Insulinoma work up
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive information. Let me compile the full insulinoma workup.
Insulinoma Workup
Overview
Insulinoma is the most common functional pancreatic endocrine neoplasm. Key facts:
- 90% are benign, solitary, sporadic adenomas
- 10% are malignant (lymph node or liver metastases)
- 10% are associated with MEN-1 (often multifocal, higher recurrence)
- Evenly distributed: 1/3 head/uncinate, 1/3 body, 1/3 tail
- <3% are ectopic (peripancreatic region)
Step 1 — Clinical Suspicion
Whipple's Triad
- Symptoms of hypoglycemia during fasting
- Documented serum glucose <50 mg/dL
- Relief of symptoms after glucose administration
Symptoms
| Category | Examples |
|---|---|
| Neuroglycopenic | Confusion, seizure, obtundation, personality change, coma, diplopia, weakness, amnesia |
| Adrenergic | Diaphoresis, trembling, palpitations, tachycardia |
Patients often learn to eat frequently to abort symptoms → weight gain/obesity is common. Symptoms can persist years before diagnosis.
Step 2 — Biochemical Confirmation
Initial Labs
- Fasting glucose + fasting insulin — if combined, insulin is inappropriately elevated in ~65% of insulinoma patients after overnight fast
- C-peptide — elevated in endogenous insulin excess; normal/low if exogenous insulin self-administration
- Proinsulin — elevated; most sensitive/specific criteria = fasting glucose <45 mg/dL + elevated proinsulin
- Insulin-to-glucose ratio — >0.3 supports insulinoma (normal <0.3)
Surreptitious Use Exclusion
| Cause | C-peptide | Other findings |
|---|---|---|
| Endogenous (insulinoma) | ↑ | ↑ proinsulin |
| Exogenous insulin | Low/normal | Possible anti-insulin antibodies (bovine/porcine) |
| Oral hypoglycemics (sulfonylureas) | ↑ | Toxicology screen positive |
Step 3 — Supervised 72-Hour Fast (Gold Standard Functional Test)
- Blood sampled every 4–6 hours for glucose and insulin
- Sample immediately when symptoms develop; stop test and give IV glucose
- 75–80% of insulinoma patients become symptomatic with glucose <40 mg/dL within 24 hours
- ~100% within 72 hours
- Diagnostic criteria during fast:
- Glucose <40–50 mg/dL with concurrent insulin >25 µU/mL
- Insulin:glucose ratio >0.3
Must be done with close supervision — can be dangerous. — Schwartz's Principles of Surgery
Step 4 — Localization Imaging
Once biochemical diagnosis is confirmed, localize and stage:
First-Line
| Modality | Notes |
|---|---|
| CT (multiphasic) | Standard first-line cross-sectional imaging |
| Endoscopic ultrasound (EUS) | >90% preoperative detection rate; highly sensitive for small pancreatic lesions |
Second-Line / Adjunct
| Modality | Indication |
|---|---|
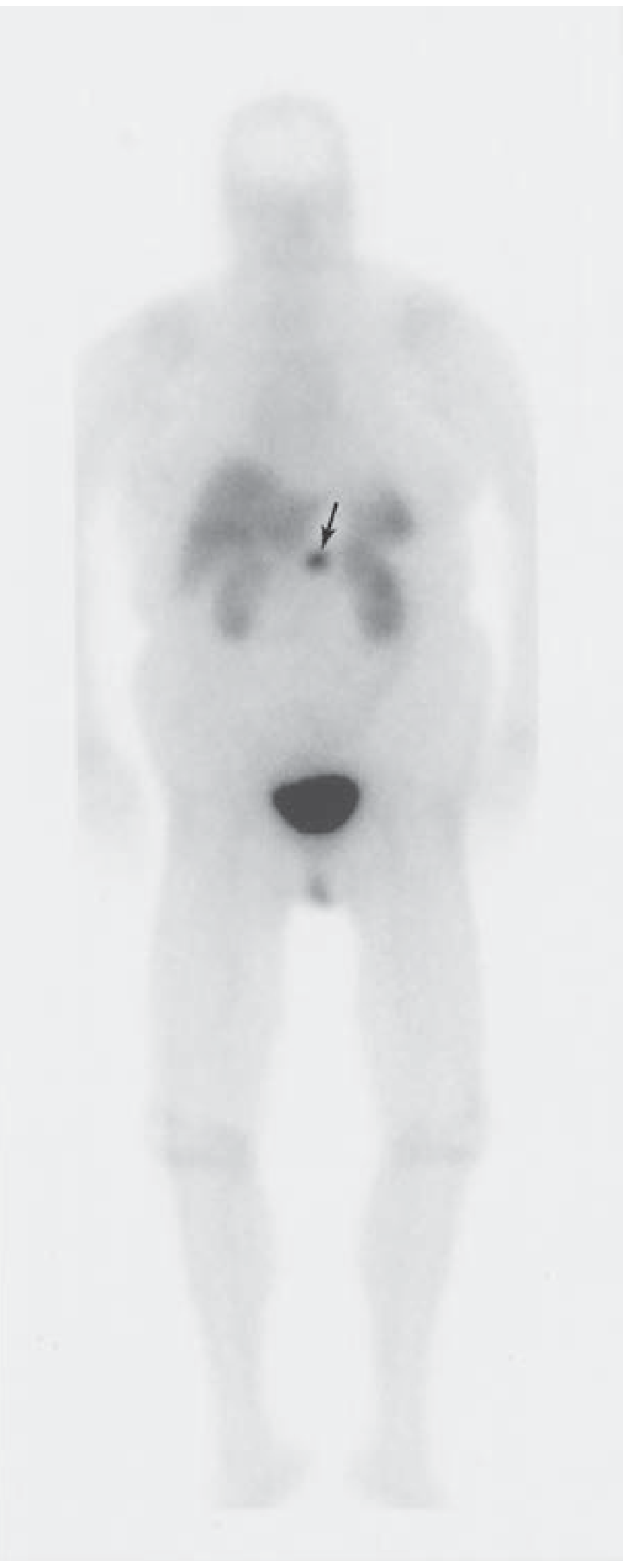
| Ga-68 DOTATATE PET scan (somatostatin receptor imaging) | Not routine — use if metastases suspected or tumor occult on other imaging |
| Hepatic venous sampling after arterial calcium stimulation | Rare; reserved for truly occult insulinoma |
| Visceral angiography with venous sampling | Rarely required |
Step 5 — MEN-1 Workup
- Screen for MEN-1 in all patients (esp. if multifocal tumors found on imaging or family history)
- MEN-1-associated insulinomas: more likely multifocal, higher surgical recurrence
- Check: serum calcium, PTH, pituitary MRI, parathyroid evaluation
Summary Algorithm
Clinical suspicion (Whipple's Triad)
↓
Fasting glucose + insulin + C-peptide + proinsulin
↓
Exclude exogenous causes (C-peptide low → exogenous insulin; toxicology → sulfonylureas)
↓
72-hour supervised fast (if biochemistry inconclusive)
↓
Biochemical confirmation → Localization
↓
CT (multiphasic) + EUS
↓
If occult: Ga-68 DOTATATE PET or arterial calcium stimulation/venous sampling
↓
Screen for MEN-1 if multifocal or familial
↓
Surgical resection (enucleation, distal pancreatectomy, or pancreaticoduodenectomy)
Sources: Mulholland and Greenfield's Surgery 7e, Schwartz's Principles of Surgery 11e, Sleisenger and Fordtran's GI and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.