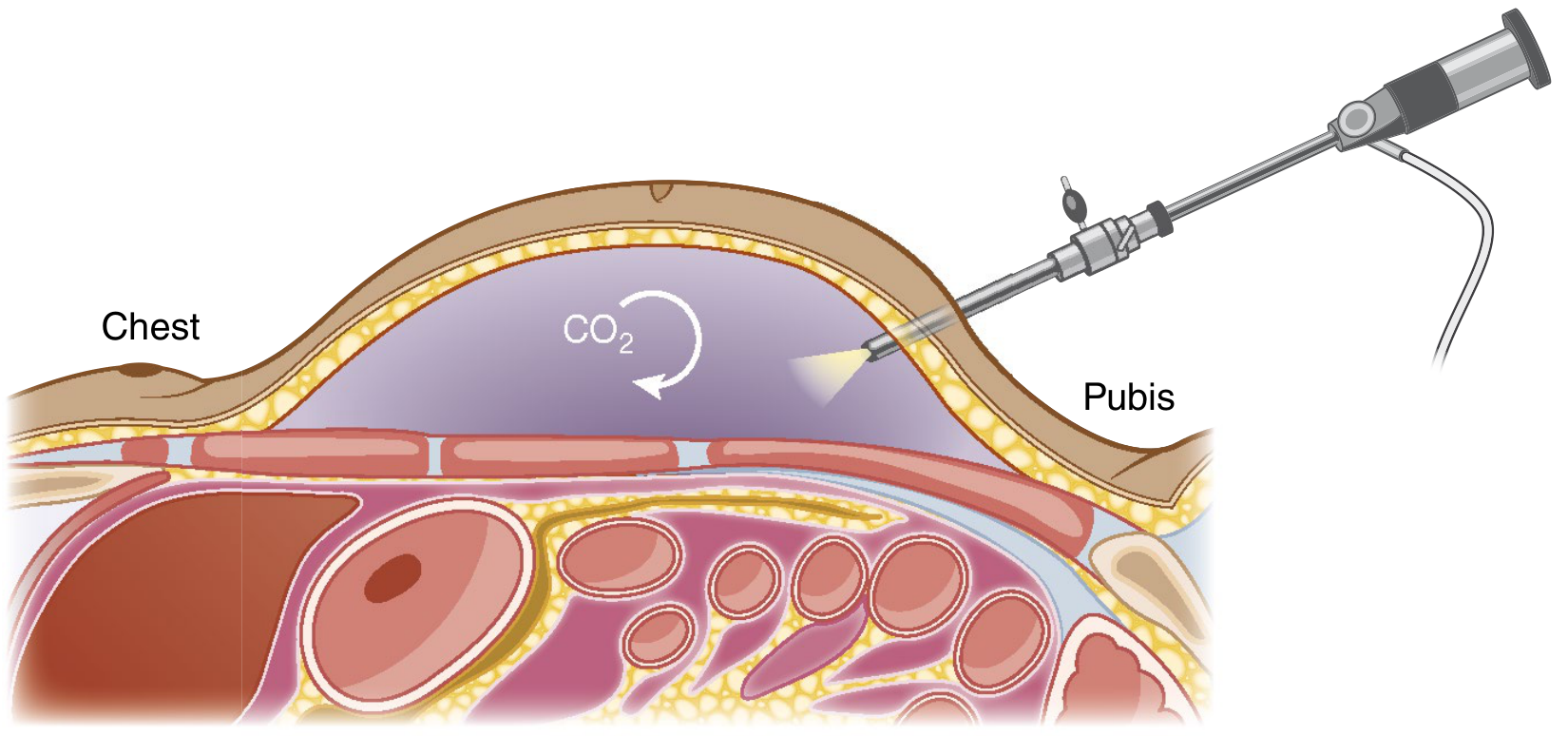
FIGURE: Insufflation of the subcutaneous space during SCOLA. The laparoscope enters via the Pfannenstiel incision and CO₂ creates the working space anterior to the aponeurosis.
Patient Selection
SCOLA is best suited for small defects:
- Hernia defect < 4 cm
- Diastasis recti < 4 cm
- No need for dermolipectomy (excess skin resection)
Complications
- Seroma (most common)
- Wound infection
- Recurrence
Summary
SCOLA = laparoscopic approach working in the subcutaneous plane (above the anterior fascia, below the skin), allowing the surgeon to plicate diastasis + place an onlay mesh + repair a concomitant hernia - all through three small Pfannenstiel-line incisions.
Source: Sabiston Textbook of Surgery - The Biological Basis of Modern Surgical Practice, p. 1655, citing Claus CMP et al. (2018).
Note: You may sometimes see the similar acronym SCORE (Surgical Council on Resident Education), which is a different entity - the national online curriculum for general surgery residency established in 2004. SCOLA and SCORE are unrelated.
Compare SCOLA vs retrorectus (Rives-Stoppa) MIS approach
Finding Sources
Searching PubMed
SCOLA "subcutaneous onlay laparoscopic" ventral hernia diastasis
Searching the Web
SCOLA vs MIS Rives-Stoppa retrorectus hernia repair comparison outcomes
Reading File
Reading File
Reading Article
PMID: 41667727
Reading File
Reading File
Loading Image
I have all the data needed. Here is the full comparison:
SCOLA vs MIS Rives-Stoppa (eTEP Retrorectus) - Head-to-Head Comparison
The Fundamental Difference: Anatomical Plane
| Feature | SCOLA | MIS Rives-Stoppa (eTEP) |
|---|---|---|
| Plane | Subcutaneous - anterior to anterior rectus fascia | Retrorectus - posterior to rectus muscle, anterior to posterior sheath |
| Access | No peritoneal entry; no fascial incision | Posterior rectus sheath incised medially; eTEP = no peritoneal entry |
| Mesh position | Onlay (anterior to fascia) | Sublay (retromuscular) |
1. Anatomy of Working Space
SCOLA
- Working space: the subcutaneous fat layer between skin and the anterior rectus aponeurosis
- CO₂ insufflated at up to 10 mmHg into this space
- Peritoneum and posterior sheath are never breached
- Dissection limited cranially to the xiphoid and laterally to the ribs
MIS Rives-Stoppa (eTEP)
- Working space: the retrorectus space, posterior to the rectus muscle and anterior to the posterior sheath
- Access gained by incising the medial attachment of the posterior sheath at the linea alba
- The eTEP "crossover maneuver" bridges the bilateral retrorectus spaces through the midline preperitoneal plane, creating one continuous space for wide mesh coverage
- Dissection can extend to the costal margin superiorly and space of Retzius inferiorly
2. Operative Technique Comparison
| Step | SCOLA | MIS Rives-Stoppa (eTEP) |
|---|---|---|
| Patient position | Supine | Supine, arms tucked, slight flexion |
| Port placement | 3 ports at Pfannenstiel line (11 mm midline + 2 × 5 mm lateral) | Lateral ports, contralateral side for triangulation; site varies by hernia location |
| Access method | Subcutaneous dissection halted at anterior aponeurosis | Posterior sheath incised at medial linea alba (transabdominal) OR optical entry into retrorectus space (eTEP) |
| Crossover | Not applicable | eTEP requires crossing midline through the preperitoneal space to reach contralateral retrorectus |
| Hernia repair | Sac opened, contents reduced, defect closed with barbed suture | Defect closed with barbed suture; posterior layer closed separately |
| Diastasis | Plicated directly through anterior approach | Linea alba plicated during posterior layer closure |
| Mesh | Polypropylene, onlay position; fixed with glue/suture/tacks | Uncoated macroporous polypropylene, retromuscular; fixation usually not required |
| Umbilicus | Stalk transected and re-created at closure | Preserved (not routinely divided) |
| Drain | Routinely left | Surgeon preference |
3. Hernia Size Indications (Sabiston)
| Defect Size | Preferred Approach |
|---|---|
| < 4 cm + diastasis < 4 cm | SCOLA - ideal candidate |
| 4-8 cm midline | MIS Rives-Stoppa (eTEP) |
| 6-14 cm | MIS TAR (transversus abdominis release) - extension of Rives-Stoppa |
| > 14 cm or >20% domain loss | Open reconstruction |
Key caveat: eTEP retrorectus space is limited laterally by the linea semilunaris. If wider coverage is needed, TAR extends the plane beyond this.
4. Contraindications
| SCOLA | MIS Rives-Stoppa (eTEP) | |
|---|---|---|
| Absolute/relative | Defects > 4 cm; patient needing dermolipectomy | Prior xiphopubic incision (disrupts midline preperitoneal space for eTEP crossover) |
| Relative | Obese patients with thick subcutaneous fat (limits visibility) | Prior preperitoneal dissection (TAPP, prior eTEP) |
| Pregnancy plans | Complex reconstruction should be deferred | Same - avoid in patients planning future pregnancies |
5. Complications Profile
| Complication | SCOLA | MIS Rives-Stoppa |
|---|---|---|
| Seroma | 19-22% (most common; driven by extent of subcutaneous dissection, not mesh per se) | Present but less prominent due to retromuscular space obliteration by mesh |
| SSI | 5% (mesh group only); 0% (no-mesh group) | Lower than open; sublay plane protects from SSI |
| Recurrence | 1.7% (mesh) vs 0% (no mesh) - short follow-up | 4.1-7% at 24 months (open data); MIS comparable |
| Bowel injury | Very low (no peritoneal entry) | Risk with posterior sheath entry (small but present) |
| Nerve injury | Low | Neurovascular bundles at linea semilunaris must be protected |
SCOLA data from Vitiello et al. 2026 meta-analysis (247 patients, 6 studies; mean follow-up only 9.5 months - limited by short follow-up and non-randomized designs).
6. Mesh Considerations
| SCOLA | MIS Rives-Stoppa | |
|---|---|---|
| Position | Onlay - in contact with subcutaneous tissue | Sublay retromuscular - isolated from skin and bowel |
| Fixation needed? | Yes - glue, sutures, or tacks (mesh can migrate in subcutaneous space) | Usually NO - retromuscular space holds mesh by pressure |
| Type | Polypropylene (lightweight) | Uncoated macroporous polypropylene preferred (well-vascularized plane) |
| Hernia-plane evidence | Sublay consistently superior to onlay for SSI and recurrence (meta-analysis) | Retromuscular sublay is the gold-standard plane for open repair |
7. Evidence Summary
| SCOLA | MIS Rives-Stoppa | |
|---|---|---|
| Best evidence | 2026 systematic review/meta-analysis (Vitiello et al., Langenbeck's Arch Surg, PMID 41667727) - 247 patients, moderate quality | Extensive comparative and cohort data; recurrence 4.1-7% at 2+ years |
| Evidence quality | Low-moderate (small, non-randomized, short follow-up) | Moderate-high (multiple RCTs for open; growing MIS data) |
| RCTs | None yet | Several for open RS; eTEP vs open in progress |
8. Decision Framework
Midline hernia + diastasis?
│
Defect < 4 cm AND diastasis < 4 cm?
├─ YES + no dermolipectomy needed → SCOLA
└─ NO
│
Defect 4-8 cm? → MIS Rives-Stoppa (eTEP retrorectus)
│
Defect 6-14 cm? → MIS TAR (extends retrorectus past semilunaris)
│
Prior xiphopubic scar? → Transabdominal retromuscular (not eTEP)
Summary
SCOLA excels in small hernias with diastasis in patients who do not need skin resection. It is technically simpler, avoids fascial incisions entirely, and keeps the surgeon out of the peritoneum - but places mesh in the biomechanically inferior onlay position with a notable seroma rate (~19%).
MIS Rives-Stoppa (eTEP) handles larger defects, places mesh in the superior retromuscular sublay plane (better integrated, no fixation needed, lower SSI), and has substantially more long-term durability data - but requires more complex dissection including the crossover maneuver, and prior xiphopubic scars are a relative contraindication to the eTEP access.
Sources: Sabiston Textbook of Surgery (The Biological Basis of Modern Surgical Practice), pp. 1652-1657; Vitiello et al. SCOLA meta-analysis, Langenbeck's Arch Surg 2026 (PMID 41667727).
This is a shared conversation. Sign in to Orris to start your own chat.