Acupuncture therapy, scalp needling
Reading File
Finding Sources
Finding Sources
Searching Images
scalp acupuncture needling zones therapy
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Searching Images
scalp acupuncture zones map motor sensory areas
Loading Image
Reading File
Here is a comprehensive overview of scalp acupuncture (SA) therapy:
Scalp Acupuncture — Overview
What Is It?
Scalp acupuncture is a specialized form of acupuncture in which fine needles are inserted subcutaneously into specific zones of the scalp, targeting regions that correspond somatotopically to underlying cortical areas (motor strip, sensory strip, visual cortex, etc.). It is distinct from traditional body acupuncture in that needle placement is guided by neuroanatomical mapping rather than classical meridian theory alone.
Anatomical Basis of Needle Insertion
The needle penetrates through the scalp and subcutaneous tissue to rest in the subgalea layer — the loose connective tissue beneath the galea aponeurotica — parallel to the skull surface.
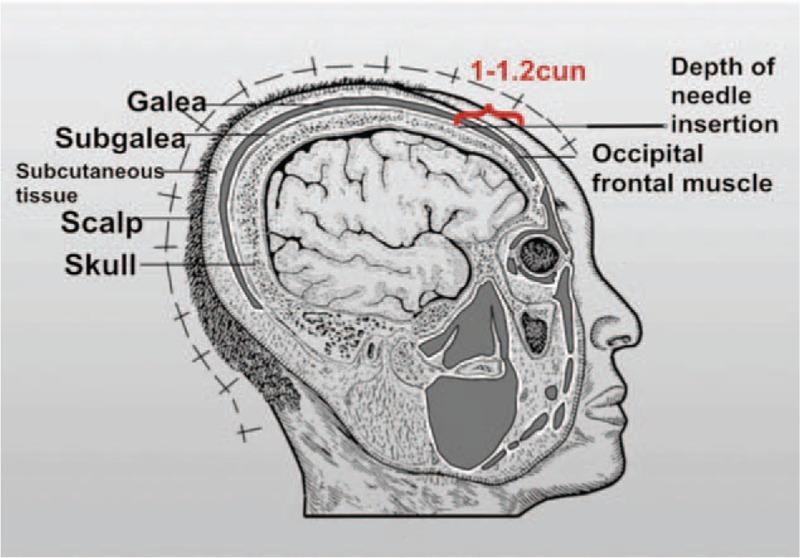
Insertion depth: 1–1.2 cun (approximately 2.5–3 cm), traversing:
- Scalp (skin)
- Subcutaneous tissue
- Galea aponeurotica
- Subgalea (target layer)
The needle lies parallel to the skull, not perpendicular. This is critical to avoid periosteum stimulation or vessel injury.
Procedure — Clinical Steps
Based on standard acupuncture procedure protocols:
- Patient positioning: Supine or prone depending on the target zone; standing/sitting is avoided, especially on the first visit.
- Point palpation: Acupoints are located on the scalp according to zone maps (e.g., motor zone, sensory zone, equilibrium zone).
- Needle insertion: 0.5–3 inch, 30–34 gauge solid stainless steel needles are inserted with a slight twirling motion at a shallow angle (nearly parallel to the skin). The classic de qi sensation (dull ache, heaviness, distension) indicates sufficient depth.
- Stimulation: After insertion, needles may be:
- Manually stimulated — rapid twirling (200 rotations/min) for 1–3 minutes
- Electroacupuncture (EA) — alligator clips attached to needle shafts connected to a battery-operated stimulator (similar to a TENS unit); current gradually increased to patient's maximal tolerance
- Retention time: 15–30 minutes per session; a timer is set and a practitioner remains accessible.
- Removal: Needles disposed of in a sharps container after single use.

Treatment Course
- Most conditions amenable to acupuncture respond within 4–10 treatments
- Follow-up intervals: up to 2 weeks apart
- As improvement occurs, intervals are spaced farther apart
- Some patients require periodic "tune-up" sessions for sustained benefit
Proposed Mechanisms
- Stimulates sensory afferent fibers → influences the CNS
- Facilitates neurotrophin release → promotes neural plasticity and repair (especially relevant in deafferentation states)
- May modulate the central auditory pathway at the olivocochlear nucleus
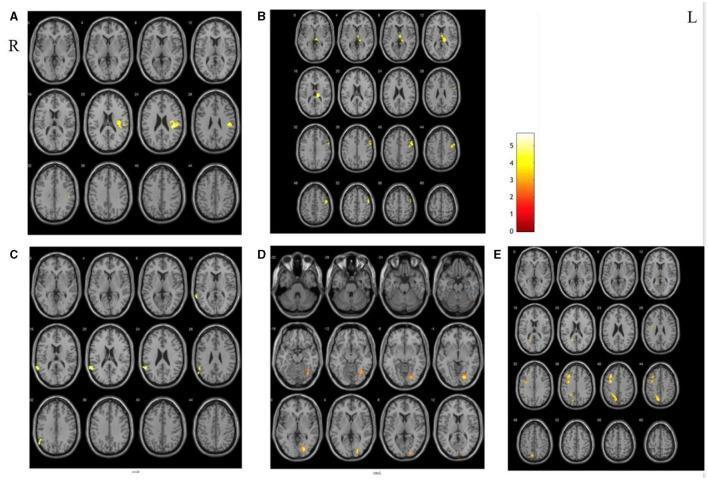
- fMRI evidence suggests acupuncture modulates limbic and subcortical structures involved in learned discomfort responses
- In post-stroke patients, SA alters resting-state functional connectivity (RSFC) — increased connectivity in putamen, postcentral gyrus, insula, and thalamus; decreased in globus pallidus and superior temporal gyrus
Clinical Applications
| Condition | Evidence Level |
|---|---|
| Stroke rehabilitation (motor/sensory deficits) | Moderate — neuroplasticity basis |
| Somatic tinnitus | Positive — responsive to scalp & auricular stimulation |
| Chronic pain | Moderate RCT evidence |
| Neurological dysfunction (intractable hiccups, insomnia) | Case-series level |
| Bilateral subjective tinnitus | No consistent benefit in blinded RCTs |
| Facial paralysis | Used in acute stage with shallow needling (0.1–0.2 cm depth, oblique angle) |
Contraindications
- Electroacupuncture must never be applied across the brain or heart
- Over the infant's fontanelle
- Over major vessels or nerves
- Active scalp infection, open wounds, or compromised skin
- Pregnancy — certain points (not necessarily scalp) may stimulate labor
- Relative: sitting or standing position for treatment (syncope risk); first treatment especially
Evidence Summary for Tinnitus (a well-studied indication)
From Cummings Otolaryngology:
"One systematic review of nine RCTs found an overall poor methodological quality, of which five RCTs showed no difference between acupuncture or electroacupuncture and a sham procedure. Of the four remaining RCTs, two showed a benefit with scalp acupuncture compared with needle insertion at nonacupoints… Current guidelines make no recommendation for or against acupuncture in the routine treatment of tinnitus."
The subset with somatosensory/somatic tinnitus (tinnitus modulated by head/neck maneuvers) appears to be the group most likely to benefit.
Sources: Pfenninger and Fowler's Procedures for Primary Care, 3rd ed.; Cummings Otolaryngology: Head and Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.