What is fundus autofluroscence . Take refernce from rynes , kanski , khurana & zia
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Searching Images
fundus autofluorescence normal and abnormal retinal imaging
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have sufficient content from the textbooks to compose a comprehensive answer. Note: Khurana's Ophthalmology and Zia's textbook are not in the library, but I have Kanski's (10th ed), Wills Eye Manual, and Bradley & Daroff's Neurology, with strong coverage. I'll compile the answer now, clearly citing sources.
Fundus Autofluorescence (FAF)
Note: Khurana's Comprehensive Ophthalmology and Zia's textbook are not in the available library. The information below is drawn from Kanski's Clinical Ophthalmology (10th ed), the Wills Eye Manual, and Bradley & Daroff's Neurology in Clinical Practice, supplemented with standard ophthalmic knowledge.
Definition
Fundus autofluorescence (FAF) is a non-invasive, dye-free imaging modality that captures the naturally occurring fluorescence of endogenous fluorophores within the fundus — most importantly lipofuscin — to map the metabolic status of the retinal pigment epithelium (RPE) and its interface with the photoreceptors.
"Imaging of fundus autofluorescence (FAF) using an enhanced fundus camera or scanning laser ophthalmoscopy permits visualization of accumulated lipofuscin in the retinal pigment epithelium." — Kanski's Clinical Ophthalmology, 10th ed.
Principle / Mechanism
- The primary fluorophore is lipofuscin, a by-product of incomplete lysosomal digestion of shed photoreceptor outer segments, accumulating within RPE cell cytoplasm.
- When excited by blue (488 nm) or green wavelength light, these fluorophores emit light at a longer wavelength (~500–700 nm), which is captured to form the FAF image.
- Images can be acquired using:
- A modified fundus camera (with excitation and barrier filters)
- Scanning Laser Ophthalmoscope (SLO) — provides superior signal-to-noise ratio
- SLO-OCT combination machines
- Wide-field SLO systems
"Autofluorescence imaging records the light emitted by native fluorophores in the retina after excitation by light of a blue or green wavelength. The principal naturally occurring fluorophore is lipofuscin, contained within cytoplasmic granules of retinal pigment epithelial cells." — Bradley & Daroff's Neurology in Clinical Practice
Normal FAF Appearance
Normal FAF image (Wills Eye Manual):
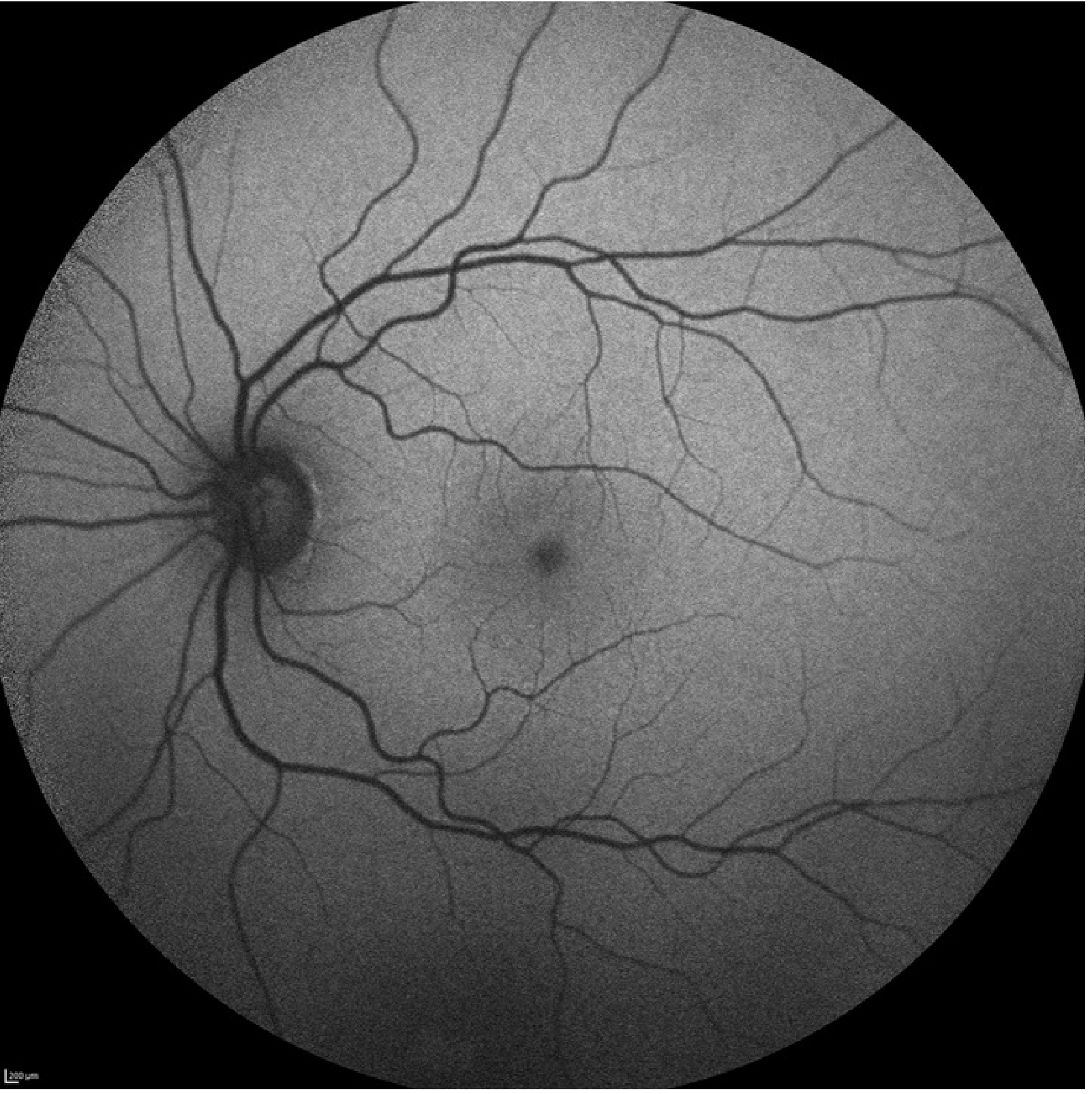
Features of a normal FAF:
| Structure | Appearance | Reason |
|---|---|---|
| Background retina | Low-level, uniform grey fluorescence | Baseline lipofuscin in RPE |
| Fovea | Hypo-autofluorescent (dark) | Macular luteal pigment absorbs blue excitation light |
| Optic disc | Very dark (absent signal) | No RPE, no fluorophores |
| Retinal blood vessels | Dark linear structures | Haemoglobin masks underlying fluorescence |
"A normal FAF image shows a low-intensity background autofluorescence with reduced intensity in the foveal region related to the absorption of blue light by macular luteal pigment. The optic nerves and blood vessels, which contain no fluorophores, appear very dark." — Bradley & Daroff's Neurology in Clinical Practice
Abnormal FAF Patterns
1. Hyperautofluorescence (Increased signal — bright areas)
- Indicates increased lipofuscin accumulation due to RPE dysfunction or metabolic stress
- Seen in:
- Inherited retinal degenerations (e.g. Retinitis Pigmentosa — perimacular ring of hyper-AF, diffuse patchy hypo-AF in mid-periphery)
- Geographic atrophy (AMD) — hyperautofluorescent rim at the leading edge of atrophy, preceding further retinal demise
- MEWDS (Multiple Evanescent White Dot Syndrome)
- Serpiginous choroidopathy
- AZOOR (Acute Zonal Occult Outer Retinopathy)
- Optic disc drusen (hyperautofluorescent)
2. Hypoautofluorescence (Decreased signal — dark areas)
- Indicates loss of RPE cells, decreased lipofuscin, or blockage of fluorescence
- Seen in:
- RPE atrophy (e.g. central area in geographic atrophy)
- Fibrosis / subretinal fibrosis
- Pigment clumping / haemorrhage (masking effect)
- RPE rips, laser scars
"Hyperautofluorescence — Many retinal diseases result in RPE dysfunction and an accumulation of RPE lipofuscin, which causes abnormal patterns of hyperautofluorescence on FAF imaging." — Kanski's Clinical Ophthalmology, 10th ed.
"Hypoautofluorescence indicates areas of decreased lipofuscin, decreased RPE density or blockage of fluorescence (e.g. RPE atrophy, fibrosis)." — Kanski's Clinical Ophthalmology, 10th ed.
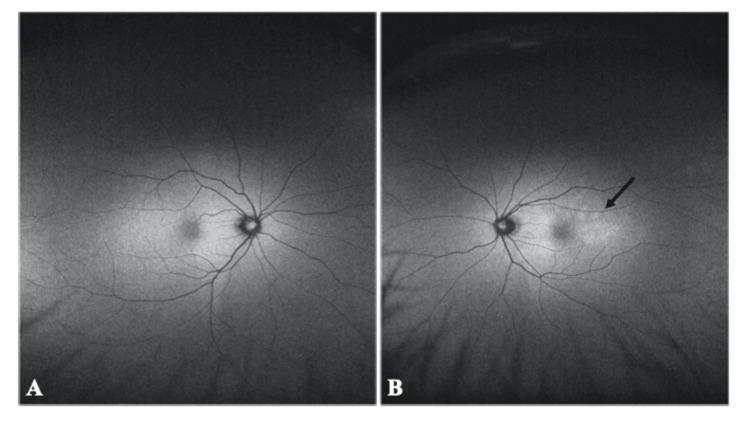
Normal (A) vs. Abnormal (B) FAF — hyperautofluorescence from choroidal lesions:
Clinical Applications
| Condition | FAF Finding |
|---|---|
| Age-related macular degeneration (AMD) — geographic atrophy | Dark (hypo-AF) central area + hyper-AF ring at active border |
| Retinitis pigmentosa & inherited retinal dystrophies | Perimacular ring of hyper-AF; patchy hypo-AF peripherally; key diagnostic & monitoring tool |
| Stargardt disease | Hypo-AF (atrophic areas) surrounded by pisciform flecks |
| Best disease (vitelliform dystrophy) | Stage-dependent AF changes |
| MEWDS / AZOOR / serpiginous choroidopathy | Pronounced hyperautofluorescence in active lesions |
| Optic disc drusen | Bright hyperautofluorescence (useful to differentiate buried drusen from papilloedema) |
| Choroidal melanoma / nevi | Lipofuscin-mediated AF patterns assist in monitoring |
| Drug toxicity (hydroxychloroquine) | FAF used alongside OCT and mfERG for toxicity monitoring |
"FAF is a non-invasive technique that detects lipofuscin and melanin in retinal pigment epithelium (RPE) cells. This provides information on RPE function and the integrity of the chorioretinal interface and is extremely helpful when assessing inflammatory conditions of the choriocapillaris." — Kanski's Clinical Ophthalmology, 10th ed.
"FAF provides sensitive information regarding the health of the RPE and allows early detection and monitoring of a variety of conditions such as age-related macular degeneration, macular dystrophies, and medication toxicity. Additionally, FAF is useful in the evaluation of certain ocular tumors, specifically choroidal nevi and melanomas." — Wills Eye Manual
Advantages
- Non-invasive — no dye injection required
- Rapid and repeatable — suitable for monitoring disease progression
- Detects subclinical RPE dysfunction before clinical or angiographic changes appear
- Can show more extensive macular disease than is clinically visible (e.g. MEWDS)
- Demonstrates leading edges of atrophy in AMD, predicting disease progression
- Differentiates buried optic disc drusen from true disc swelling
Limitations
- Media opacities (cataracts, corneal haze) cause artifacts and signal reduction
- Low signal-to-noise ratio with standard fundus cameras (SLO preferred)
- Does not distinguish cause of hyper-AF (multiple conditions can look similar)
- Cannot assess choroidal vasculature (unlike ICGA)
- Requires patient cooperation for adequate image capture
"Limitations of FAF include a susceptibility to artifact from media opacities." — Kanski's Clinical Ophthalmology, 10th ed.
Summary
FAF is an indispensable, dye-free window into RPE metabolic health. It exploits lipofuscin fluorescence to yield a real-time map of RPE integrity. Hyperautofluorescence signals RPE stress/lipofuscin accumulation; hypoautofluorescence signals RPE loss or signal blockage. Its greatest clinical value lies in inherited retinal degenerations, AMD monitoring, inflammatory chorioretinopathies, and drug toxicity screening.
"Fundus autofluorescence has become particularly helpful in the diagnosis and management of retinal diseases and the clinical use is likely to expand in the future." — Kanski's Clinical Ophthalmology, 10th ed.
Sources cited:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Edition — Ch. 14 (Investigation of Macular Disease, p. 582), Ch. 12 (Uveitis investigations), Ch. 15 (Inherited retinal dystrophies)
- Wills Eye Manual — Ophthalmic Photographic Imaging Studies, §14.9
- Bradley & Daroff's Neurology in Clinical Practice — Ch. 43 (Fundus Autofluorescence Imaging, p. 872)
Note: Khurana's Comprehensive Ophthalmology and Zia's textbook were not available in the current library. The core principles described above are consistent across standard ophthalmology texts.
This is a shared conversation. Sign in to Orris to start your own chat.