Brachial plexus mri normal anatomy findings diagnostic approch various pathology of brachial plexus and it imaging findings
Reading File
Finding Sources
Finding Sources
Searching the Web
brachial plexus MRI normal anatomy imaging findings pathology diagnostic approach
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the key content and images needed. Now I'll compose the comprehensive response.
Brachial Plexus MRI: Normal Anatomy, Diagnostic Approach, and Pathology
1. Overview and Clinical Relevance
The brachial plexus (BP) presents one of the most diagnostically challenging anatomical regions in the body due to its complex three-dimensional organization, deep location, and proximity to vessels, muscles, and the lung apex. MRI has become the primary imaging modality - it has largely replaced CT myelography for root avulsion diagnosis and is superior to CT for evaluating soft tissue masses, nerve signal, and neoplastic infiltration.
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, p. 186-211
- Grainger & Allison's Diagnostic Radiology, p. 1338-1339
- Bradley and Daroff's Neurology in Clinical Practice, p. 1618-1619
2. Anatomy of the Brachial Plexus
Formation
The brachial plexus is formed by the ventral rami of C5, C6, C7, C8, and T1 (occasionally with prefixed C4 or postfixed T2 contributions). The anatomical organization follows a strict sequence:
| Level | Components | Location |
|---|---|---|
| Roots | C5-T1 ventral rami | Within intervertebral foramina, between anterior and middle scalene muscles |
| Trunks | Upper (C5+C6), Middle (C7), Lower (C8+T1) | Interscalene triangle |
| Divisions | Anterior and posterior from each trunk | Retroclavicular (behind clavicle) |
| Cords | Lateral, Medial, Posterior | Costoclavicular space; named relative to axillary artery |
| Terminal branches | Musculocutaneous, Median, Ulnar, Radial, Axillary | Infraclavicular / axilla |
Key rule: No named branch nerves arise at the division level.
Anatomical Spaces
Three compartments of the thoracic outlet are clinically important:
- Interscalene triangle - between anterior and middle scalene muscles, with first rib as base; contains roots and trunks; most common site of BP compression
- Costoclavicular space (cervicoaxillary canal) - bounded by clavicle superiorly, subclavius anteriorly, first rib and middle scalene posteriorly; contains cords; most common site of venous compression
- Subcoracoid / pectoralis minor space - beneath pectoralis minor tendon and coracoid process; contains cords and proximal terminal branches
The cords are named by their relationship to the axillary artery:
- Lateral cord: anterior divisions of upper + middle trunks → innervates forearm/wrist flexors
- Medial cord: anterior division of inferior trunk → innervates forearm/wrist flexors
- Posterior cord: all three posterior divisions → innervates extensors of forearm/wrist
3. MRI Imaging Anatomy - Normal Findings
MRI Protocol for Brachial Plexus
A standard 1.5T or 3T BP protocol includes 6 key sequences:
| Sequence | Key Role |
|---|---|
| Coronal T1 | Identifies normal anatomy - nerves appear as low-to-intermediate signal structures with surrounding perineural fat; best for identifying gross anatomy and asymmetry |
| Coronal STIR / T2 fat-sat | Suppresses fat signal; nerves show mild intrinsic T2 hyperintensity normally; abnormal hyperintensity = pathology |
| Axial T2 Dixon FS | Cross-sectional nerve anatomy; identifies fascicular pattern |
| Coronal T1 FS post-contrast | Characterizes enhancement (neoplasm, inflammation, neuritis) |
| Axial T1 FS post-contrast | Complements coronal post-contrast views |
| 3D MR neurography (NerveVIEW / SPACE / IDEAL) | Selective nerve visualization; improves conspicuity at root/trunk level |
Normal MRI Appearance
On T1-weighted coronal images, the nerve roots and trunks appear as low-to-intermediate signal linear structures surrounded by bright perineural fat within the interscalene triangle. On T2-weighted images, nerves show a slight intrinsic hyperintensity relative to muscle (fascicular pattern), but significantly less than fluid.
The following figure shows the normal brachial plexus anatomy on coronal T1W and T2W MRI, with nerve roots C5-T1 and the three cords (LC = lateral cord, MC = medial cord, PC = posterior cord) identified:
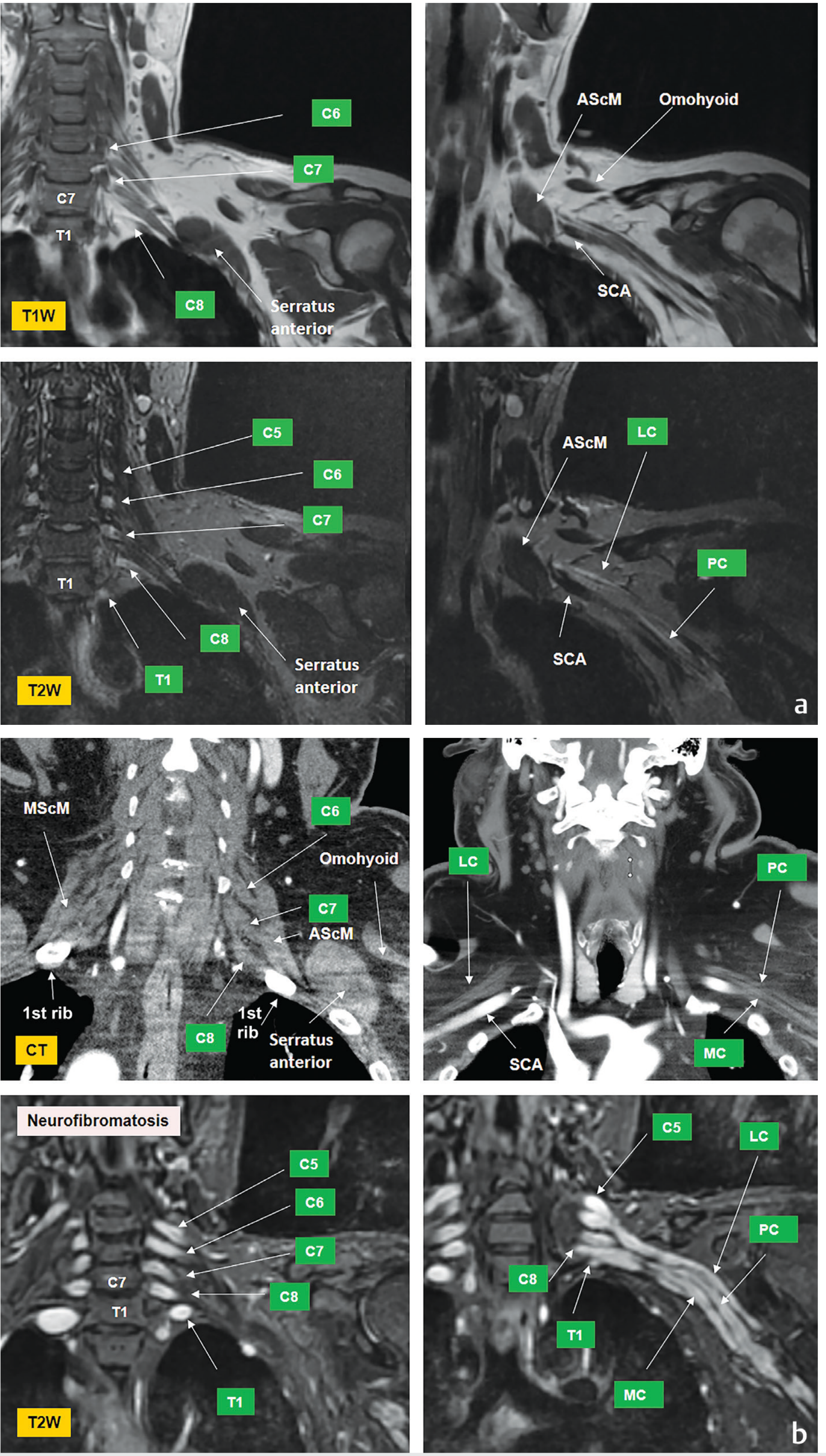
Fig. 6.3 - Normal brachial plexus: Coronal T1W and T2W MRI showing C5-T1 roots, and lateral (LC), medial (MC), and posterior (PC) cords. Note comparison with plexiform neurofibromatosis case in bottom row. - Imaging Anatomy, p. 187-188
The axial CT image below shows the cord-level anatomy, demonstrating the relationship of the lateral cord (LC), posterior cord (PC), and medial cord (MC) to the subclavian artery (SCA) and subclavian vein (SCV) at the retroclavicular level:
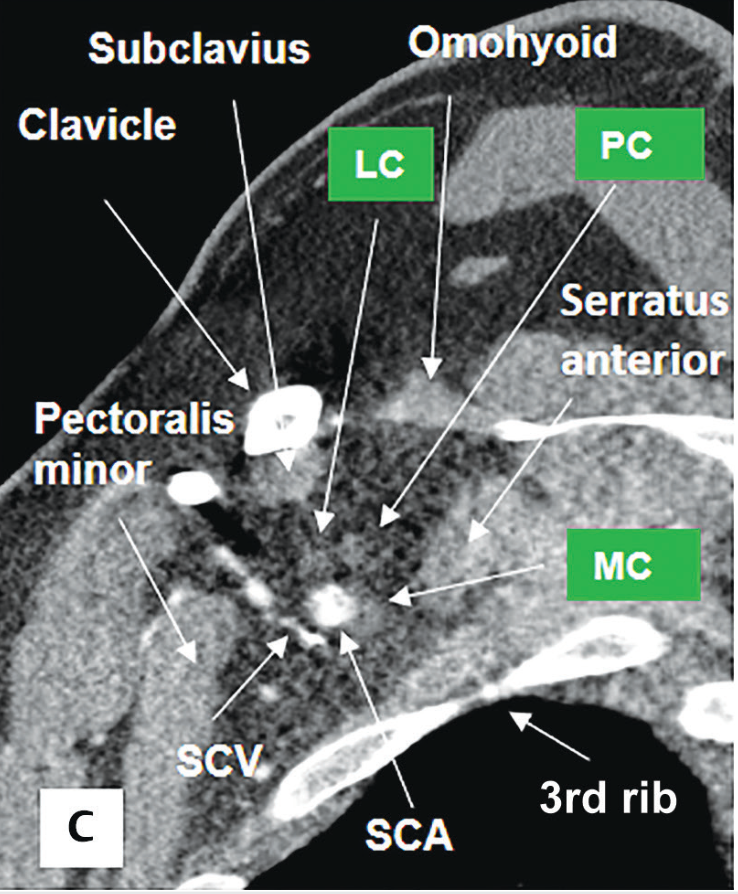
Fig. 6.4c - Normal cord-level anatomy at the costoclavicular space on axial CT. - Imaging Anatomy, p. 188
Normal checklist on MRI report:
- Spinal cord: normal volume and signal
- Roots: symmetric, no T2 hyperintensity, no pseudomeningocele
- Trunks: symmetric caliber within interscalene triangle
- Divisions: normal, retroclavicular
- Cords: symmetric, no enhancement
- Scalene muscles: normal
- Rotator cuff muscles and chest wall: normal
- Vertebral bodies and neural exit foramina: widely patent
- Thoracic outlet spaces: no fibrous band or mass
- Vasculature: no compression
4. Diagnostic Approach to Brachial Plexus Pathology
Localization Framework
Brachial plexopathy is categorized by anatomical level, which has important prognostic and treatment implications:
| Region | Anatomical Level | Typical Pathologies |
|---|---|---|
| Supraclavicular | Roots, trunks (interscalene triangle) | Root avulsion, disc herniation, Pancoast tumor, Parsonage-Turner, NF1 |
| Retroclavicular | Divisions (behind clavicle) | Clavicle fractures, subclavian artery aneurysm |
| Infraclavicular | Cords, terminal branches | Metastatic breast/lung cancer, radiation plexopathy, dislocation, axillary mass |
Pre- vs. Post-Ganglionic Distinction
This is the most critical distinction for surgical planning:
- Pre-ganglionic (proximal to dorsal root ganglion): root avulsion from spinal cord; not surgically repairable; Horner syndrome if C8/T1 involved
- Post-ganglionic (distal to DRG): rupture or neuroma-in-continuity; potentially surgically repairable
MRI with 3D T2 myelographic sequences is the key tool - it shows the intradural nerve roots and identifies pseudomeningoceles (indicating complete root avulsion with dural tear).
Key MRI Diagnostic Parameters to Report
- Pre- vs. post-ganglionic injury location
- Mass vs. non-mass enhancement
- Laterality (unilateral vs. bilateral)
- Segment involved (root / trunk / division / cord / branch)
- Anatomical region and relationship to surrounding structures
- Associated denervation changes in muscles
5. Specific Pathologies and MRI Findings
5.1 Traumatic Brachial Plexus Injury
The most common cause of BP pathology. About 75% involve root avulsion from the cord (pre-ganglionic), with only 25% confined to the distal BP.
Mechanism: Forced traction - shoulder depression with contralateral neck flexion (motorcyclist falling).
MRI findings:
| Finding | MRI Feature |
|---|---|
| Root avulsion | Absent nerve root on 3D T2 myelogram; empty root sleeve |
| Traumatic pseudomeningocele | Fluid-filled CSF pouch at level of avulsed root; bright on T2 "myelogram" sequence |
| Cord edema | Diffuse T2 hyperintensity in cervical cord (from multi-level avulsion) |
| Post-ganglionic rupture | Nerve discontinuity; perineural edema; no pseudomeningocele |
| Neuroma-in-continuity | Fusiform nerve enlargement; T2 hyperintensity; variable enhancement |
| Denervation edema | T2 hyperintensity and swelling of denervated muscles (acute/subacute) |
| Fatty atrophy | T1 bright intramuscular signal in chronically denervated muscles |
The coronal T2 "myelogram" sequence below shows root avulsions at C8 and T1 on the left, with traumatic pseudomeningoceles (arrows):
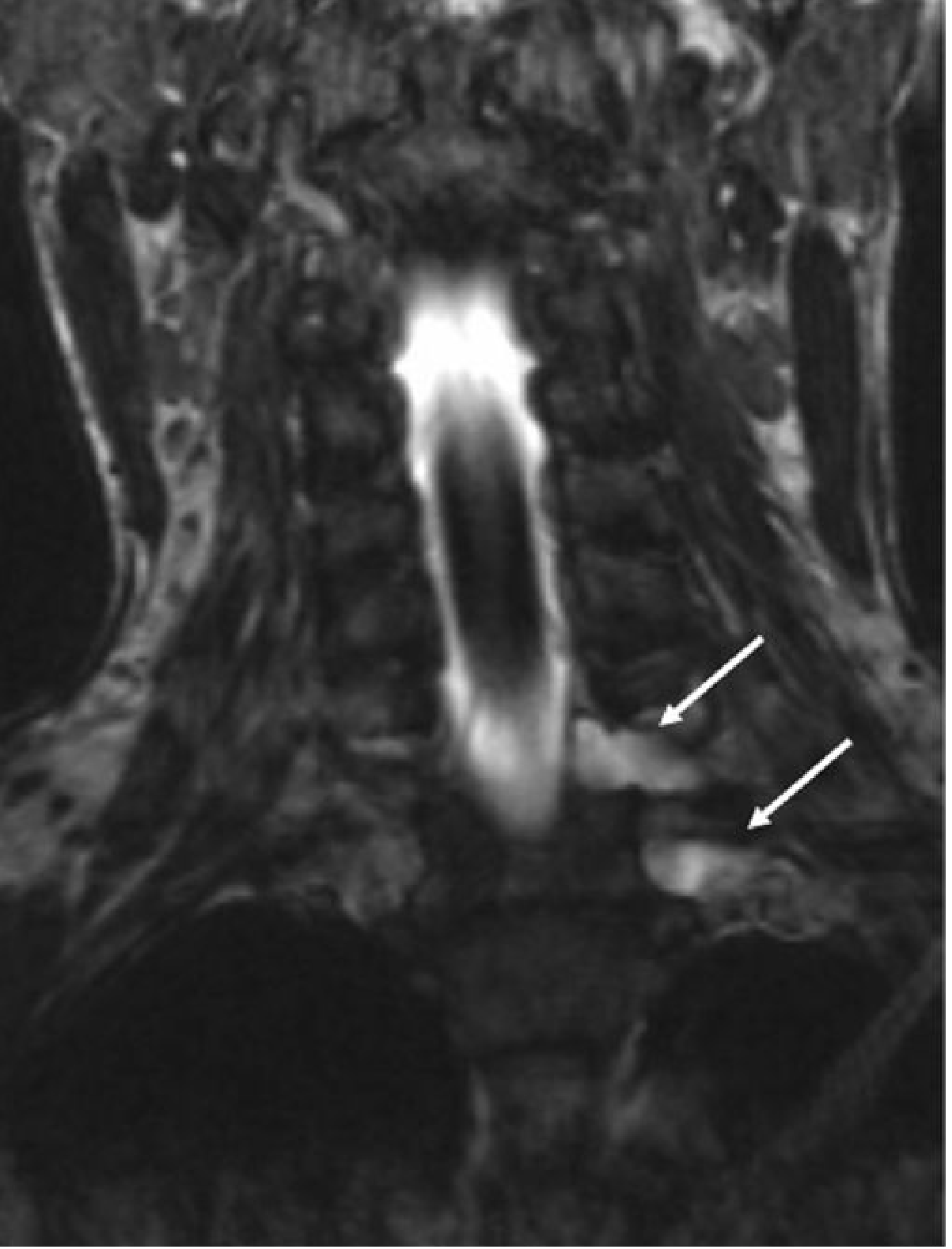
Fig. 52.32 - Coronal T2 'myelogram' sequence showing brachial plexus avulsion at C8 and T1, left side, with traumatic meningoceles (arrows). - Grainger & Allison's Diagnostic Radiology, p. 1339
The sagittal T2 image below shows diffuse cord edema due to multi-level nerve root avulsions:

Fig. 52.31 - Sagittal T2 MRI: Diffuse cervical cord edema due to nerve root avulsions at multiple levels. - Grainger & Allison's Diagnostic Radiology, p. 1339
Clinical note: The presence of intact nerve roots on MRI in a patient with clinical BP injury suggests the injury has occurred more distally, usually in the infraclavicular region.
5.2 Radiation-Induced Plexopathy
The second most important non-traumatic cause. Breast carcinoma accounts for 40-75% of cases, followed by lung carcinoma and lymphoma. Radiation plexopathy is unlikely below 6000 cGy; above this dose, onset ranges from 3 months to 26 years (mean ~6 years).
Mechanism: Endoneural and perineural fibrosis with obliteration of vasa nervorum; direct myelin/axon damage.
MRI findings:
- Diffuse thickening and enlargement of plexus elements within the radiation field - no discrete focal mass
- Mild T2 hyperintensity of affected nerve elements (without mass)
- Variable enhancement (usually mild or absent with fibrosis)
- No regional lymphadenopathy or mass lesion
- Typical distribution: upper plexus (C5/C6) from breast cancer treatment fields
The following MRI demonstrates radiation plexitis in a breast cancer patient - coronal T1W and T2W showing thickening (arrows) of the right brachial plexus cords and divisions:
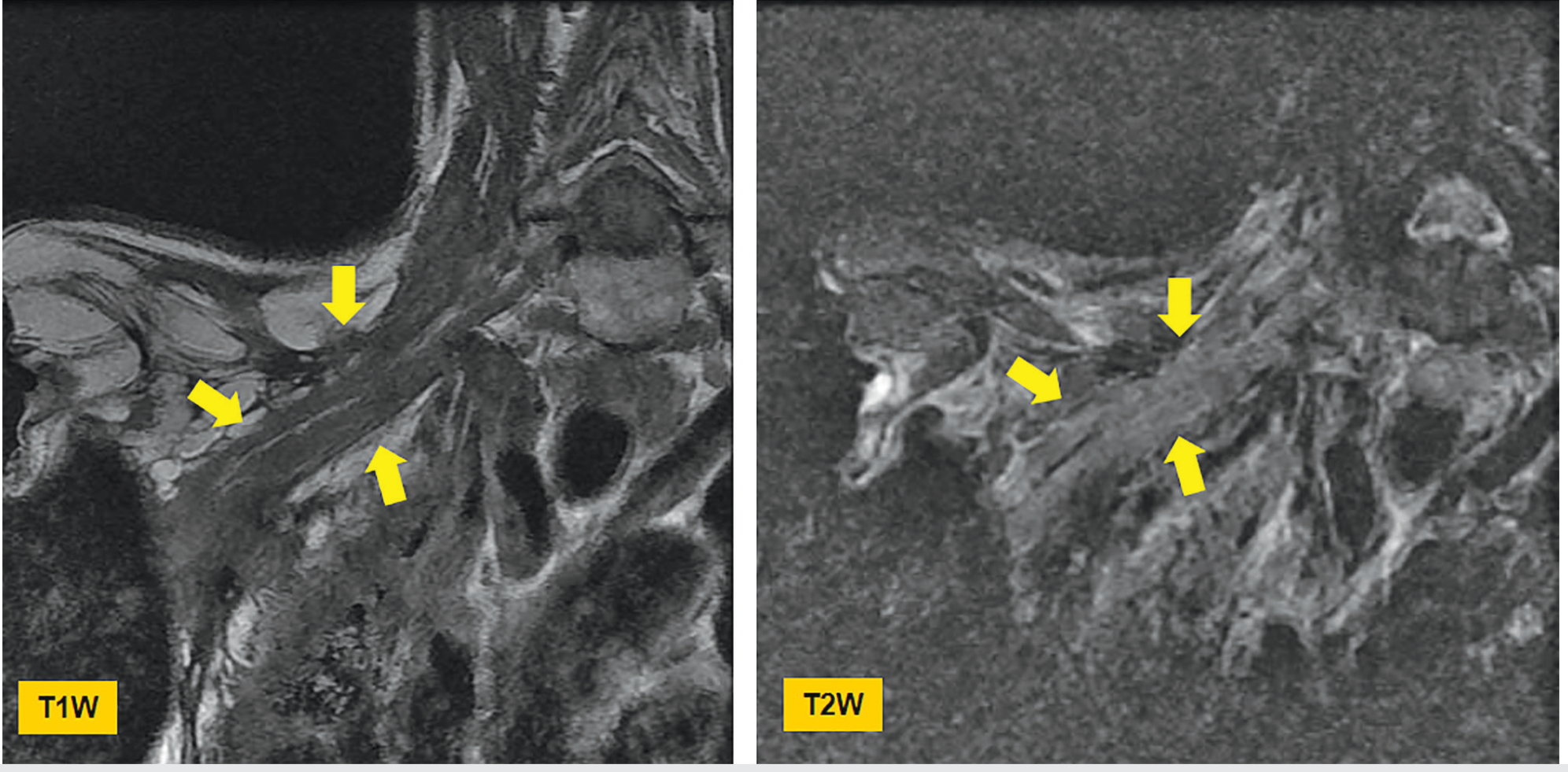
Fig. 6.34 - Radiation plexitis in breast cancer. Coronal T1W and T2W MRI: thickening (arrows) of right brachial plexus cords and divisions due to radiation injury. - Imaging Anatomy, p. 211
Key distinction: Radiation vs. Neoplastic plexopathy
| Feature | Radiation Plexopathy | Metastatic/Neoplastic Plexopathy |
|---|---|---|
| Mass lesion | Absent | Present (adjacent or infiltrating) |
| Distribution | Diffuse, within radiation field | Focal or regional |
| T2 signal | Mild uniform hyperintensity | More focal, intense |
| Enhancement | Minimal | Variable, often avid |
| Upper vs. lower | Tends upper (C5/C6) | Tends lower (C8/T1 - Pancoast) |
| Epidural extension | Rare | May extend into epidural space |
| MR neurography | No intrinsic nerve tumor | May show intrinsic nerve tumor |
| Pain | Less severe | Often severe, characteristic |
5.3 Neoplastic Plexopathy (Metastatic/Infiltrative)
Most commonly from lung cancer, breast cancer, and lymphoma. Due to proximity of lower BP to the lung apex and lymph nodes, lower plexus involvement (C8/T1) predominates.
Pancoast (Superior Sulcus) Tumor: Apical lung cancer invading the brachial plexus from below. Presents with Horner syndrome (C8/T1 sympathetic chain involvement), arm/shoulder pain, and intrinsic hand muscle weakness.
MRI findings:
- Mass lesion adjacent to or infiltrating the plexus
- T2 hyperintensity of involved nerve elements
- Post-contrast enhancement of involved segments
- May show epidural extension - must be reported
- Lymphadenopathy in supraclavicular/infraclavicular regions
- MR neurography can help distinguish intrinsic nerve tumor from extrinsic compression
Hodgkin lymphoma: Infiltrates the upper plexus (C5/C6) in 10-15% of cases.
The coronal T2W images below show acute left brachial plexus injury with T2 hyperintensity of involved nerve roots:
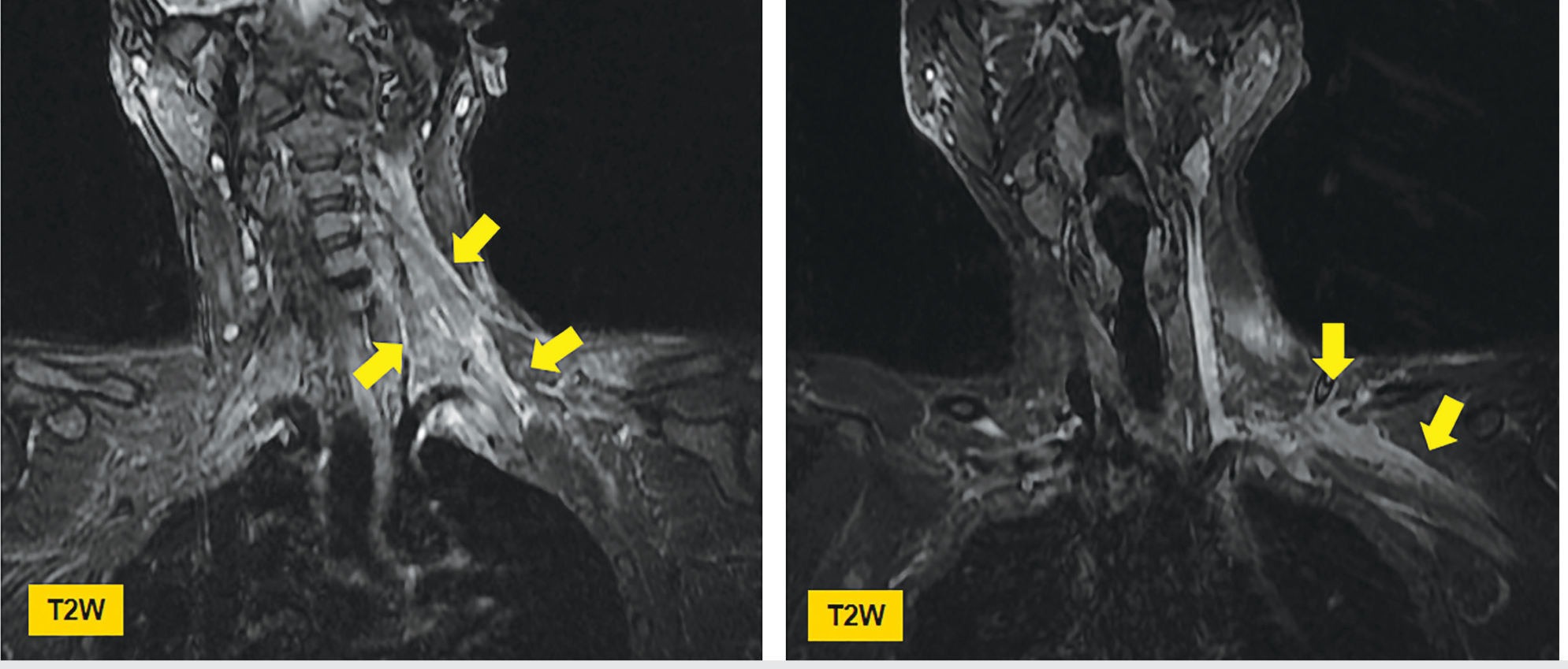
Fig. 6.35 - Acute injury of the left brachial plexus: Coronal T2W MRI showing T2 hyperintense nerve elements (arrows). - Imaging Anatomy, p. 211
5.4 Peripheral Nerve Sheath Tumors
Schwannoma and Neurofibroma are the most common intrinsic BP tumors.
- Schwannoma: Encapsulated, eccentric from nerve; MRI shows T2 hyperintensity, "target sign" on T2 (peripheral hyperintensity with central hypointense zone), avid post-contrast enhancement; can arise from cervical plexus, sympathetic chain, or BP
- Neurofibroma: Non-encapsulated, intrinsic to nerve fascicles; multiple in NF1; same T2/target appearance; fusiform enlargement
- Plexiform neurofibroma: Pathognomonic of NF1; multinodular "bag of worms" appearance on T2; extensive plexus involvement; risk of malignant transformation
- MPNST (Malignant Peripheral Nerve Sheath Tumor): Rapid enlargement; loss of target sign; heterogeneous T2 signal; perilesional edema; avid irregular enhancement; PET-CT shows increased FDG uptake
The bottom panel of Fig. 6.3 (shown earlier) demonstrates the T2W appearance of plexiform neurofibromatosis on coronal MRI - note the markedly enlarged, multi-nodular nerve roots throughout the brachial plexus.
5.5 Parsonage-Turner Syndrome (Neuralgic Amyotrophy)
Acute idiopathic brachial plexus neuritis. Classic presentation: sudden severe shoulder pain followed by weakness and muscle atrophy.
MRI findings:
- Often normal on conventional MRI
- MR neurography may show T2 hyperintensity of involved nerves (suprascapular, long thoracic, axillary nerve most commonly)
- Muscle denervation edema on STIR (acute) or fatty atrophy (chronic) in a non-dermatomal distribution
- No mass lesion - key to distinguish from neoplasm
5.6 Thoracic Outlet Syndrome (TOS)
Compression of neurovascular structures in the thoracic outlet. Neurogenic TOS (most common, 90-95%) involves compression of the lower trunk (C8/T1) by fibrous band, cervical rib, or anomalous first rib.
MRI findings:
- Cervical rib or elongated C7 transverse process on scout images
- Fibrous band: low T1/T2 signal structure extending from anomalous rib tip to normal first rib, stretching/angulating the lower trunk
- Nerve compression, flattening, and T2 signal change at compression point
- Dynamic MRI (abduction-external rotation) may provoke compression
- Associated vascular changes: subclavian artery post-stenotic dilatation / aneurysm (arterial TOS), or subclavian vein thrombosis (venous TOS / Paget-Schroetter)
5.7 Radiation-Related Changes - Summary Table
| Pathology | Key MRI Feature | Differentiator |
|---|---|---|
| Root avulsion | Empty root sleeve; pseudomeningocele | 3D T2 myelogram |
| Radiation fibrosis | Diffuse nerve thickening, no mass, minimal enhancement | History; upper plexus |
| Metastatic infiltration | Focal mass, avid enhancement, epidural spread | FDG-PET, MRN |
| Nerve sheath tumor | T2 target sign, fusiform, encapsulated | Schwannoma vs NF1 |
| Neuralgic amyotrophy | Normal nerve, muscle denervation pattern | Clinical; STIR muscles |
| TOS | Fibrous band / cervical rib; dynamic compression | Structural compression |
6. Advanced MRI Techniques
MR Neurography (MRN)
Uses surface coils, fat suppression, and 3D sequences (SPACE, CUBE, IDEAL) to selectively visualize peripheral nerves. High-resolution 3T MRN has become the preferred technique for complex BP evaluation. It can detect both extraneural and intraneural lesions and is especially useful for:
- Distinguishing radiation fibrosis from neoplastic recurrence
- Evaluating peripheral nerve continuity post-trauma
- Planning surgical neurolysis or nerve grafting
Diffusion Tensor Imaging (DTI) / Tractography
Allows non-invasive visualization of nerve fiber tracts and assessment of microstructural integrity. Provides quantitative metrics (fractional anisotropy, apparent diffusion coefficient) that correlate with nerve integrity. Tractography of the BP is a promising but still investigational technique.
3D T2 Myelographic Sequences
The "myelogram" MRI - heavily T2-weighted sequences with CSF as the contrast. Shows intradural nerve roots clearly against bright CSF background. The standard for diagnosing root avulsions and pseudomeningoceles.
7. Denervation Changes in Muscles
Muscle signal changes are often the first indirect clue of BP pathology on MRI:
| Stage | Finding | MRI Sequence |
|---|---|---|
| Acute denervation (days-weeks) | Muscle edema/swelling; T2/STIR hyperintensity | STIR/T2 fat-sat |
| Subacute (weeks-months) | Continued T2 signal; mild volume loss | T2 fat-sat |
| Chronic (months-years) | Fatty atrophy; T1 hyperintensity replacing muscle | T1 |
A non-dermatomal pattern of denervation changes points to plexus (rather than root or peripheral nerve) pathology. Distribution mapping (e.g., supraspinatus + infraspinatus = suprascapular nerve; deltoid + teres minor = axillary nerve) helps localize the injured BP segment.
Sources
- Imaging Anatomy: Bones, Joints, Vessels and Nerves, Vol. 3, pp. 186-212
- Grainger & Allison's Diagnostic Radiology, pp. 1338-1339 (Trauma) and p. 936 (Radiation)
- Bradley and Daroff's Neurology in Clinical Practice, pp. 1618-1620 (Neoplastic/Radiation Plexopathy)
- Current Surgical Therapy 14e, p. 2243-2245 (High-resolution MRN)
- Neuroanatomy through Clinical Cases 3rd ed., p. 370 (Pancoast/Apical tumor MRI)
- Applied Radiology: MRI of the Brachial Plexus - A Practical Review (Vijayasarathi & Chokshi, 2016)
This is a shared conversation. Sign in to Orris to start your own chat.