Confocal microscope
confocal microscope principles applications 2025
https://ibidi.com/content/216-confocal-microscopy
Confocal Microscope
What Is It?
Principle of Operation
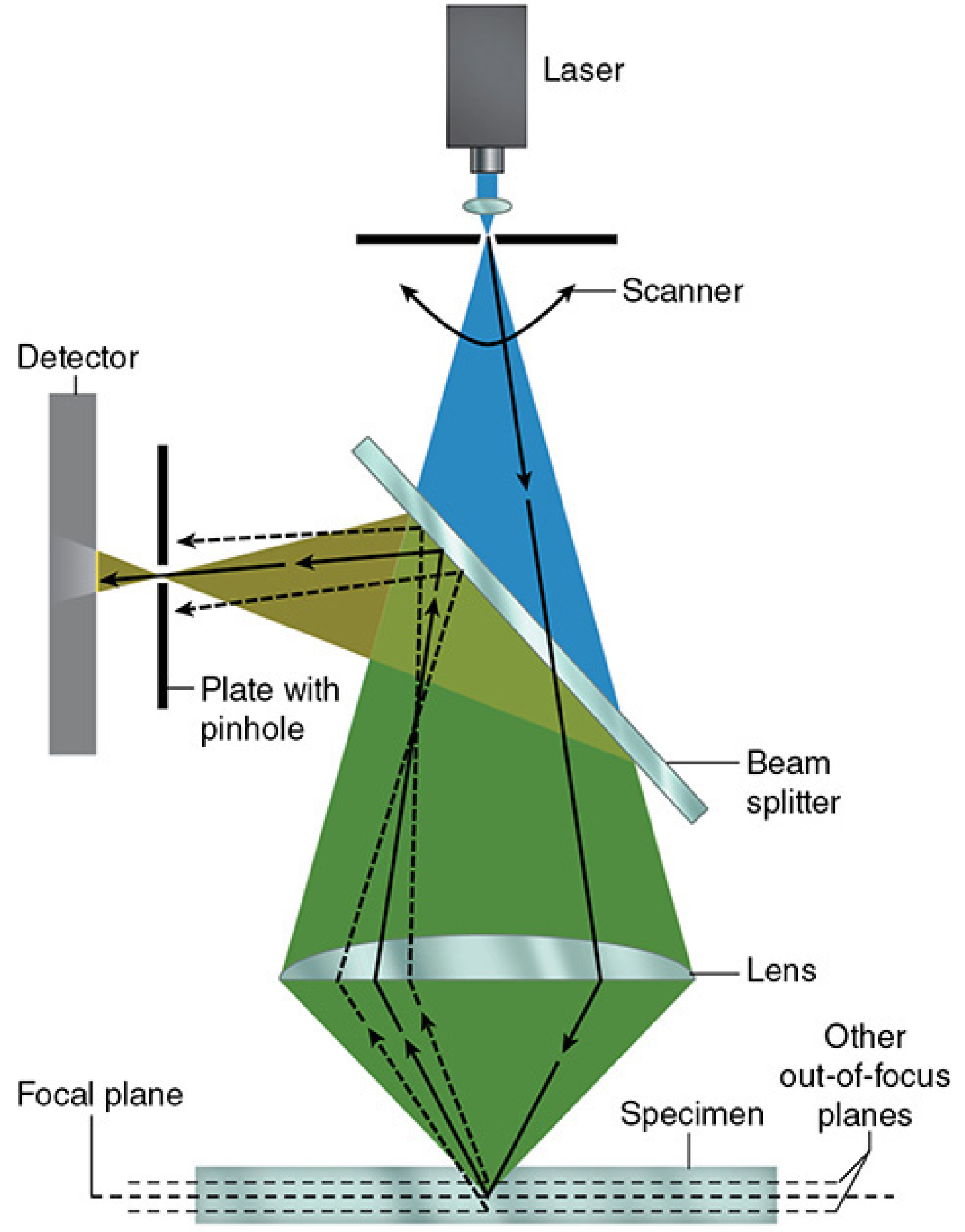
- A laser produces a coherent, monochromatic point source of light.
- The beam passes through a scanning system (galvanometer mirrors) that moves it in a raster pattern across the specimen.
- A beam splitter (dichromatic mirror) redirects excitation light toward the specimen and allows emitted fluorescence to pass through toward the detector.
- Emitted light from the specimen travels back through the optics and is focused onto a plate with a pinhole aperture in front of the detector.
- Only light from the focal plane passes cleanly through the pinhole. Light from planes above or below forms large, defocused disks that are physically blocked.
- A photomultiplier tube (PMT) or other detector captures the signal. A computer assembles the individual point measurements into a complete image.
"The point light source, the focal point of the lens, and the detector's pinpoint aperture are all optically conjugated or aligned to each other in the focal plane (confocal), and unfocused light does not pass through the pinhole." - Junqueira's Basic Histology, 17e
Key Components
| Component | Function |
|---|---|
| Laser | Provides intense, monochromatic, coherent point illumination |
| Scanner (galvanometer mirrors) | Rasters the beam across the specimen |
| Dichromatic mirror (beam splitter) | Separates excitation from emission light |
| Objective lens | Focuses laser to a diffraction-limited spot |
| Pinhole aperture | Blocks out-of-focus fluorescence at the detector plane |
| Photomultiplier tube (PMT) | Detects emitted photons with high sensitivity |
| Computer system | Assembles digital images; enables 3D reconstruction |
Optical Sectioning and 3D Reconstruction
Types of Confocal Microscopes
| Type | Mechanism | Notes |
|---|---|---|
| Laser Scanning Confocal (LSCM/CLSM) | Single beam scanned by galvanometer mirrors | Most common; ~1 frame/sec standard speed |
| Spinning Disk (Nipkow disk) | Rotating disk with arrays of pinholes and microlenses | Much faster; better for live-cell imaging; less phototoxicity |
| Resonant Scanning | Mirror oscillates at resonant frequency (~8 kHz) | Near-video speed; useful for fast dynamic events |
| Programmable Array Microscope (PAM) | Digital micromirror device | Flexible pinhole patterns |
| Airyscan (ZEISS) | 32-element detector array replacing single pinhole | Better signal-to-noise and ~1.7x resolution improvement |
Confocal vs. Widefield Microscopy
| Feature | Widefield | Confocal |
|---|---|---|
| Illumination | Full field | Point scanning |
| Detection | Camera-based | Detector with pinhole |
| Out-of-focus light | Present (blurs image) | Strongly rejected |
| Optical sectioning | No | Yes |
| Best for | Thin specimens, speed | Thick samples, 3D imaging |
| Live cell imaging | Excellent | Possible (faster with spinning disk) |
| Phototoxicity | Lower | Higher (LSCM) |
Applications
- Imaging subcellular structures (nuclei, mitochondria, cytoskeleton)
- Protein localization and co-localization studies
- Tracking intracellular signaling in live cells
- Visualization of neuronal networks and synaptic structures
- Dendritic spine morphology
- Calcium imaging
- Tumor architecture in 3D culture models (spheroids, organoids)
- Viability gradients and drug response
- Non-invasive in vivo "virtual biopsy" of the epidermis and papillary dermis
- Pre-histologic diagnosis of melanocytic tumors and skin cancers
- Guides biopsy site selection; reduces unnecessary excisions
- Monitors treatment response of neoplastic and inflammatory diseases
- (Dermatology 2-Volume Set, 5e)
- Studying bacterial and viral interactions with host cells (e.g., Bartonella in RBCs)
- Visualizing biofilm 3D architecture
- Surface profiling and roughness measurements
- Semiconductor and microelectronics inspection
Advantages
- High resolution with optical sectioning
- Elimination of out-of-focus background ("haze")
- Non-destructive 3D imaging of intact specimens
- Multi-channel fluorescence imaging (multiple labels simultaneously)
- Compatible with live cell imaging (especially spinning disk)
Limitations
- Slower image acquisition compared to widefield (LSCM)
- Phototoxicity and photobleaching from intense laser illumination
- Signal loss - the pinhole rejects some in-focus photons along with out-of-focus light
- Penetration depth limited to ~100-200 µm (deeper imaging requires multiphoton microscopy)
- Cost - significantly more expensive than conventional fluorescence microscopes
- In RCM for skin: limited penetration to upper dermis; thick stratum corneum (palmoplantar) restricts use
Recent Developments (2025)
- Evident launched the IXplore IX85 SpinXL and SpinSR spinning disk confocals in May 2025, expanding live-cell imaging capabilities
- ZEISS introduced Lightfield 4D in March 2025, a light-field microscopy system aimed at 4D imaging in neuroscience, cancer, and developmental biology
- Airyscan and STED super-resolution modes are increasingly integrated into standard confocal platforms, pushing resolution below the diffraction limit
- Junqueira's Basic Histology: Text and Atlas, 17e, p. 37-38
- Jawetz, Melnick & Adelberg's Medical Microbiology, 28e, p. 23
- Dermatology 2-Volume Set, 5e, pp. 41-42
- ibidi - Confocal Microscopy Principles
- Evident Scientific - Confocal Microscopy Principles
In ophthalmology
confocal microscopy ophthalmology cornea glaucoma clinical applications 2025
"confocal microscopy" AND ophthalmology
"in vivo confocal microscopy" AND cornea
Confocal Microscopy in Ophthalmology
Overview
"The confocal microscope optically sections the cornea to noninvasively obtain structural information of the different corneal layers." - Wills Eye Manual, 6e
Instruments Used
| Instrument | Type | Notes |
|---|---|---|
| HRT-II Rostock Cornea Module (Heidelberg) | Laser scanning | Most widely used in research and clinical practice |
| ConfoScan 4 (NIDEK) | Slit-scanning | White-light source; wider field of view |
| VivoScan (Nidek) | Updated slit-scan platform |
Layers of the Cornea Imaged
- Epithelium - superficial, wing, and basal cells; goblet cell infiltration in limbal stem cell deficiency (LSCD)
- Bowman's layer - acellular; disrupted in dystrophies and post-refractive surgery
- Stroma - keratocyte nuclei, extracellular matrix, nerve fiber bundles
- Sub-basal nerve plexus (SNP) - the densest accessible peripheral nerve network in the body; visible as a branching fiber layer between epithelium and Bowman's layer
- Descemet's membrane - usually transparent
- Endothelium - hexagonal cell mosaic; cell density counts
Clinical Applications
1. Infectious Keratitis
"Other investigations include immunohistochemistry, PCR and in vivo confocal microscopy. Corneal biopsy may be necessary for diagnosis." - Kanski's Clinical Ophthalmology, 10e "In cases of Acanthamoeba keratitis, they can be visualized in corneal scrapings and by confocal microscopy in vivo in the cornea on examination by an expert ophthalmologist." - Red Book 2021
- Visualizes fungal filaments/hyphae within corneal stroma in real time
- Useful when scraping cultures are negative or slow to grow
- "Confocal microscopy frequently permits identification of organisms in vivo, but is not widely available outside tertiary centres." - Kanski's Clinical Ophthalmology, 10e
- IVCM identifies the obligate intracellular organisms in immunocompromised patients (Wills Eye Manual)
- Complements Gram stain and Giemsa staining
2. Corneal Endothelial Assessment
- Endothelial cell density (ECD) - normal ~2500-3000 cells/mm²; critical threshold for corneal decompensation ~500-800 cells/mm²
- Cell morphology - hexagonality (normal >60%), coefficient of variation in cell size (polymegethism and pleomorphism)
- Pre- and post-operative monitoring (cataract surgery, keratoplasty, anterior chamber IOLs)
- Assessment in Fuchs' endothelial dystrophy and iridocorneal endothelial (ICE) syndrome
3. Corneal Dystrophies and Deposits
- Granular dystrophy - bright, discrete stromal deposits
- Macular dystrophy - diffuse hazy deposits in keratocyte cytoplasm
- Lattice dystrophy - reflective linear deposits (amyloid)
- Map-dot-fingerprint (EBMD) - epithelial maps, dots, fingerprint patterns
- Mucopolysaccharidoses - stromal haze and keratocyte changes
- Darier-White disease - corneal involvement documented by IVCM
4. Limbal Stem Cell Deficiency (LSCD)
"Conjunctivalization of cornea with goblet cells (confirmed with confocal microscopy, impression cytology with acid Schiff stain or monoclonal antibody against cytokeratin 19)." - Kanski's Clinical Ophthalmology, 10e
- Confirm LSCD diagnosis
- Grade severity and extent
- Monitor response to stem cell transplantation
5. Corneal Nerve Assessment
"Corneal confocal microscopy assesses corneal nerve fiber and nerve branch density and significantly correlates with IENFD [intraepidermal nerve fiber density] in patients with small-fiber neuropathy... In diabetics, reduced corneal sensation and corneal nerve fiber and nerve branch density correlates with disease duration and with IENFD." - Bradley & Daroff's Neurology, 7e
- Corneal nerve fiber density (CNFD) - number of fibers per mm²
- Corneal nerve branch density (CNBD)
- Corneal nerve fiber length (CNFL) - total length per frame
- Diagnosing and staging diabetic neuropathy
- Monitoring chemotherapy-induced neuropathy
- Small-fiber neuropathy assessment (correlates with skin punch biopsy IENFD)
- Gulf War Illness (corneal nerve biomarkers - AAO 2025)
- Multiple sclerosis, Parkinson's disease, and other neurodegenerative research
6. Ocular Allergy and Inflammatory Conditions
- Vernal and atopic keratoconjunctivitis - identifying eosinophil infiltration, dendritic cell density
- Monitoring treatment response in allergic eye disease
- Dry eye disease - assessment of corneal nerve changes and inflammatory cell infiltration
7. Contact Lens-Related Changes
- Monitoring keratocyte activation and stromal changes from extended wear
- Detecting early subclinical microbial keratitis
- Evaluating corneal nerve recovery after lens discontinuation
8. Pre- and Post-Surgical Evaluation
- Refractive surgery (LASIK, PRK) - sub-basal nerve plexus regeneration monitoring, keratocyte activation in the ablation zone
- Penetrating keratoplasty / DSAEK / DMEK - endothelial cell density in donor and recipient corneas
- Keratoconus - stromal architecture, Vogt's striae at cellular level
Advantages
- Non-invasive - no biopsy required; in vivo, real-time imaging
- Cellular resolution (~1-2 µm lateral, ~5-10 µm axial)
- All corneal layers visible from epithelium to endothelium
- Repeat imaging possible for longitudinal monitoring
- Unique access to the sub-basal nerve plexus - a peripheral nerve network accessible non-invasively in no other way
Limitations
- Depth limited to ~500 µm (full corneal thickness) - cannot image anterior chamber or lens
- Field of view narrow (~400 x 400 µm per frame)
- Contact probe required (topical anesthetic + coupling gel); patient cooperation needed
- Not widely available outside tertiary centres (Kanski's)
- Operator skill affects image quality and interpretation
- Thick stratum corneum (palmoplantar) limits usefulness - not relevant here but limbal or conjunctival areas can be difficult
- AI-assisted automated nerve quantification is actively being developed to reduce observer variability (PMID 39198101)
Summary Table
| Application | What IVCM Detects | Clinical Impact |
|---|---|---|
| Acanthamoeba keratitis | Cysts and trophozoites in stroma | Diagnosis without biopsy |
| Fungal keratitis | Hyphae / filaments | Avoids delay; guides treatment |
| Corneal endothelium | ECD, morphology | Pre-op planning, dystrophy staging |
| Corneal dystrophies | Layer-specific deposits | Avoids diagnostic biopsy |
| LSCD | Goblet cells in epithelium | Confirms diagnosis, grades severity |
| Diabetic neuropathy | Sub-basal nerve plexus | Surrogate for skin biopsy IENFD |
| Contact lens changes | Keratocyte/nerve changes | Safety monitoring |
| Post-refractive surgery | Nerve regeneration | Recovery assessment |
| Ocular allergy | Inflammatory cells, dendritic cells | Treatment monitoring |
- Wills Eye Manual, 6e - Section 14.14
- Kanski's Clinical Ophthalmology, 10e - Fungal Keratitis & Acanthamoeba Keratitis
- Bradley & Daroff's Neurology in Clinical Practice, 7e - Small-Fiber Neuropathy
- Red Book 2021 - Acanthamoeba
- Rozitis et al. (2025), Clin Exp Ophthalmol, PMID 40433731 - Corneal deposits by IVCM
- Simsek et al. (2024), Turk J Ophthalmol, PMID 39743938 - IVCM in ocular allergies
- AAO 2025 - Session 233: Anterior Segment OCT and IVCM in Corneal Diseases
Create poster
A professional clinical ophthalmology educational poster titled "In Vivo Confocal Microscopy (IVCM) in Ophthalmology" for clinicians. Clean, modern medical design with a dark navy blue and teal color scheme with white text. Layout has these clearly labeled sections arranged in a grid: TOP: Large bold title "In Vivo Confocal Microscopy (IVCM) in Ophthalmology" with subtitle "Non-invasive cellular-resolution imaging of the living cornea" LEFT COLUMN: Section "Principle" with icon of eye and laser beam: Point laser illumination + pinhole aperture eliminates out-of-focus light. Optically sections all corneal layers from epithelium to endothelium (~500 µm depth). Resolution: 1–2 µm lateral. Section "Corneal Layers Imaged" as a vertical stack diagram showing: Epithelium → Bowman's Layer → Stroma (keratocytes + nerves) → Sub-Basal Nerve Plexus → Descemet's Membrane → Endothelium MIDDLE COLUMN - "Clinical Applications" as icons with labels: 🦠 Infectious Keratitis: Acanthamoeba cysts, fungal hyphae identified in vivo 👁 Endothelial Assessment: Cell density (ECD), hexagonality, pleomorphism ⚡ Corneal Dystrophies: Layer-specific deposits without biopsy 🌿 Corneal Nerves: Sub-basal nerve plexus — diabetic neuropathy biomarker 💧 LSCD: Goblet cell infiltration confirms limbal stem cell deficiency 💊 Post-Surgical: Nerve regeneration after LASIK/PRK, DMEK monitoring RIGHT COLUMN: "Key Nerve Parameters" box: • CNFD – Corneal Nerve Fiber Density • CNBD – Corneal Nerve Branch Density • CNFL – Corneal Nerve Fiber Length Correlates with skin biopsy IENFD in diabetic neuropathy "Advantages vs Limitations" two-column mini-table: Advantages: Non-invasive, real-time, all layers, repeatable, no biopsy Limitations: Narrow FOV (~400×400 µm), contact probe, limited to cornea, tertiary centre access BOTTOM BAR: "Instruments: HRT-II Rostock Module (laser) | ConfoScan 4 (slit-scanning)" and sources line in small text Use microscopy-style circular image placeholders showing blue-teal honeycomb endothelium cells and branching nerve fibers as decorative elements. Professional academic poster style.
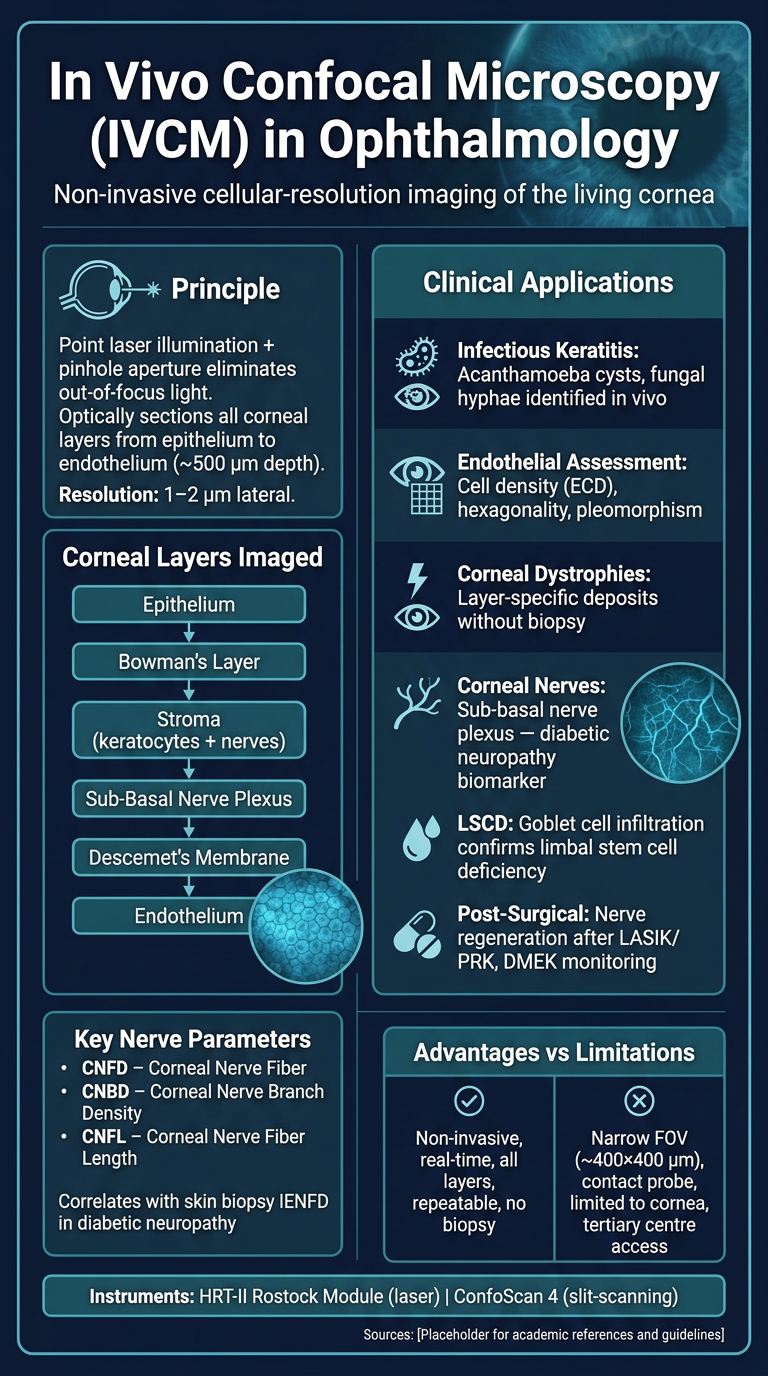
- Principle - point laser + pinhole optical sectioning
- Corneal layers imaged - epithelium to endothelium
- Key clinical applications - infectious keratitis (Acanthamoeba, fungi), endothelial assessment, dystrophies, nerve plexus imaging, LSCD, and post-surgical monitoring
- Corneal nerve parameters (CNFD, CNBD, CNFL) with the diabetic neuropathy link
- Advantages vs. limitations summary
- Instruments used clinically