Conservative management of acute cholecystitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to provide a thorough answer. Here is the synthesized response:
Conservative Management of Acute Cholecystitis
When is Conservative Management Indicated?
Cholecystectomy is the definitive treatment for acute cholecystitis, but non-operative (conservative) management is reserved for specific scenarios:
- Patients presenting in a delayed fashion (>72 hours, when inflammation is well-established)
- Patients with significant medical comorbidities that make surgery high-risk (heart failure, severe cardiopulmonary disease)
- Patients who are critically ill (Grade III disease) requiring stabilization before any intervention
- As an initial "cool-down" period in Grade II disease before interval cholecystectomy
— Sabiston Textbook of Surgery, p. 1831; Sleisenger and Fordtran's, p. 1263
Tokyo Guidelines Severity Grading (TG18)
| Grade | Criteria |
|---|---|
| I (Mild) | No organ dysfunction; symptoms <72 h; low operative risk |
| II (Moderate) | WBC >18,000/mm³; palpable RUQ mass; symptoms >72 h; or marked local inflammation (gangrenous cholecystitis, pericholecystic abscess) |
| III (Severe) | Organ dysfunction: circulatory failure, neurologic disturbance, respiratory failure (PaO₂/FiO₂ <300), renal failure (creatinine >2.0 mg/dL), hepatic failure (INR >1.5), thrombocytopenia (<100,000/mm³) |
— Current Surgical Therapy, p. 513
Components of Conservative Management
1. IV Fluids and Resuscitation
- Start IV hydration immediately to restore tissue perfusion and correct electrolyte imbalances.
- Maintain NPO (nothing by mouth) status.
2. Analgesia
- Parenteral opioids (e.g., morphine, fentanyl) are usually required for pain control.
3. Antibiotic Therapy
Antibiotics are essential — bile or gallbladder wall cultures are positive for bacteria in >40% of patients.
Target organisms: E. coli, Klebsiella, Enterobacter, Bacteroides spp.
| Severity | Antibiotic Regimen |
|---|---|
| Mild–moderate | Cefoxitin (single-agent cephalosporin) |
| Severe | Piperacillin-tazobactam or 3rd-generation cephalosporin + metronidazole |
| Gangrenous/emphysematous | Must include anaerobic coverage |
- If source control is achieved surgically, postoperative antibiotics are not needed in mild-to-moderate disease.
- Continue antibiotics postoperatively for: severe infection, intraoperative gallbladder perforation, or gangrenous cholecystitis.
— Sleisenger and Fordtran's, p. 1263; Sabiston, p. 1831
4. Close Clinical Monitoring
- Watch for failure of conservative therapy (worsening pain, fever, rising WBC, peritonitis).
- ~25% of medically managed patients develop a complication despite conservative treatment — these require urgent surgical intervention.
- Of those who do remit (75%), ~25% experience recurrence within 1 year and 60% within 6 years.
— Harrison's Principles of Internal Medicine 22E, p. ~357
Natural History Under Conservative Management
Approximately 75% of patients treated medically will have remission of acute symptoms within 2–7 days of hospitalization. — Harrison's
However, ~20% of patients initially admitted for conservative management fail to respond and require unplanned surgical intervention before the planned interval procedure. — Sabiston, p. 1831
Percutaneous Cholecystostomy — When Antibiotics Alone Fail
For patients who fail antibiotic and supportive therapy and are not candidates for cholecystectomy, percutaneous cholecystostomy tube placement is the next step:
- Preferred for: critically ill patients, poor performance status (Charlson Comorbidity Index ≥6 or ASA class ≥3)
- Provides gallbladder drainage and source control without general anaesthesia
- After stabilization, interval cholecystectomy is recommended unless the patient has very poor expected survival (CCI ≥4 + limited life expectancy), in which case observation alone is appropriate
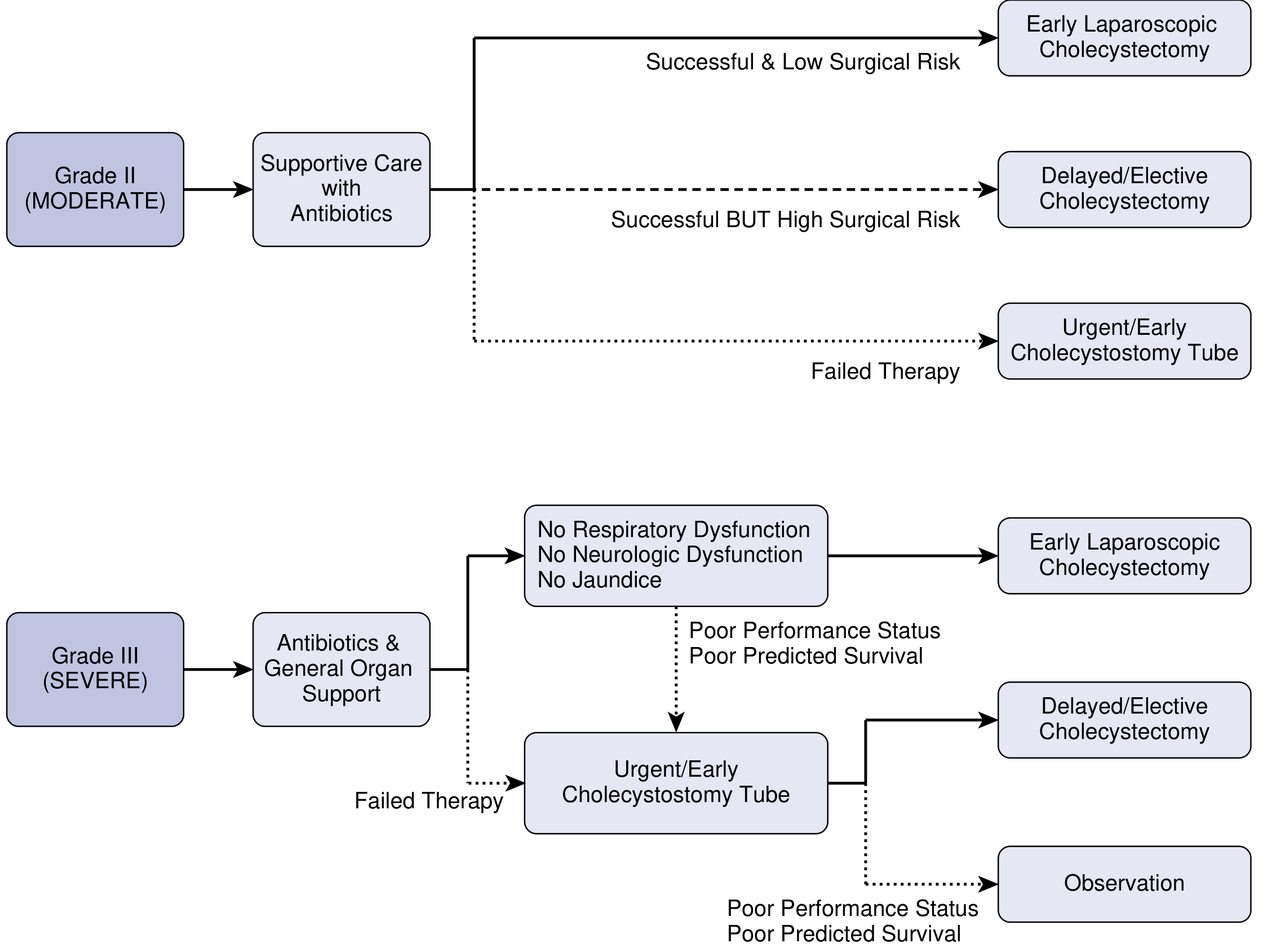
Tokyo Guidelines 2018 flowchart for Grade II and III acute cholecystitis management. — Current Surgical Therapy, p. 513
Interval Cholecystectomy After Conservative Management
For patients who respond to conservative therapy, elective laparoscopic cholecystectomy should be planned:
- Traditionally performed 6–8 weeks after the acute episode ("cool-down" period).
- However, multiple RCTs show early cholecystectomy (within 3 days) is equally safe with fewer total hospital days (9.6 vs. 17.8 days) and avoids the 26% failure rate of the delayed approach.
- The delayed approach carries a 2% mortality rate vs. 0% for the early approach in combined trial data.
— Sleisenger and Fordtran's, p. 1263 (Table 90.4)
Special Populations
- Elderly/high-comorbidity patients (e.g., heart failure): benefit most from initial non-operative approach followed by definitive surgery when optimised. — Sleisenger and Fordtran's
- Pregnancy: Conservative care is the mainstay; second trimester is preferred for cholecystectomy if surgery becomes necessary. — Swanson's Family Medicine Review
- Acalculous cholecystitis: Conservative management principles are the same, but underlying triggers (prolonged fasting, critical illness, parenteral nutrition, burns) must also be addressed.
Summary Algorithm
Acute Cholecystitis
├── Grade I (Mild) → Early laparoscopic cholecystectomy (preferred)
├── Grade II (Moderate)
│ ├── Antibiotics + supportive care
│ │ ├── Success + low surgical risk → Early cholecystectomy
│ │ ├── Success + high surgical risk → Delayed/elective cholecystectomy
│ │ └── Failed → Urgent percutaneous cholecystostomy
└── Grade III (Severe)
├── Antibiotics + organ support
│ ├── Resolves (no resp/neuro dysfunction) → Early cholecystectomy
│ └── Poor performance → Cholecystostomy → Delayed surgery or observation
└── Failed therapy → Urgent cholecystostomy
This is a shared conversation. Sign in to Orris to start your own chat.