What is fundus autoflorescens .take reference from zia , khurana & kanski
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information from Kanski's Clinical Ophthalmology (the authoritative source you requested), Wills Eye Manual, and Bradley & Daroff's Neurology. Note that "Zia" and "Khurana" are not present in the library — Kanski is well-covered. Here is the full answer:
Fundus Autofluorescence (FAF)
Note: The library contains Kanski's Clinical Ophthalmology (10th ed.) and Wills Eye Manual. Neither "Zia" nor "Khurana" ophthalmology textbooks are present in the database — the information below is sourced from Kanski and supplemented with Wills Eye Manual.
Definition & Principle
Fundus autofluorescence (FAF) is a non-invasive retinal imaging modality that records light emitted by native fluorophores in the retina after excitation by blue or green wavelength light.
The principal naturally occurring fluorophore is lipofuscin, contained within cytoplasmic granules of the retinal pigment epithelium (RPE) cells. Lipofuscin accumulates in RPE cells following photoreceptor degradation.
FAF imaging using an enhanced fundus camera or scanning laser ophthalmoscopy (SLO) permits visualization of accumulated lipofuscin in the RPE.
— Kanski's Clinical Ophthalmology, p. 582
Equipment
Images can be captured by:
- A properly equipped fundus camera
- An SLO-OCT machine
- A wide-field SLO — Bradley & Daroff's Neurology in Clinical Practice
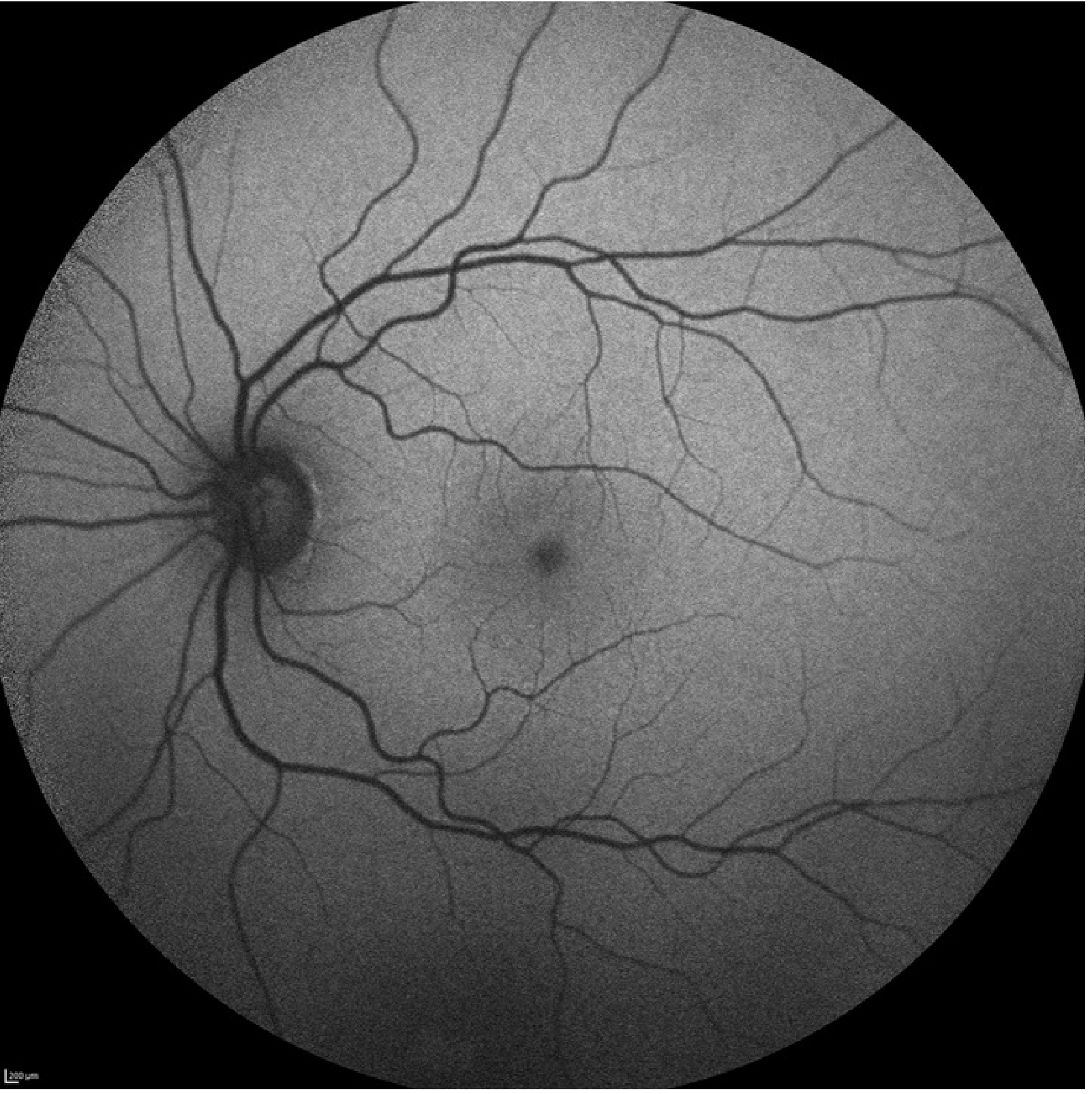
Normal FAF Appearance
A normal FAF image shows:
- Low-intensity background autofluorescence
- Reduced intensity at the fovea — due to absorption of blue light by macular luteal (xanthophyll) pigment
- Very dark optic nerve and blood vessels — contain no fluorophores
Abnormal Patterns
1. Hyperautofluorescence
Indicates RPE dysfunction and accumulation of lipofuscin. Seen in:
- Inherited retinal degenerations — particularly useful for diagnosis and follow-up
- More extensive macular disease than is visible clinically (e.g., MEWDS — Multiple Evanescent White Dot Syndrome)
- Geographic atrophy — distinct areas of hyperautofluorescence appear at the leading edges of lesions, seeming to precede retinal demise
2. Hypoautofluorescence
Indicates:
- Decreased lipofuscin
- Decreased RPE density
- Blockage of fluorescence (e.g., RPE atrophy, fibrosis)
— Kanski's Clinical Ophthalmology, p. 582
Clinical Applications
| Application | Details |
|---|---|
| Age-related macular degeneration (AMD) | Monitoring geographic atrophy and its progression |
| Inherited retinal dystrophies | Best first investigation along with OCT |
| Macular dystrophies | Early detection and monitoring |
| Medication toxicity | e.g., hydroxychloroquine toxicity screening |
| Ocular tumours | Evaluation of choroidal nevi and melanomas |
| Optic disc drusen | FAF can identify drusen at or slightly below the optic nerve head surface |
— Kanski's Clinical Ophthalmology, p. 582; Wills Eye Manual, p. 1098
Limitations
- Susceptible to artifact from media opacities (e.g., cataract, vitreous haemorrhage) — Kanski's Clinical Ophthalmology, p. 582
Key Clinical Tip (from Kanski)
"Fundus autofluorescence has become particularly helpful in the diagnosis and management of retinal diseases and the clinical use is likely to expand in the future." — Kanski's Clinical Ophthalmology, p. 582
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., p. 582
- Wills Eye Manual, p. 1098
- Bradley & Daroff's Neurology in Clinical Practice (supplementary)
This is a shared conversation. Sign in to Orris to start your own chat.