ACLS BLS
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Here is a comprehensive overview of BLS and ACLS based on authoritative cardiology and emergency medicine textbooks.
Basic Life Support (BLS)
BLS encompasses interventions that can be performed without special equipment — basic airway management, rescue breathing, and manual chest compressions.
BLS Algorithm (Adult Cardiac Arrest)
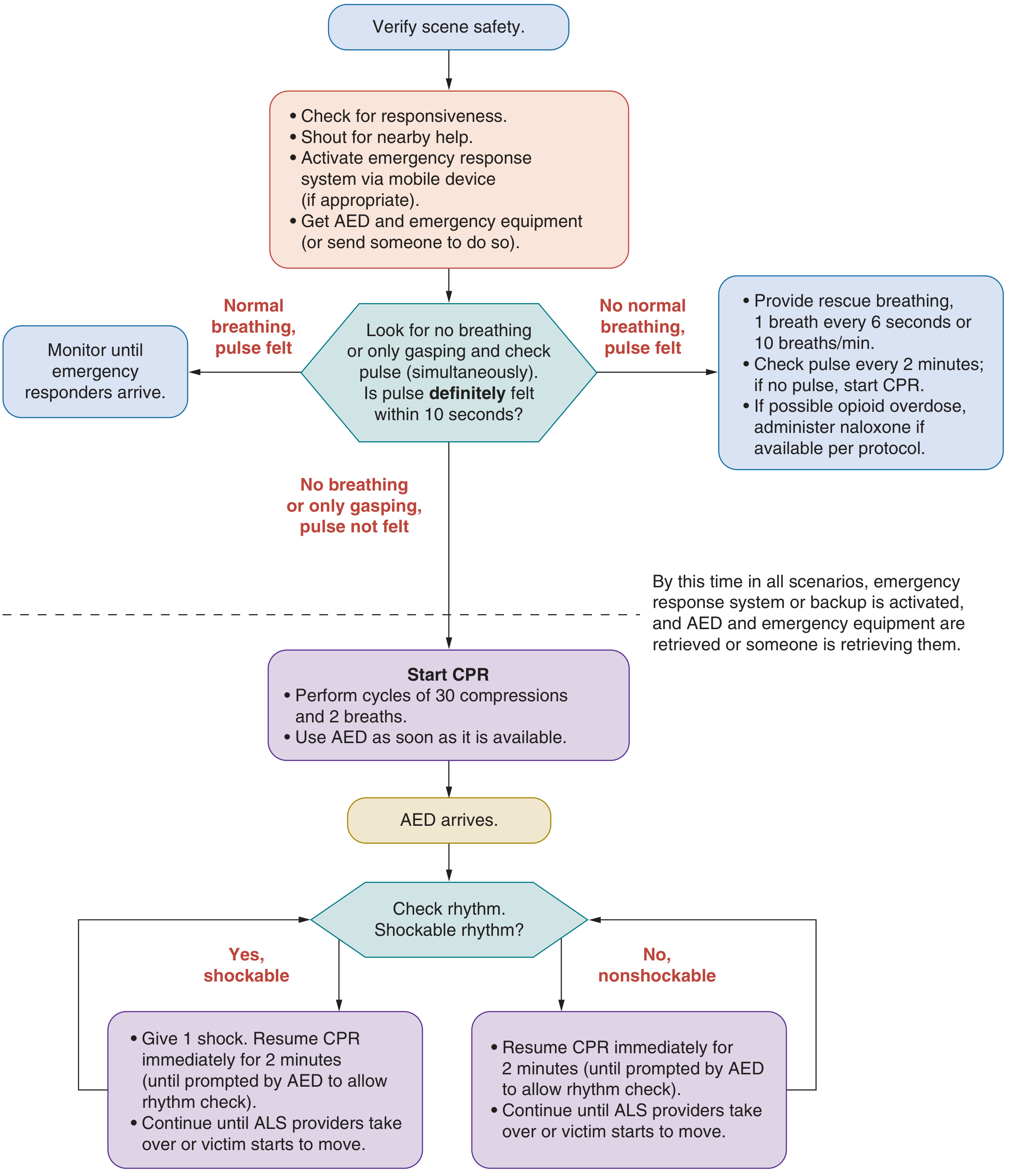
Steps:
- Verify scene safety
- Check responsiveness — shout, stimulate
- Activate emergency response — call 911, get AED
- Assess pulse + breathing simultaneously (<10 seconds)
- Normal breathing, pulse felt → Monitor
- No breathing, pulse felt → Rescue breaths (1 breath every 6 sec; give naloxone if opioid OD suspected)
- No breathing, no pulse → Start CPR
- CPR: 30 compressions : 2 breaths; use AED as soon as available
- AED arrives → Check rhythm → shock if shockable; resume CPR immediately for 2 min
Quality CPR Parameters
| Parameter | Target |
|---|---|
| Compression rate | 100–120/min |
| Compression depth (adults) | ~5 cm (2 in); not >6 cm (2.5 in) |
| Chest recoil | Complete — do not lean on chest |
| Compression:Breath ratio | 30:2 |
| Rescuer switch interval | Every 2 minutes |
AED use should precede CPR in unwitnessed arrests — check rhythm first, shock if indicated. Resuming CPR immediately after a shock (rather than waiting for rhythm recheck) carries a class IIb indication.
Discontinuation of BLS
BLS may be terminated when survival is futile. The Ontario BLS termination rule uses 3 criteria: (1) unwitnessed arrest, (2) three CPR/AED cycles without ROSC, and (3) no shockable rhythm observed.
Advanced Cardiac Life Support (ACLS)
ACLS extends BLS by adding: airway management, IV/IO access, vasopressors/antiarrhythmics, and advanced monitoring.
ACLS Algorithm (Adult Cardiac Arrest)
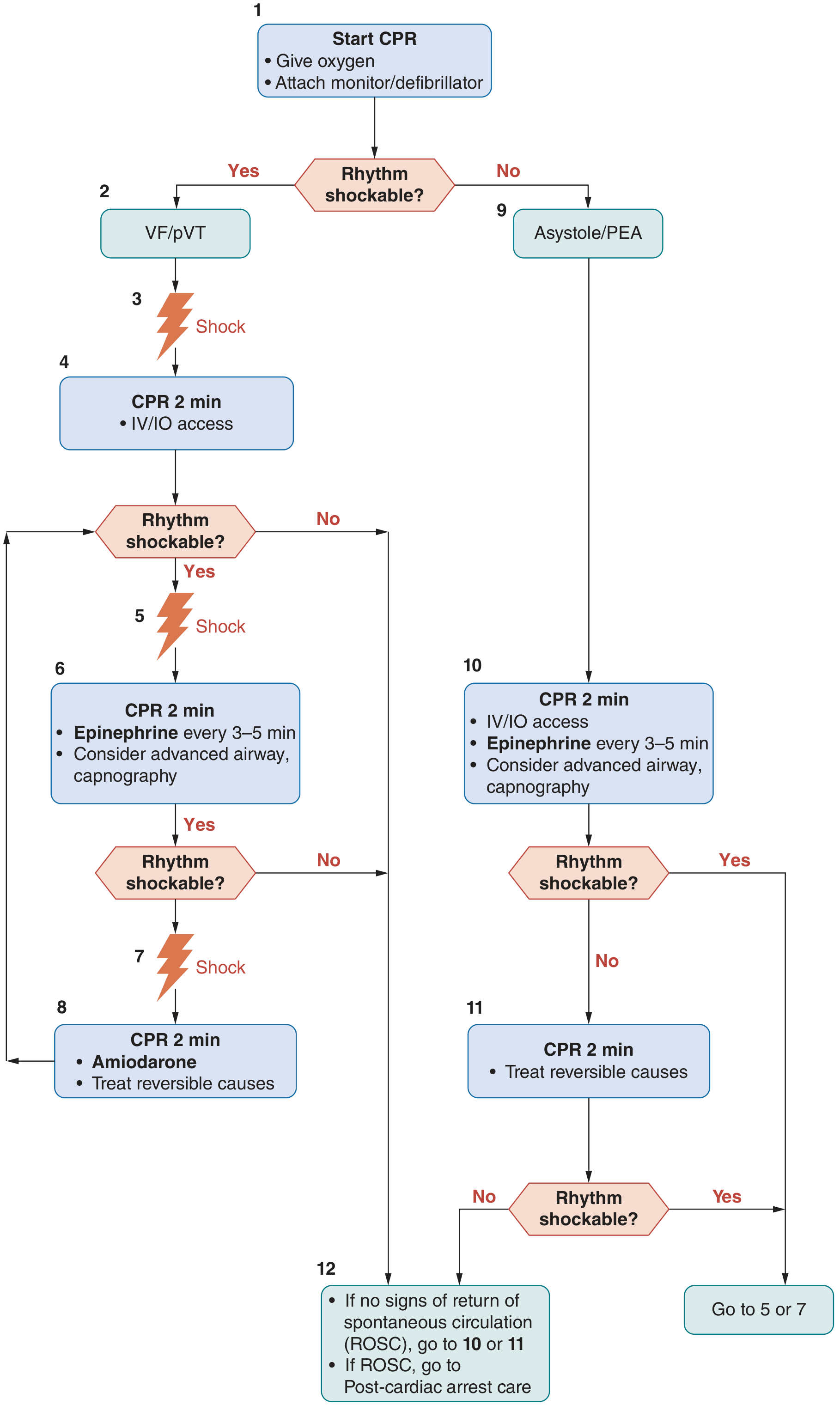
Shockable rhythms (VF / pulseless VT):
- Shock → CPR 2 min + IV/IO access
- If still shockable: Shock → CPR 2 min + Epinephrine q3–5 min ± advanced airway
- If still shockable: Shock → CPR 2 min + Amiodarone + treat reversible causes (H's & T's)
Non-shockable rhythms (Asystole / PEA):
- CPR 2 min + IV/IO access + Epinephrine q3–5 min ± advanced airway
- CPR 2 min + treat reversible causes
- If rhythm becomes shockable → go to shockable arm
Airway Management in ACLS
- Bag-Mask Ventilation (BMV) or advanced airway (ETI or SGA) are both acceptable
- When advanced airway is in place: 1 breath every 6 compressions (10/min)
- SGA preferred over ETI if operator ETI experience is limited
- Each breath: ~600 mL over 1 second
Key ACLS Medications
| Drug | Indication | Notes |
|---|---|---|
| Epinephrine 1 mg IV/IO q3–5 min | PEA/Asystole (use early); VF/pVT (after failed shocks) | Raises diastolic BP → improves coronary perfusion |
| Amiodarone | Shock-refractory VF/pVT | Superior to placebo for survival to hospital admission |
| Lidocaine | Shock-refractory VF/pVT | Alternative to amiodarone |
| Vasopressin | Cardiac arrest | Not superior to epinephrine |
| Atropine | Not recommended for asystole/PEA | Ineffective in cardiac arrest |
| Magnesium sulfate | Torsades de Pointes |
Reversible Causes — The H's & T's
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion (acidosis) | Toxins |
| Hypo/Hyperkalemia | Thrombosis (pulmonary embolism) |
| Hypothermia | Thrombosis (coronary — MI) |
Monitoring During ACLS
- End-tidal CO₂ (EtCO₂): Normal ~35–45 mmHg; optimal CPR yields 15–20 mmHg; ROSC → sudden rise to >35 mmHg. EtCO₂ <10 mmHg after >20 min of resuscitation = marker of futility
- Arterial BP, oximetry, and bedside ultrasound also used
Post-Cardiac Arrest Care (ROSC)
- Target MAP ≥65 mmHg or SBP ≥90 mmHg (fluids + pressors)
- Target SpO₂ 94%, PaO₂ ~100 mmHg, PaCO₂ 35–45 mmHg
- Consider emergent coronary angiography/PCI for suspected coronary occlusion
- Targeted Temperature Management (TTM)
- ICU-level neurological monitoring
Sources: Fuster and Hurst's The Heart, 15th Edition | Roberts and Hedges' Clinical Procedures in Emergency Medicine | Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e
Detailed explanation of BLS And ACLS refer AHA and Harrison
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a detailed explanation of BLS and ACLS synthesized from Harrison's Principles of Internal Medicine 22E and Braunwald's Heart Disease (the definitive AHA-aligned cardiovascular reference), cross-referenced with Fuster & Hurst's The Heart.
BASIC LIFE SUPPORT (BLS)
Definition and Purpose
BLS encompasses the initial interventions that can be performed without special equipment to maintain viability of the central nervous system, heart, and vital organs until definitive return of spontaneous circulation (ROSC) can be achieved. It can be performed by trained laypersons, emergency technicians, and healthcare professionals alike.
"There should be minimal delay between diagnosis and preparatory effort in the initial response and institution of BLS." — Braunwald's Heart Disease
The Chain of Survival (AHA Framework)
Per Harrison's 22E, the out-of-hospital chain of survival includes six links:
| Step | Action |
|---|---|
| 1 | Recognition of SCA + activation of emergency response system |
| 2 | Rapid CPR with emphasis on chest compressions |
| 3 | Defibrillation as early as possible (AED) |
| 4 | Advanced life support (ACLS) |
| 5 | Post-cardiac arrest care |
| 6 | Recovery |
Survival impact: IHCA survival to discharge was 33% when CPR was initiated within the first minute vs. 14% when delayed >1 minute. With VF as initial rhythm: 50% vs. 32%, respectively. (Braunwald's Heart Disease)
The CAB Sequence (AHA Update)
The classic "ABC" (Airway → Breathing → Compressions) has been replaced by "CAB" — Compressions first — because:
- Compressions maintain perfusion without interruption
- Avoids excessive ventilation
- Minimizes delays to circulatory support (Braunwald's)
Step-by-Step BLS Protocol
1. Scene Safety & Recognition
- Verify the scene is safe
- Check for responsiveness (shout, stimulate)
- Gasping respirations and brief seizure activity are common during SCA — do not mistake them for breathing or responsiveness (Harrison's)
2. Activate Emergency Response
- Call 911 (or ask bystander to call); use speaker mode
- If opioid overdose suspected → administer naloxone if available
- Check for pulse (≤10 seconds) — do not delay compressions for prolonged pulse check
3. Chest Compressions (C)
| Parameter | Target |
|---|---|
| Rate | 100–120 compressions/min |
| Depth | ≥5 cm (2 in.); not >6 cm (2.5 in.) |
| Recoil | Full chest recoil between compressions — do not lean |
| Interruptions | Minimize; keep pauses <10 sec |
| Compression:Breath ratio | 30:2 (single or dual rescuer, adults) |
| Two-rescuer (infant/child) | 15:2 ratio retained |
| Switch interval | Every 2 minutes to avoid fatigue |
"Chest compressions generate forward cardiac output with sequential filling and emptying of the cardiac chambers, with competent valves maintaining forward direction of flow." — Harrison's Principles of Internal Medicine 22E
Hands-only CPR: For untrained or remotely trained lay rescuers, compression-only CPR is equally beneficial and more likely to be applied correctly. (Harrison's)
4. Airway (A)
- Tilt head back, lift chin; clear oropharynx of foreign bodies, dentures
- Heimlich maneuver if foreign body obstruction suspected
- In hospitals: Ambu bag ventilation until ETT placed
- Out-of-hospital: mouth-to-mouth while awaiting EMS (Braunwald's)
5. Breathing (B)
- With 30:2 ratio — deliver 2 breaths between every 30 compressions
- Each breath: ~600 mL tidal volume over 1 second
- Avoid excessive ventilation (raises intrathoracic pressure, reduces venous return)
6. Defibrillation (AED)
- Apply AED as soon as available — AED use should precede CPR check in unwitnessed arrests
- AED analyzes rhythm and advises shock for VF/pulseless VT
- Chest compressions continue while defibrillator charges
- On shock delivery: resume CPR immediately for 2 min before next rhythm check
- First shock: 200 J biphasic waveform (Harrison's)
- If shockable rhythm persists → repeat maximal energy shock every 2 min cycle
"When arrest is witnessed, use of AEDs by lay responders can improve cardiac arrest survival rates." — Harrison's 22E
BLS Algorithm (AHA, from Fuster & Hurst's The Heart)
Discontinuation of BLS
The Ontario BLS termination rule (3 criteria):
- Unwitnessed arrest
- Three CPR/AED cycles without ROSC
- No shockable rhythm observed
ADVANCED CARDIAC LIFE SUPPORT (ACLS)
Definition
ACLS is the next resuscitative level after BLS, designed to:
- Restore cardiac rhythm to one that is hemodynamically effective
- Optimize ventilation
- Maintain and support the restored circulation
"Implementation of ACLS is not intended to suggest an abrupt cessation of BLS activities, but rather a transition from one level of activity to the next." — Braunwald's Heart Disease
ACLS adds: IV/IO access, advanced airway, vasopressors, antiarrhythmics, and physiologic monitoring.
ACLS Algorithms by Rhythm
A. Shockable Rhythms: VF / Pulseless VT
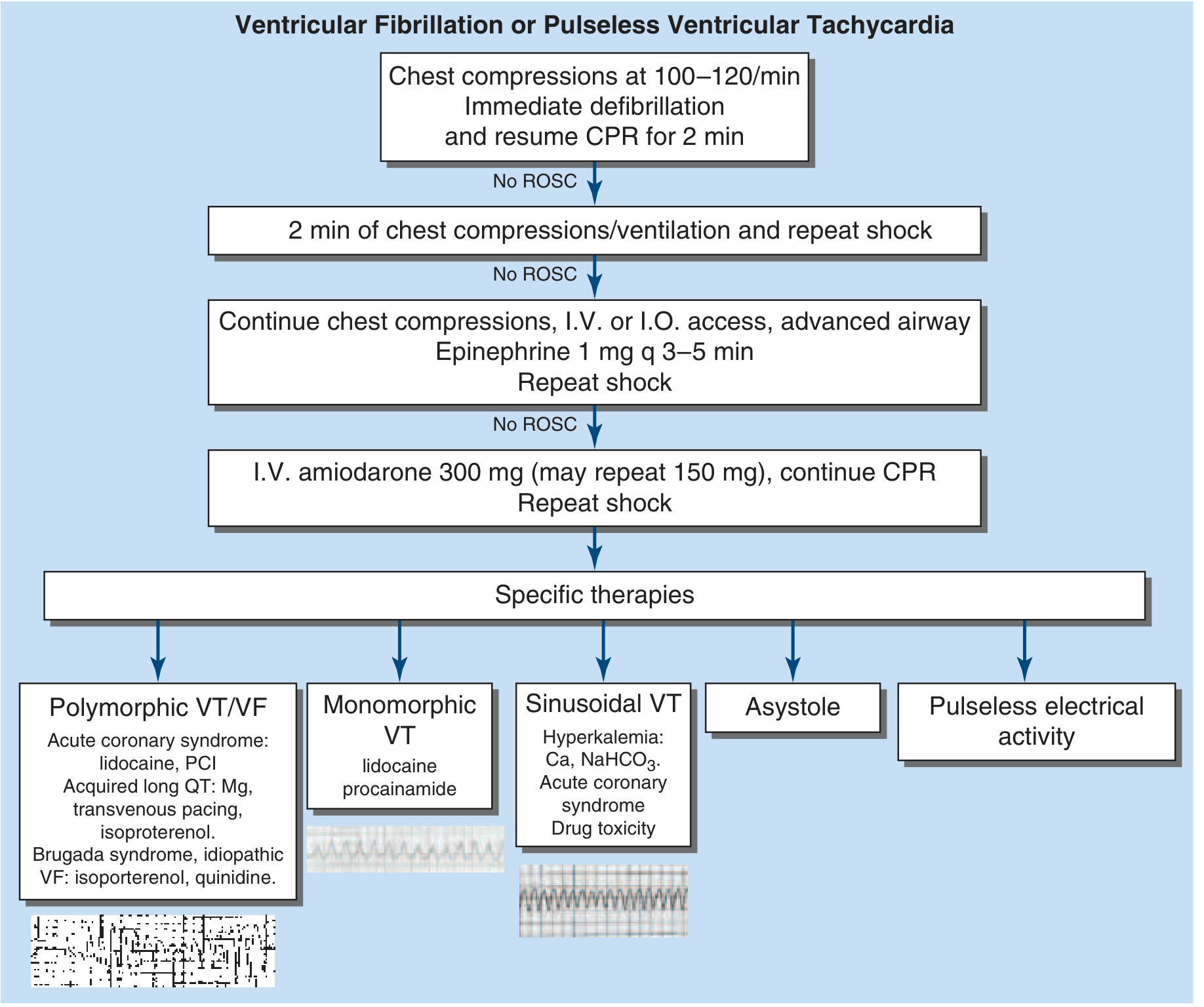
Sequence:
- Chest compressions 100–120/min + immediate defibrillation (200 J biphasic) → resume CPR 2 min
- No ROSC → 2 min CPR/ventilation + repeat shock
- No ROSC → IV/IO access + advanced airway + Epinephrine 1 mg q3–5 min + repeat shock
- No ROSC → Amiodarone 300 mg IV bolus (repeat 150 mg if recurs) + repeat shock
- If amiodarone fails → Lidocaine
- Continue guided by specific etiology (see below)
Rhythm-specific therapies:
| Rhythm Pattern | Treatment |
|---|---|
| Polymorphic VT/VF + ACS | Lidocaine, emergent PCI |
| Polymorphic VT + acquired long QT | Magnesium, transvenous pacing, isoproterenol |
| Brugada syndrome / idiopathic VF | Isoproterenol, quinidine |
| Monomorphic VT | Lidocaine, procainamide |
| Sinusoidal VT (hyperkalemia) | Calcium gluconate, NaHCO₃ |
| QT prolongation / torsades | Magnesium sulfate IV |
B. Non-Shockable Rhythms: Asystole / PEA / Bradyarrhythmia
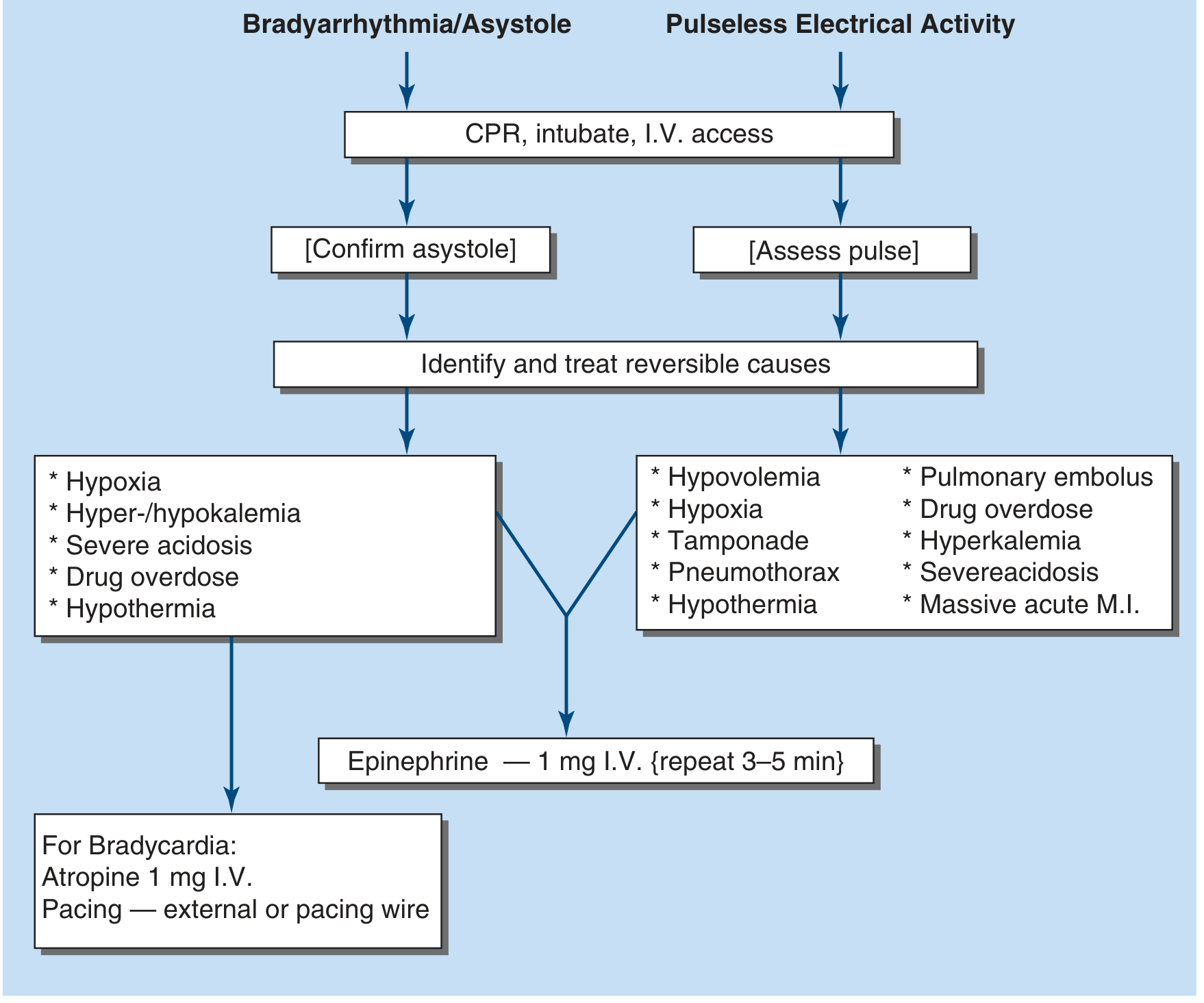
Sequence:
- CPR + intubation + IV access
- Confirm asystole (2 leads); assess pulse for PEA
- Identify and treat reversible causes (see H's & T's below)
- Epinephrine 1 mg IV q3–5 min
- For bradycardia specifically:
- Atropine 1 mg IV (note: atropine is NOT recommended for asystole/PEA per current AHA guidelines — only for bradycardic rhythms)
- External pacing or transvenous pacing wire
ACLS Algorithm Overview (AHA)
Reversible Causes — The H's & T's
These must be actively sought and corrected in all cardiac arrest situations:
| H's | T's |
|---|---|
| Hypovolemia | Tension pneumothorax |
| Hypoxia | Tamponade (cardiac) |
| Hydrogen ion excess (acidosis) | Toxins / drug overdose |
| Hypo / Hyperkalemia | Thrombosis — pulmonary (PE) |
| Hypothermia | Thrombosis — coronary (MI) |
"Naloxone should be administered if opiate overdose is suspected." — Harrison's 22E
Airway Management in ACLS
| Modality | Notes |
|---|---|
| Bag-Mask Ventilation (BMV) | Acceptable; minimizes CPR interruptions |
| Endotracheal Intubation (ETI) | Preferred for securing airway; risk of interrupting CPR |
| Supraglottic Airway (SGA) | Preferred over ETI if operator experience is limited |
| Ventilation rate with advanced airway | 1 breath every 6 compressions (10/min) |
| Target oxygen | Reverse hypoxemia; monitor arterial pO₂ — avoid hyperoxia |
ACLS Medications — Summary Table
| Drug | Dose | Indication | Notes |
|---|---|---|---|
| Epinephrine | 1 mg IV/IO q3–5 min | All cardiac arrest rhythms | PEA/asystole: use early; VF/pVT: after failed shocks. Raises diastolic BP → coronary perfusion |
| Amiodarone | 300 mg IV bolus; repeat 150 mg | Shock-refractory VF/pVT | Improves survival to hospital admission; survival to discharge benefit in witnessed arrest |
| Lidocaine | 60–100 mg IV | Amiodarone failure; acute MI-triggered arrest | Also used for monomorphic VT |
| Magnesium sulfate | IV bolus | Torsades de Pointes; resistant polymorphic VT | Even without effect on QT duration |
| Atropine | 1 mg IV | Symptomatic bradycardia only | NOT recommended for asystole or PEA |
| NaHCO₃ | 1 mEq/kg | Persistent metabolic acidosis after ROSC | Not routine |
| Calcium gluconate (10%) | IV | Acute hyperkalemia, hypocalcemia, Ca-blocker toxicity | Not routine |
| Vasopressin | — | Alternative vasoconstrictor | Not superior to epinephrine; largely fallen out of favor |
Monitoring During ACLS
| Parameter | Value / Significance |
|---|---|
| End-tidal CO₂ (EtCO₂) | Normal: 35–45 mmHg; Optimal CPR: 15–20 mmHg; ROSC: sudden rise >35 mmHg; <10 mmHg after >20 min = futility marker |
| Arterial BP | Confirms hemodynamics during CPR |
| SpO₂ / Oximetry | Guide oxygenation |
| Bedside echo | Identifies tamponade, PE, MI, wall motion |
| ABG | Assesses acidosis, hypoxia, electrolytes |
Post-Cardiac Arrest Care (After ROSC)
Per Harrison's 22E and Braunwald's:
Hemodynamic Targets
- SBP >90 mmHg / MAP >65 mmHg — use vasopressors + volume as needed
Respiratory Targets
- SpO₂: 94% (avoid hyperoxia — excessive FiO₂ worsens reperfusion injury)
- PaCO₂: 35–45 mmHg (normocapnia — avoid hypo/hypercapnia)
- ETI for impaired consciousness
Coronary Angiography
- Immediate PCI if ST-elevation on post-arrest ECG
- Also consider if: cardiogenic shock, electrical instability, ongoing ischemia
- For VT/VF without ST elevation: emergent angiography not clearly superior to delayed strategy
Targeted Temperature Management (TTM)
- Brain injury due to ischemia-reperfusion is the leading cause of death post-ROSC — accounts for >2/3 of deaths (Harrison's)
- Probability of neurologic recovery decreases rapidly: <30% at 5 min from collapse to ROSC (without CPR)
Electrolyte & Metabolic Management
- Treat hyperkalemia, severe hypokalemia, QT-prolonging drug toxicity
- Monitor and correct acidosis
Concept of Cardiocerebral Resuscitation (CCR)
A refinement of standard ACLS, also called minimally interrupted cardiac resuscitation, which:
- Emphasizes continuous chest compressions interrupted primarily for single shocks
- Defers and limits ventilatory actions
- Challenges the routine benefit of compression-ventilation cycling
- Adding "head-up/torso-up" positioning has been reported to nearly double resuscitation rates in community studies by improving cerebral perfusion (Braunwald's)
"Successful ROSC after IHCA is associated with a shorter median duration of resuscitation — 12 minutes (IQR 6–20 min) in survivors." — Braunwald's Heart Disease
BLS vs. ACLS — Key Differences
| Feature | BLS | ACLS |
|---|---|---|
| Who performs it | Laypersons, first responders, HCPs | Trained paramedics, nurses, physicians |
| Equipment needed | None / AED only | IV/IO, airway devices, drugs, monitors |
| Airway | Basic (head-tilt/chin-lift, BMV) | Advanced (ETI, SGA, capnography) |
| Pharmacology | None (naloxone in opioid OD) | Epinephrine, amiodarone, lidocaine, etc. |
| Defibrillation | AED (automated) | Manual defibrillator (synchronized/asynchronous) |
| Goal | Maintain perfusion until ACLS | Achieve ROSC + hemodynamic stabilization |
| Primary intervention | Compressions | Rhythm identification + targeted therapy |
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill) | Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine (AHA-aligned) | Fuster and Hurst's The Heart, 15th Edition
More detailed for example if give epinephrine what is the dose interval and location everything
Finding Sources
Finding Sources
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.