Peptic ulcer
Reading File
Finding Sources
Searching the Web
peptic ulcer disease pathophysiology diagnosis treatment 2024
Searching PubMed
"peptic ulcer"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
I now have very comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Peptic Ulcer Disease (PUD)
Definition
A peptic ulcer is an excoriated mucosal defect extending through the muscularis mucosae in any portion of the GI tract exposed to gastric acid and pepsin. Although the name implies pepsin, acid is the indispensable factor - peptic ulcers do not occur in its absence, and nearly all heal with proton pump inhibitors (PPIs). - Guyton & Hall Textbook of Medical Physiology; Bailey & Love's Short Practice of Surgery, 28e
Common Sites
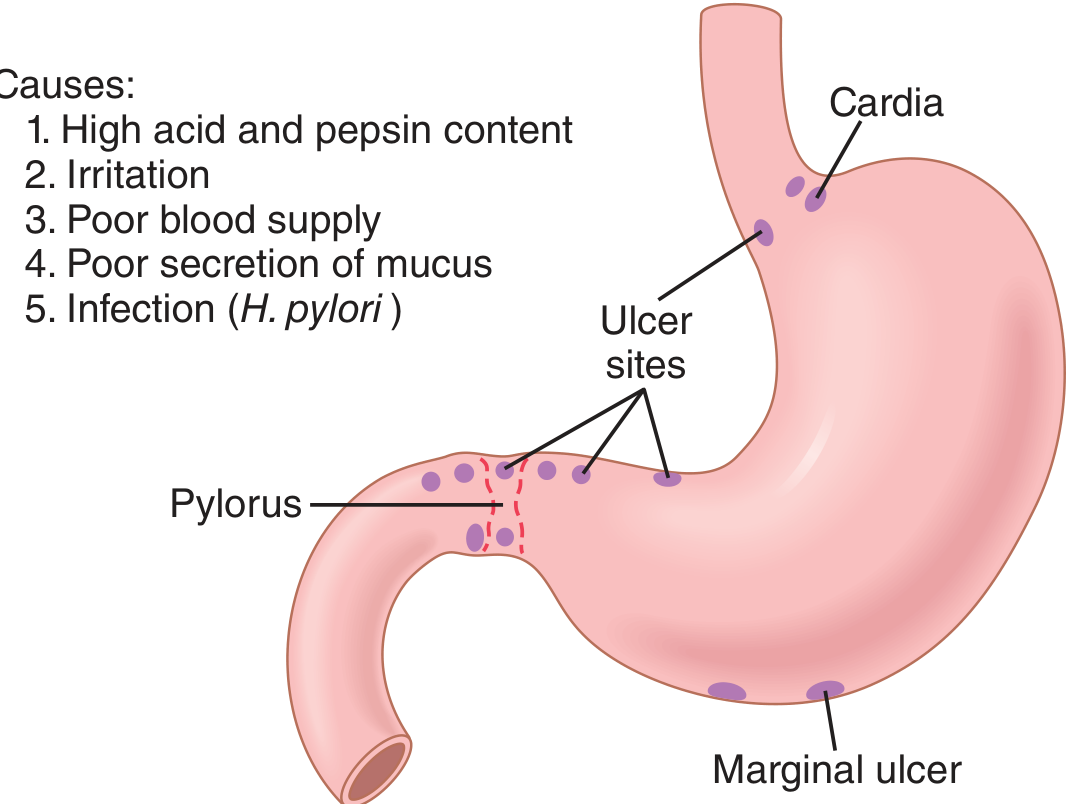
Figure: Causes and common sites of peptic ulcer (Guyton & Hall)
| Site | Notes |
|---|---|
| First part of duodenum | Most common overall |
| Gastric antrum / lesser curve (incisura angularis) | Classic gastric ulcer location |
| Prepyloric / pyloric channel | Behaves like duodenal ulcer; must biopsy |
| Oesophagus (lower) | Due to acid reflux |
| Meckel's diverticulum | Contains ectopic gastric mucosa |
| Stomal (marginal) ulcer | After gastroenterostomy or Billroth II |
- Bailey & Love's Short Practice of Surgery, 28e; Guyton & Hall
Epidemiology
-
Over 4 million individuals in the US are treated each year
-
Lifetime risk: ~10% in males, ~4% in females
-
Duodenal ulcers are ~4x more common than gastric ulcers
-
Incidence is declining in resource-rich countries (due to H. pylori eradication) but rising in resource-poor nations
-
Peak incidence has shifted to older age groups; gender gap is narrowing
-
Robbins & Kumar Basic Pathology; Bailey & Love, 28e
Pathophysiology - The Balance Concept
PUD results from an imbalance between damaging and protective forces:
Protective factors:
- Mucus gel layer (secreted by mucous neck glands)
- HCO₃⁻ secretion trapped within mucus (neutralizes any H⁺ that penetrates)
- Prostaglandin E₂ (stimulates HCO₃⁻ secretion, maintains mucosal blood flow)
- Mucosal blood flow and growth factors
- Pancreatic bicarbonate (neutralizes acid in duodenum)
- Brunner glands (alkaline mucus in proximal duodenum)
Damaging factors:
-
H⁺ and pepsin (always required)
-
Helicobacter pylori infection
-
NSAIDs (suppress prostaglandin synthesis, impair barrier)
-
Smoking (reduces mucosal blood flow, delays healing)
-
Alcohol, stress, corticosteroids
-
Costanzo Physiology, 7e; Robbins & Kumar Basic Pathology
Aetiology
1. Helicobacter pylori
-
Responsible for >70% of PUD cases overall; >90% of duodenal ulcers
-
Gram-negative bacterium that colonises gastric mucus (especially the antrum)
-
Survives in the acid environment via urease - converts urea to NH₃, alkalinising its local environment
-
Releases cytotoxins (e.g., CagA toxin) that disrupt the mucous barrier and damage epithelial cells
-
NH₄⁺ (in equilibrium with NH₃) is directly cytotoxic
-
Diagnostic basis of the ¹³C-urea breath test: patient drinks ¹³C-urea → converted to ¹³CO₂ by urease → detected in exhaled breath
-
Only 5-10% of infected individuals develop ulcers, so host factors and strain variation (CagA-positive strains are more virulent) also matter
-
Costanzo Physiology, 7e; Robbins & Kumar Basic Pathology
2. NSAIDs
- Inhibit COX enzymes → suppress prostaglandin synthesis → loss of mucosal protection and HCO₃⁻ secretion
- Now the most common cause of gastric ulcers in Western countries as H. pylori rates fall, while low-dose aspirin use in older adults increases
- Robbins & Kumar Basic Pathology
3. Zollinger-Ellison Syndrome
- Gastrin-secreting tumour (gastrinoma) → massive acid hypersecretion
- Causes multiple ulcers in stomach, duodenum, and even jejunum
- In this syndrome, acid is essentially the sole aetiological factor
- Robbins & Kumar Basic Pathology; Bailey & Love, 28e
4. Other Risk Factors
- Cigarette smoking (increased relapse rate)
- Alcohol-related cirrhosis, COPD, chronic renal failure, hyperparathyroidism
- Hypercalcaemia (stimulates gastrin → increases acid secretion)
- High-dose corticosteroids
Morphology (Pathology)
-
Chronic ulcers penetrate the mucosa into the muscularis propria, leading to fibrosis
-
Gastric ulcers tend to be larger than duodenal ulcers
-
Gastric ulcers: most common on lesser curve at the incisura angularis (boundary between acid-secreting and non-acid-secreting epithelia)
-
Duodenal: most common in the first part; "kissing ulcers" = simultaneous anterior and posterior ulcers (anterior tend to perforate, posterior tend to bleed from the gastroduodenal artery)
-
Fibrosis from chronic ulcers can cause pyloric stenosis or "hourglass" deformity of the stomach
-
Chronic gastric ulcers may erode posteriorly into the pancreas or splenic artery
-
Bailey & Love, 28e
Clinical Features
Gastric and duodenal ulcers are clinically indistinguishable by symptoms alone.
-
Epigastric pain: gnawing or burning in character, sometimes radiating to the back
-
Pain may be relieved by eating (especially duodenal) or worsened by food (gastric)
-
Intermittent course with periods of remission - this periodicity reflects spontaneous healing cycles
-
Vomiting: not prominent unless gastric outlet obstruction occurs
-
Weight loss (gastric ulcers often present with weight loss)
-
Bleeding: chronic blood loss → microcytic anaemia; acute = haematemesis ± melaena
-
Examination: epigastric tenderness; succussion splash if gastric outlet obstruction
-
Bailey & Love, 28e
Investigations
Endoscopy (Gastroduodenoscopy) - Gold Standard
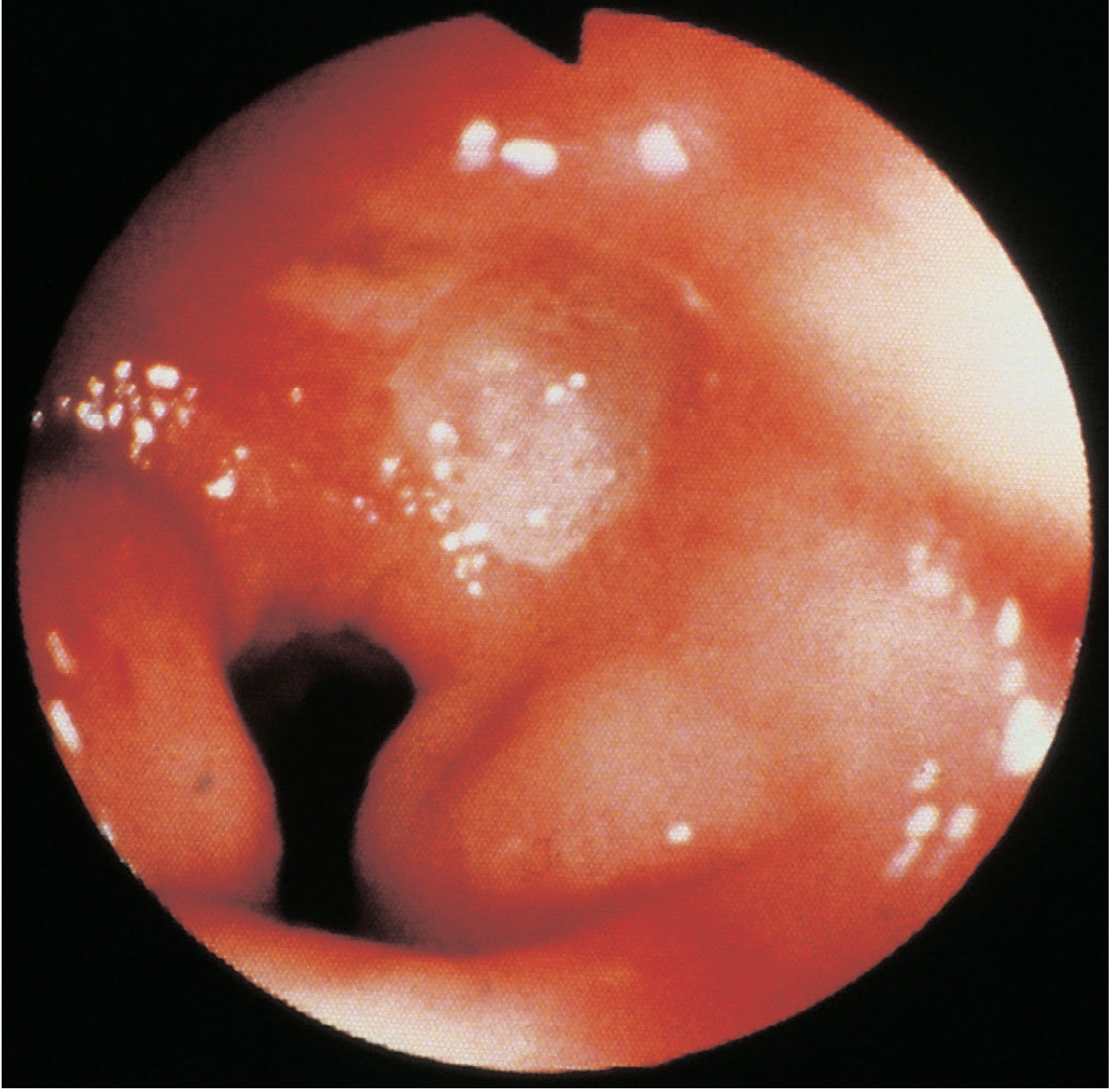
Figure: Duodenal ulcer at gastroduodenoscopy (Bailey & Love, 28e)
- Allows direct visualisation, biopsy, and therapeutic intervention
- All gastric ulcers must be biopsied (multiple biopsies) to exclude malignancy, regardless of appearance
- Antral biopsies + CLO (Campylobacter-like organism) test for H. pylori
- Duodenal ulcers: biopsy not mandatory for malignancy (duodenal ulcer = almost never malignant), but H. pylori testing should be done
H. pylori Testing
| Test | Type | Notes |
|---|---|---|
| ¹³C-urea breath test | Non-invasive | High sensitivity/specificity; used for diagnosis + post-treatment |
| Stool antigen test | Non-invasive | Equally accurate |
| CLO (urease) test | Endoscopic | Rapid, done at endoscopy |
| Serology | Blood | Cannot confirm active infection or eradication |
| Histology | Endoscopic | Gold standard for tissue diagnosis |
Barium Meal
- Now largely replaced by endoscopy
- Duodenal ulcer: "niche" sign; gastric ulcer: seen on lesser curve with radiating folds
- Useful where endoscopy not available
Other Tests
- FBC (anaemia), urea and electrolytes
- Fasting gastrin level if Zollinger-Ellison suspected
Treatment
1. Acid Suppression
- Proton pump inhibitors (PPIs): first-line for all peptic ulcers; render patients virtually achlorhydric; standard dose for 4-8 weeks
- H₂ receptor antagonists: less potent than PPIs; used as adjuncts or alternatives
- Antacids: symptom relief only
2. H. pylori Eradication
The cornerstone of treatment for H. pylori-positive ulcers. Standard regimens:
- Triple therapy: PPI + clarithromycin + amoxicillin (or metronidazole) for 7-14 days
- Quadruple therapy (bismuth-based): PPI + bismuth + tetracycline + metronidazole - used where clarithromycin resistance is high or after first-line failure
- Rising antibiotic resistance (especially to clarithromycin and levofloxacin) has complicated eradication, per 2024 ACG guidelines
Recent evidence: A 2024 systematic review with meta-analysis (PMID 39294424) found that vonoprazan (a potassium-competitive acid blocker) is superior to PPIs for both treatment and prevention of gastric/duodenal ulcers, representing an emerging alternative to standard PPI-based regimens.
A 2025 Cochrane review (PMID 40337979) confirmed that PPIs effectively prevent NSAID-induced ulcers and dyspepsia.
3. NSAID-Induced Ulcers
- Stop the NSAID if possible
- PPI co-prescription if NSAID cannot be stopped
- Switch to selective COX-2 inhibitor (lower ulcer risk, though not zero)
4. Lifestyle Measures
- Stop smoking (reduces relapse rate)
- Avoid alcohol excess
- Avoid NSAIDs and aspirin where possible
5. Surgery
Surgery is now very rarely required for uncomplicated PUD. Indications:
- Failure of medical therapy
- Complications (perforation, uncontrolled bleeding, obstruction)
- Suspected malignancy
Complications
| Complication | Key Points |
|---|---|
| Bleeding | Most common complication; posterior duodenal ulcers erode the gastroduodenal artery; assessed by Rockall score; endoscopic therapy first-line |
| Perforation | Anterior duodenal ulcers most often perforate; presents with sudden-onset peritonitis; primarily surgical (laparoscopic Graham patch repair) |
| Gastric outlet obstruction | Fibrosis → pyloric stenosis; presents with vomiting, succussion splash; balloon dilation or surgery |
| Malignant transformation | Rare in gastric ulcers; virtually never in duodenal ulcers; always biopsy gastric ulcers |
| Penetration | Erosion into adjacent organs (pancreas, splenic artery, colon) |
Gastric vs. Duodenal Ulcer - Comparison
| Feature | Gastric Ulcer | Duodenal Ulcer |
|---|---|---|
| Relative frequency | Less common | More common (~4x) |
| Acid secretion | Normal or low | Often elevated |
| Pain and food | Pain may worsen with food | Food often relieves pain |
| Malignancy risk | Present - always biopsy | Virtually nil |
| H. pylori association | Common | Very common (>90%) |
| Typical site | Lesser curve, incisura angularis | First part of duodenum |
| Posterior erosion risk | Splenic artery, pancreas | Gastroduodenal artery (bleeding) |
| Anterior perforation | Less common | Common ("anterior perforate, posterior bleed") |
Sources:
- Robbins & Kumar Basic Pathology, p. 3901-3909
- Guyton & Hall Textbook of Medical Physiology, p. 825
- Bailey & Love's Short Practice of Surgery, 28e, p. 1178-1180
- Costanzo Physiology, 7e, p. 370
- Sleisenger & Fordtran's Gastrointestinal and Liver Disease
- PMID 39294424 - Vonoprazan vs PPIs meta-analysis (2024)
- PMID 40337979 - Cochrane review: PPIs for NSAID-induced ulcers (2025)
This is a shared conversation. Sign in to Orris to start your own chat.