How can I measure QT Interval in an Ecg and what are the normal reference values
Reading File
Finding Sources
Finding Sources
Searching Images
QT interval measurement ECG
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive, well-sourced information. Here is a complete answer:
Measuring the QT Interval on an ECG
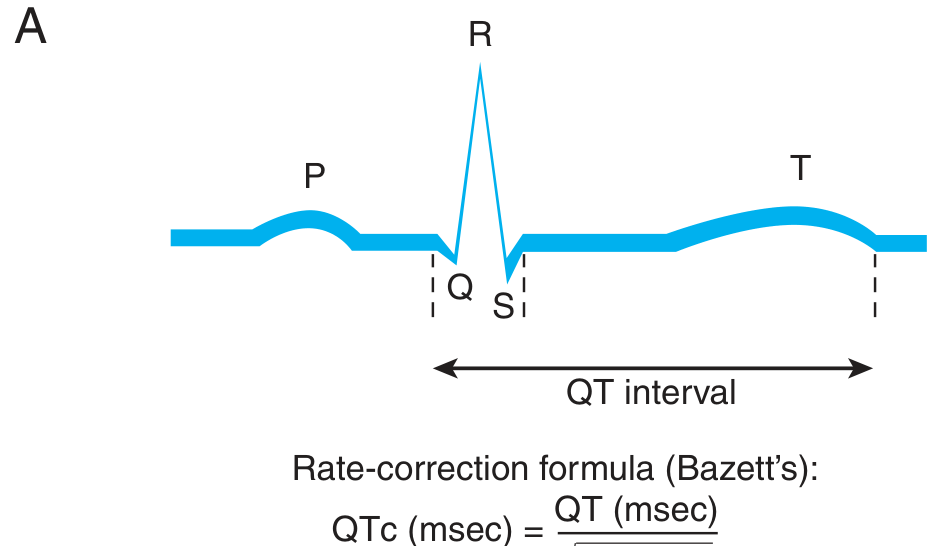
What the QT Interval Represents
The QT interval encompasses ventricular depolarization + repolarization — from the onset of the QRS complex to the end of the T wave. It reflects the total time for ventricular electrical activation and recovery.
Step-by-Step Measurement
- Choose the correct leads — measure in leads II, V5, and V6. Report the longest interval, averaged over 3–5 consecutive cycles.
- Identify the start point — the very first deflection of the QRS complex (the Q wave, or the beginning of the R wave if no Q is visible).
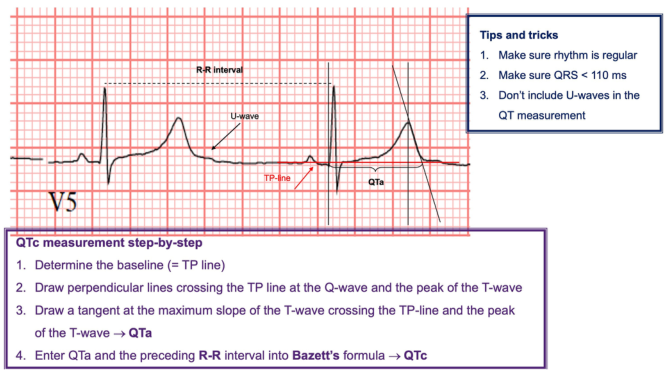
- Identify the end point — where the T wave returns to the isoelectric baseline (TP line). Use the tangent method: draw a line along the steepest descending slope of the T wave and note where it crosses the baseline.
- Handle U waves carefully — do not include U waves. If a U wave is present and merges with the T wave, extrapolate the T wave slope down to the baseline to find the true end.
- Ensure valid conditions before trusting the measurement:
- Rhythm must be regular
- QRS duration must be < 110 ms (wide QRS inflates QT)
Goldman-Cecil Medicine, International Edition
Rate Correction (QTc)
Because the QT interval shortens with faster heart rates, it must be corrected. Two formulas are used:
Bazett's formula (most widely used clinically):
$$QTc = \frac{QT}{\sqrt{RR}}$$
- QT and RR are both in seconds
- Works well at normal heart rates; overcorrects at high rates, undercorrects at low rates
Fridericia's formula (more accurate in atrial fibrillation and at extremes of heart rate):
$$QTc = \frac{QT}{\sqrt[3]{RR}}$$
For atrial fibrillation or irregular rhythms, average the QT over at least 3 beats and use an RR averaged over 10 cycles.
Goldman-Cecil Medicine, International Edition
Normal Reference Values
| Parameter | Normal / Threshold |
|---|---|
| Normal QTc (men) | ≤ 440–450 ms |
| Normal QTc (women) | ≤ 460 ms (slightly longer due to hormonal differences) |
| Prolonged QTc (men) | > 450 ms |
| Prolonged QTc (women) | > 460 ms |
| High-risk prolongation | > 500 ms (increased risk of torsades de pointes) |
| Short QT syndrome | < 320–340 ms (rare; associated with malignant arrhythmias) |
Women of all ages tend to have a slightly longer QTc than men of the same age. QTc can also vary across the day in the same individual.
Goldman-Cecil Medicine, International Edition
Wide QRS Adjustment
In patients with bundle branch block or other causes of QRS prolongation, the measured QT is artificially lengthened. A practical correction is:
Adjusted QT = Measured QT − (QRS duration − 80 ms)
Alternatively, use the JT interval (J point to T wave end) as a proxy for repolarization in these patients, though normal reference ranges for JT are less well established.
Clinical Pearls
- A QTc > 500 ms significantly raises the risk of torsades de pointes (polymorphic VT).
- Common acquired causes of QT prolongation: antiarrhythmics (sotalol, dofetilide, amiodarone), antipsychotics, macrolide antibiotics, hypokalemia, hypomagnesemia, and ischemia.
- Congenital long QT syndrome: at least 17 causative genes identified; LQT1, LQT2, and LQT3 (KCNQ1, KCNH2, SCN5A) account for ~90% of gene-positive cases.
Goldman-Cecil Medicine; Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.