Respiration mechanism physiology detail with flowcharts and simple explanation
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Searching the Web
mechanism of respiration physiology inspiration expiration flowchart simple
I now have all the information needed to compile a comprehensive, well-structured answer with flowcharts. Let me write it up:
Respiration: Mechanism & Physiology
What is Respiration?
Respiration is the process by which the body takes in oxygen (O₂) from the atmosphere, delivers it to cells, and removes carbon dioxide (CO₂) produced by cellular metabolism. It has two major components:
- External respiration - gas exchange between air and blood (lungs)
- Internal respiration - gas exchange between blood and tissue cells
Overview Flowchart
ATMOSPHERE (O₂ rich air)
↓
Nose/Mouth → Trachea → Bronchi → Bronchioles → Alveoli
↓
GAS EXCHANGE in Alveoli (O₂ in, CO₂ out)
↓
Pulmonary Capillaries → Blood (O₂ bound to Hemoglobin)
↓
Heart (Left side) → Systemic Circulation
↓
Tissue Capillaries → Cells receive O₂, release CO₂
↓
CO₂-rich blood → Heart (Right side) → Lungs
↓
CO₂ diffuses into alveoli → exhaled out
Phase 1: Ventilation (Breathing Mechanics)
Ventilation is the physical movement of air in and out of the lungs. It works on a simple principle: air always flows from high pressure to low pressure.
A. INSPIRATION (Breathing IN) - Active Process
BRAIN (Medulla/Pons) sends nerve signals
↓
Phrenic nerve (C3,4,5) → Diaphragm contracts & flattens
Intercostal nerves → External intercostal muscles contract
↓
Thoracic cavity EXPANDS (volume ↑)
↓
Intrapleural pressure FALLS (becomes more negative)
↓
Lung volume INCREASES (lungs stretch passively via pleura)
↓
Intrapulmonary (alveolar) pressure DROPS below atmospheric
↓
Air flows IN from atmosphere → down pressure gradient
↓
Alveoli fill with fresh air
Key muscles: The diaphragm is the most important muscle of inspiration - it accounts for ~75% of inspiratory effort. When it contracts, the abdominal contents are pushed downward and the ribs lift upward and outward. - Costanzo Physiology 7th Edition
During exercise, the external intercostal muscles and accessory muscles (sternocleidomastoid, scalenes) assist.
B. EXPIRATION (Breathing OUT) - Passive at Rest
Diaphragm & intercostals RELAX
↓
Thoracic cavity RECOILS inward (volume ↓)
↓
Elastic recoil of lung tissue pushes air out
↓
Intrapulmonary pressure RISES above atmospheric
↓
Air flows OUT down pressure gradient
↓
Exhalation complete
During exercise or in obstructive disease (e.g., asthma): expiration becomes active, using the abdominal muscles and internal intercostal muscles to forcibly push air out. - Costanzo Physiology 7th Edition
Phase 2: Gas Exchange (Diffusion)
At the Alveoli (External Respiration)
Gas exchange across the alveolar-capillary membrane occurs purely by passive diffusion down partial pressure gradients. The wall is only ~1.5 µm thick - extremely thin for rapid exchange.
ALVEOLUS | BLOOD (Pulmonary capillary)
|
PO₂ = 100 mmHg | PO₂ = 40 mmHg (deoxygenated blood)
| → O₂ diffuses from alveolus INTO blood ✓
|
PCO₂ = 40 mmHg | PCO₂ = 45 mmHg (CO₂ from tissues)
| → CO₂ diffuses from blood INTO alveolus ✓
|
Result: blood becomes OXYGENATED & CO₂ is exhaled
At the Tissues (Internal Respiration)
BLOOD (Systemic capillary) | TISSUE CELL
|
PO₂ = 100 mmHg | PO₂ = 40 mmHg (cell uses O₂)
| → O₂ diffuses INTO cells ✓
|
PCO₂ = 40 mmHg | PCO₂ = 45 mmHg (CO₂ produced)
| → CO₂ diffuses INTO blood ✓
|
Result: cells get O₂, CO₂ removed to blood
During inhalation, the bronchi, bronchioles, and alveolar ducts all increase in diameter and length. Alveoli enlarge slightly and elastic fibers stretch. During exhalation, the elastic fibers recoil passively, driving air back out. - Junqueira's Basic Histology, 17e
Phase 3: Oxygen Transport in Blood
Once O₂ enters the blood, it is carried in two ways:
| Form | Amount | Mechanism |
|---|---|---|
| Bound to hemoglobin (HbO₂) | ~98.5% | Each Hb carries 4 O₂ molecules |
| Dissolved in plasma | ~1.5% | Very small contribution |
The Bohr Effect (O₂ Release at Tissues)
When blood reaches metabolically active tissues:
CO₂ enters blood from tissues
↓
CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻
↓
pH falls (blood becomes more acidic)
↓
O₂-Hemoglobin dissociation curve shifts RIGHT
↓
Hemoglobin releases MORE O₂ to tissues ✓
In the lungs, the reverse happens: CO₂ leaves blood → pH rises → curve shifts LEFT → Hb picks up MORE O₂. - Guyton & Hall Textbook of Medical Physiology
Factors that shift the O₂-Hb curve to the RIGHT (more O₂ released to tissues):
- ↑ CO₂
- ↑ H⁺ (lower pH)
- ↑ Temperature
- ↑ 2,3-BPG (important in chronic hypoxia)
Phase 4: CO₂ Transport in Blood
CO₂ is carried from tissues back to the lungs in three forms:
| Form | % Carried | Notes |
|---|---|---|
| As bicarbonate (HCO₃⁻) | ~70% | Main form; formed inside RBCs |
| Bound to hemoglobin (carbaminohemoglobin) | ~23% | CO₂ binds to protein part of Hb |
| Dissolved in plasma | ~7% | Small but contributes to PCO₂ |
Phase 5: Control of Breathing
Breathing is automatically controlled by the brainstem. You don't have to think about it!
PERIPHERAL CHEMORECEPTORS CENTRAL CHEMORECEPTORS
(Carotid & aortic bodies) (Medulla - brain surface)
↓ Detect low PO₂ / high PCO₂ ↓ Detect CO₂/H⁺ in CSF
↓ ↓
↓←←←← SIGNALS ←←←←←←←←←←←←←←↓
↓
RESPIRATORY CENTER (Medulla & Pons)
↓
┌────────┴────────┐
Pre-Bötzinger complex Pontine Respiratory Group
(rhythmic inspiration) (modulates rhythm/pattern)
↓
Phrenic nerve + Intercostal nerves
↓
Muscles contract → BREATH
Key triggers for increased breathing:
- ↑ CO₂ in blood (most powerful stimulus)
- ↓ O₂ in blood (severe hypoxia)
- ↓ pH (acidosis)
- Exercise (anticipatory + feedback signals)
Lung Compliance and Surfactant
Compliance = how easily the lung stretches for a given pressure change.
- High compliance (e.g., emphysema) = lungs too "floppy" → hyperinflation
- Low compliance (e.g., fibrosis) = lungs too stiff → restricted breathing
Surfactant (produced by Type II pneumocytes) lines alveoli and reduces surface tension, preventing alveolar collapse (atelectasis). Without surfactant (e.g., in premature infants - Respiratory Distress Syndrome), alveoli collapse with each breath.
FEV₁/FVC - Clinical Lung Function Test
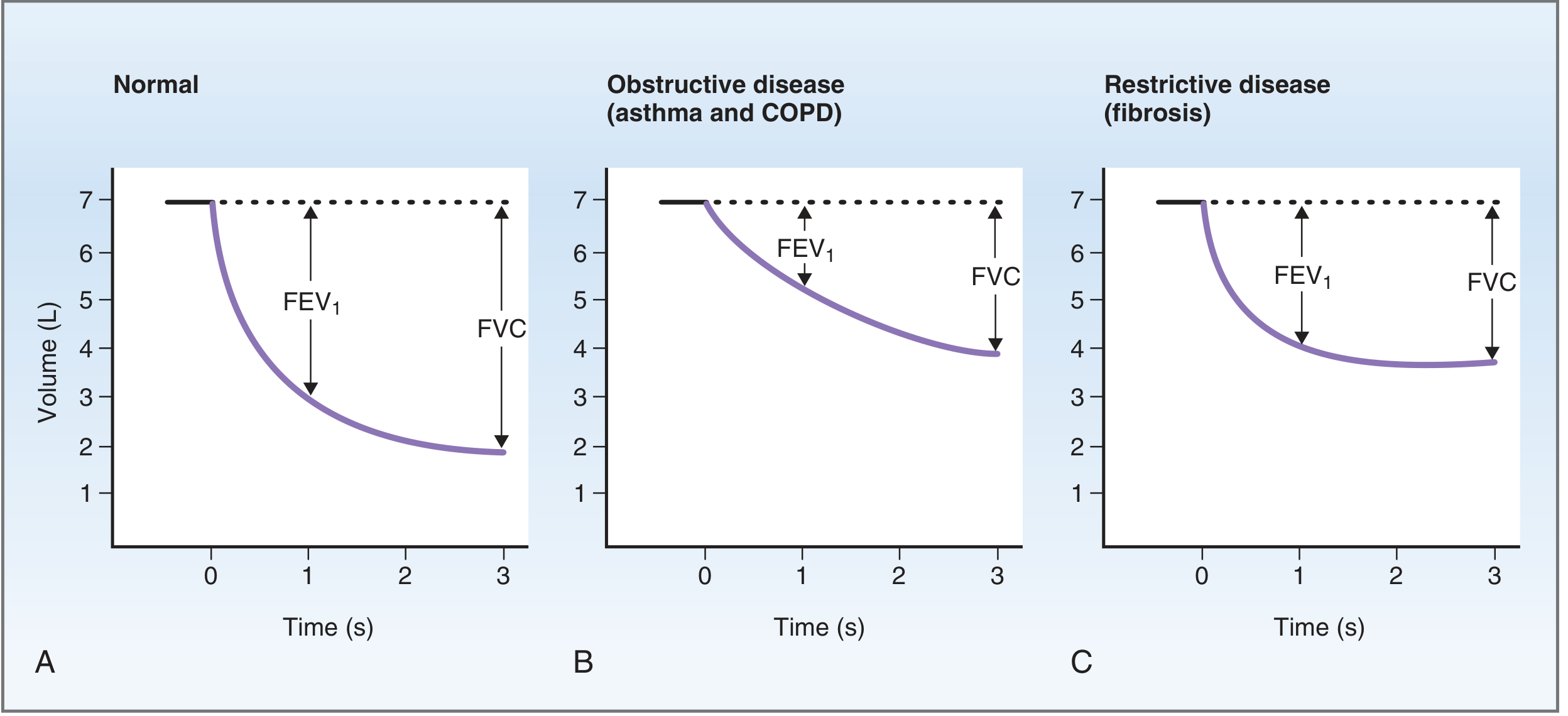
Normal FEV₁/FVC ≈ 0.8 (80% of vital capacity expired in 1 second)
| Disease | FVC | FEV₁ | FEV₁/FVC | Example |
|---|---|---|---|---|
| Normal | Normal | Normal | ~0.80 | - |
| Obstructive | ↓ | ↓↓ | ↓ (<0.70) | Asthma, COPD |
| Restrictive | ↓ | ↓ | ↑ or normal | Fibrosis |
- Costanzo Physiology 7th Edition, pp. 204-205
Summary: The Complete Cycle (Simple Version)
┌─────────────────────────────────────────────────────┐
│ 1. BRAIN signals diaphragm to contract │
│ 2. Chest expands → pressure drops → AIR INHALED │
│ 3. O₂ diffuses from alveoli into blood │
│ 4. O₂ binds hemoglobin → carried to body cells │
│ 5. Cells use O₂ → make CO₂ │
│ 6. CO₂ diffuses into blood → back to lungs │
│ 7. Diaphragm relaxes → chest recoils → AIR EXHALED │
│ 8. CO₂ released into alveoli → breathed out │
│ 9. CO₂ levels sensed → brain triggers next breath │
│ 10. Cycle repeats ~12-20 times per minute at rest │
└─────────────────────────────────────────────────────┘
Sources:
- Costanzo Physiology 7th Edition - Mechanics of Breathing, pp. 204-215
- Junqueira's Basic Histology, 17e - Respiratory Movements, p. 893
- Guyton & Hall Textbook of Medical Physiology - Oxygen transport, Bohr Effect, p. 526
- TeachMePhysiology - Mechanics of Breathing
This is a shared conversation. Sign in to Orris to start your own chat.