All ECG Findings
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching Images
ECG findings normal waveform P wave QRS ST segment T wave
Searching the Web
all ECG findings comprehensive list interpretation clinical
Reading Web Page
https://geekymedics.com/how-to-read-an-ecg/
Searching Images
12-lead ECG ST elevation STEMI inferior lateral anterior findings
Searching Images
atrial fibrillation flutter bundle branch block ECG arrhythmia
Searching Images
Wolff Parkinson White delta wave long QT hypokalemia hyperkalemia ECG
Here is a comprehensive reference of all major ECG findings, organized systematically for clinical interpretation.
All ECG Findings — Comprehensive Reference
🔬 Systematic Approach to ECG Reading
Always read an ECG in this order: Rate → Rhythm → Axis → Intervals → P waves → QRS → ST segment → T waves → U waves → Special waves
1. RATE
| Finding | Value | Significance |
|---|---|---|
| Normal sinus rate | 60–100 bpm | Normal |
| Sinus bradycardia | < 60 bpm | Vagal tone, athletes, hypothyroidism, β-blockers, sick sinus syndrome |
| Sinus tachycardia | > 100 bpm | Pain, fever, sepsis, hypovolemia, hyperthyroidism, PE, anxiety |
2. RHYTHM
Normal
- Normal Sinus Rhythm (NSR): Regular P waves before every QRS, rate 60–100 bpm, PR 120–200 ms
Atrial Arrhythmias
| Rhythm | ECG Features | Causes |
|---|---|---|
| Sinus arrhythmia | P-wave morphology normal; R-R varies with breathing | Normal variant (especially young) |
| Atrial premature complex (APC) | Early P wave with abnormal morphology | Caffeine, stress, structural heart disease |
| Atrial tachycardia | P waves present, rate 150–250 bpm, abnormal P morphology | Digoxin toxicity, structural disease |
| Multifocal atrial tachycardia (MAT) | ≥3 distinct P-wave morphologies, irregular, rate >100 | COPD, electrolyte imbalance |
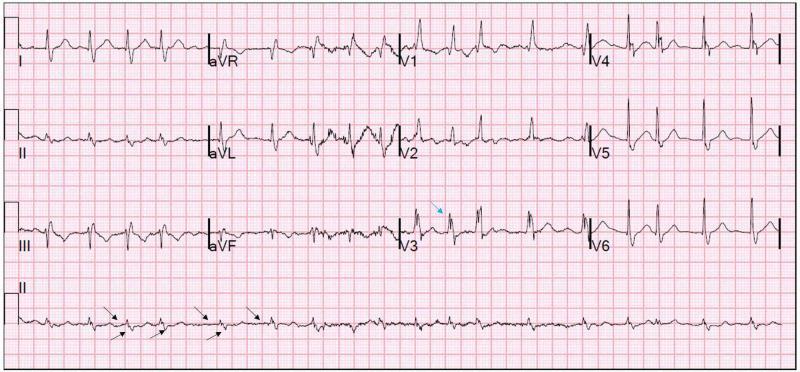
| Atrial flutter | Sawtooth flutter waves (~300 bpm) in II, III, aVF; ventricular rate typically 150 bpm (2:1 block) | Structural disease, post-cardiac surgery |
| Atrial fibrillation (AF) | Absent P waves, irregularly irregular rhythm, fibrillatory baseline | HTN, valvular disease, thyrotoxicosis, alcohol, HF |
AV Block (Heart Block)
| Block | PR Interval | Dropped QRS? | Notes |
|---|---|---|---|
| 1st degree | Fixed, > 200 ms | No | Benign; ↑ vagal tone, inferior MI, digoxin |
| 2nd degree – Mobitz I (Wenckebach) | Progressive lengthening → dropped QRS | Yes, periodically | Usually benign; below AV node |
| 2nd degree – Mobitz II | Fixed PR, intermittent dropped QRS (2:1, 3:1) | Yes | Serious; below Bundle of His → risk of complete block |
| 3rd degree (Complete) | P waves and QRS completely dissociated | Yes (all) | Junctional/ventricular escape rhythm; emergency |
Ventricular Arrhythmias
| Rhythm | ECG Features | Significance |
|---|---|---|
| PVC (premature ventricular complex) | Wide, bizarre QRS, no preceding P wave, compensatory pause | Common; if frequent or R-on-T → malignant |
| Ventricular tachycardia (VT) | Wide QRS (>120 ms), rate >100, AV dissociation, fusion/capture beats | Life-threatening |
| Ventricular fibrillation (VF) | Chaotic, irregular deflections; no organized waveforms | Cardiac arrest |
| Torsades de pointes | Twisting QRS axis around baseline; long QT preceding | Drug-induced, electrolyte disorders |
| Accelerated idioventricular rhythm (AIVR) | Wide QRS 40–100 bpm, no P waves | Post-reperfusion, benign |
| Asystole | Flat line; no P waves or QRS | Cardiac arrest |
Pre-excitation Syndromes
| Finding | Features | Cause |
|---|---|---|
| WPW (Wolff-Parkinson-White) | Short PR (<120 ms), delta wave (slurred QRS upstroke), wide QRS | Accessory pathway (Bundle of Kent) → risk of AF with rapid conduction |
3. CARDIAC AXIS
| Axis | Lead I | Lead aVF | Causes |
|---|---|---|---|
| Normal (-30° to +90°) | Positive | Positive | Normal |
| Left axis deviation (LAD) (> -30°) | Positive | Negative | LBBB, LAFB, inferior MI, LVH |
| Right axis deviation (RAD) (> +90°) | Negative | Positive | RBBB, RVH, PE, LPFB, lateral MI |
| Extreme axis (NW axis) | Negative | Negative | VT, severe RVH, artifact |
4. P WAVE ABNORMALITIES
| Finding | Features | Cause |
|---|---|---|
| P mitrale | Wide (>120 ms), bifid (notched) P in lead II; negative terminal component in V1 | Left atrial enlargement (e.g., mitral stenosis) |
| P pulmonale | Tall (>2.5 mm), peaked P in II, III, aVF | Right atrial enlargement (e.g., COPD, tricuspid stenosis, RVH) |
| Absent P waves | No visible P waves | AF, junctional rhythm, hyperkalemia (severe) |
| Retrograde P waves | P negative in II, III, aVF; follows QRS | Junctional tachycardia |
5. PR INTERVAL
| Finding | Duration | Cause |
|---|---|---|
| Normal | 120–200 ms | — |
| Short PR (<120 ms) | <120 ms | WPW, LGL syndrome, junctional rhythm |
| Prolonged PR (>200 ms) | >200 ms | 1st degree AV block, digoxin, inferior MI |
6. QRS COMPLEX
Duration / Width
| Finding | Duration | Features | Cause |
|---|---|---|---|
| Narrow QRS | < 120 ms | Normal conduction | — |
| RBBB (Right Bundle Branch Block) | ≥ 120 ms | RSR' (M-shape/"bunny ears") in V1; wide S in I, V6 | Pulmonary embolism, RVH, congenital, ischemia |
| LBBB (Left Bundle Branch Block) | ≥ 120 ms | Broad, notched R in I, aVL, V5–V6; deep S/QS in V1; T-wave discordance | IHD, cardiomyopathy, hypertension; may mask STEMI |
| LAFB (Left anterior fascicular block) | Normal | LAD, small Q in I/aVL, small R in III | Common; usually benign |
| LPFB (Left posterior fascicular block) | Normal | RAD, small R in I/aVL, small Q in III | Rarer; associated with extensive MI |
Amplitude / Morphology
| Finding | Features | Cause |
|---|---|---|
| Low voltage | QRS amplitude < 5 mm in all limb leads, < 10 mm in precordial leads | Pericardial effusion, obesity, COPD, amyloidosis, hypothyroidism |
| Electrical alternans | Alternating QRS axis/amplitude | Large pericardial effusion/tamponade |
| Pathological Q waves | > 25% of R wave height, ≥ 40 ms wide | Prior MI (transmural infarction), LBBB, WPW |
| Poor R-wave progression (PRWP) | Failure of R wave to grow V1→V4 | Anterior MI, LBBB, RVH, COPD |
| LVH (Left ventricular hypertrophy) | S in V1 + R in V5 or V6 ≥ 35 mm (Sokolow-Lyon); tall R in aVL ≥ 11 mm | Hypertension, AS, HCM |
| RVH (Right ventricular hypertrophy) | R > S in V1; RAD; deep S in V6 | Pulmonary HTN, COPD, PS, ASD |
| Delta wave | Slurred initial QRS upstroke | WPW |
| Epsilon wave | Small positive deflection at end of QRS in V1–V3 | Arrhythmogenic right ventricular cardiomyopathy (ARVC) |
| J wave (Osborn wave) | Positive deflection at J-point (junction of QRS and ST) | Hypothermia (pathognomonic), Brugada |
| Fragmented QRS (fQRS) | Notching/slurring of QRS in ≥2 contiguous leads | Myocardial fibrosis/scar, prior MI |
7. ST SEGMENT
| Finding | Features | Cause |
|---|---|---|
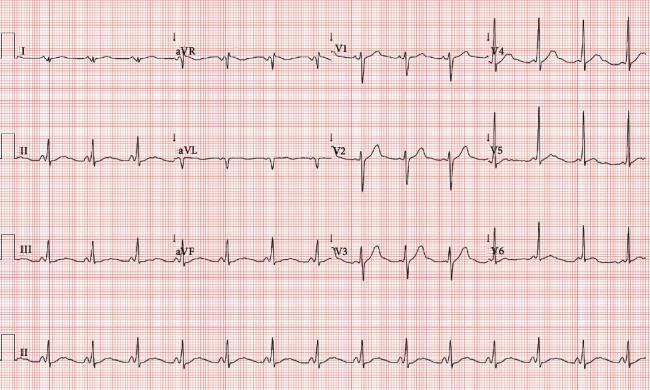
| ST elevation (STE) | Convex (tombstone) morphology in contiguous leads ≥1 mm | STEMI, vasospasm (Prinzmetal), LV aneurysm |
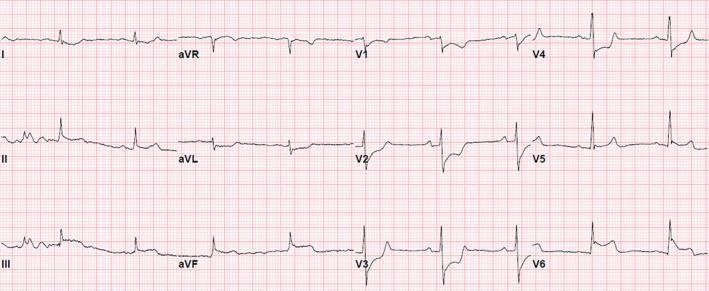
| Inferior STEMI | STE in II, III, aVF + reciprocal STD in I, aVL | RCA or LCx occlusion |
| Anterior STEMI | STE in V1–V4 | LAD occlusion |
| Lateral STEMI | STE in I, aVL, V5–V6 | LCx, diagonal branch occlusion |
| Posterior MI | STD in V1–V3 (= reciprocal); tall R in V1–V2 | LCx/RCA (posterior territory) |
| ST depression (STD) | Horizontal or downsloping ≥ 0.5 mm | Subendocardial ischemia/NSTEMI, digoxin effect (reverse tick), LVH strain |
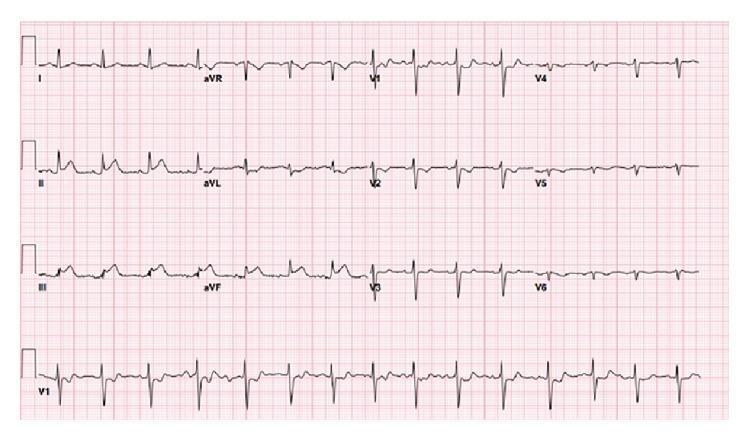
| Saddle-shaped (concave) STE | Diffuse, saddle-shaped ST elevation in most leads (not just contiguous) | Pericarditis |
| Brugada pattern | Coved-type (type 1) STE with RBBB morphology in V1–V2 | Brugada syndrome (VF risk) |
| Early repolarization | Concave STE + J-point notching, most prominent V2–V5 | Normal variant (young, athletic males); occasionally malignant |
| de Winter T waves | Upsloping STD + tall, symmetric T waves in V1–V6 (without STE) | Proximal LAD occlusion equivalent |
8. QT INTERVAL
| Finding | QTc | Cause |
|---|---|---|
| Normal QTc | 350–440 ms (♂), 350–460 ms (♀) | — |
| Prolonged QT (QTc > 440/460 ms) | > 440 ms ♂, > 460 ms ♀ | Drugs (amiodarone, sotalol, haloperidol, azithromycin, quinolones, TCA), hypokalemia, hypomagnesemia, hypocalcemia, congenital LQTS → risk of Torsades |
| Short QT (QTc < 360 ms) | < 360 ms | Hypercalcemia, hyperkalemia, acidosis, hyperthermia, Short QT syndrome, digoxin |
9. T WAVE ABNORMALITIES
| Finding | Features | Cause |
|---|---|---|
| Normal T wave | Upright in I, II, V3–V6; inverted in aVR; variable in III, aVL, V1–V2 | — |
| Tall/peaked T waves | > 5 mm in limb leads, > 10 mm in precordial | Hyperkalemia (early/tent-shaped), hyperacute MI, vagotonia |
| Inverted T waves | Downward deflection (in leads where normally upright) | Ischemia/NSTEMI, PE (V1–V4), RVH (V1–V3), cardiomyopathy, CNS events (deep symmetric inversion), RBBB, digoxin |
| Wellens syndrome T waves | Deep symmetric T inversions (type A: biphasic) or (type B: deeply inverted) in V2–V3 | Critical proximal LAD stenosis (pre-infarction pattern) |
| Flat T waves | Non-specific | Ischemia, hypokalemia, LVH strain |
| Biphasic T waves | Two-phase deflection | Ischemia, hypokalemia, Wellens |
10. U WAVES
| Finding | Features | Cause |
|---|---|---|
| Normal U wave | Small positive deflection after T wave, best in V2–V3 | Purkinje fiber repolarization |
| Prominent U waves | Tall U waves > T wave | Hypokalemia (classic), hypomagnesemia, bradycardia, digoxin, amiodarone |
| Inverted U waves | Negative U | Ischemia, LVH |
11. ELECTROLYTE & METABOLIC PATTERNS
| Condition | ECG Pattern |
|---|---|
| Hyperkalemia | Peaked T waves → widened QRS → sine-wave pattern → asystole/VF |
| Hypokalemia | Flattened T waves, prominent U waves, ST depression, long QU interval |
| Hypercalcemia | Short QT interval, shortened ST segment |
| Hypocalcemia | Long QT (prolonged ST segment) |
| Hypomagnesemia | Long QT, Torsades de pointes |
| Hypermagnesemia | Prolonged PR, widened QRS, heart block |
| Hypothyroidism | Sinus bradycardia, low voltage, prolonged QT, flat T waves |
| Hypothermia | Osborn (J) waves, sinus bradycardia, slow AF, long QT |
| Digoxin effect | Reverse-tick (scooped) ST depression, short QT, flat T waves |
| Digoxin toxicity | PAT with block, bidirectional VT, AV block, junctional tachycardia |
12. SPECIAL CONDITIONS / SYNDROMES
| Syndrome | Hallmark ECG Finding |
|---|---|
| Brugada syndrome | Type 1: coved STE ≥ 2 mm in V1–V2 with RBBB pattern; fever-induced |
| ARVC | Epsilon wave in V1–V3, T inversions in right precordial leads, LBBB-morphology VT |
| Long QT syndrome (LQTS) | QTc > 500 ms; Torsades de pointes |
| Short QT syndrome | QTc < 320 ms; peaky symmetric T waves; AF/VF risk |
| Brugada pattern type 2 & 3 | Saddle-back STE in V1–V2; diagnostic only with Na-channel blockers |
| HCM (hypertrophic cardiomyopathy) | LVH, deep narrow Q waves in I, aVL, V5–V6, T inversions |
| Acute pericarditis | Widespread saddle-shaped ST elevation + PR depression (especially II, aVF); reciprocal ST/PR changes in aVR |
| Pulmonary embolism (PE) | Sinus tachycardia (most common); S1Q3T3 pattern; RBBB; T inversions V1–V4; RAD |
| Cardiac tamponade | Low voltage + sinus tachycardia + electrical alternans |
| Prinzmetal angina | Transient STE with normal baseline ECG |
| Wellens syndrome | Biphasic or deeply inverted T waves in V2–V3 during pain-free interval → critical LAD stenosis |
| de Winter pattern | Upsloping STD + tall T waves V1–V6; no STE → LAD STEMI equivalent |
| LQTS type 1 | Broad-based T waves |
| LQTS type 2 | Notched/biphasic T waves |
| LQTS type 3 | Long isoelectric ST, late-peaking T wave |
13. PACEMAKER ECG FINDINGS
| Finding | Features |
|---|---|
| Ventricular pacing | Pacing spike → wide LBBB-morphology QRS |
| Atrial pacing | Pacing spike → normal QRS (if AV conduction intact) |
| Dual-chamber pacing | Two spikes: before P and before QRS |
| Failure to pace | No pacing spike when expected |
| Failure to capture | Pacing spike present but no QRS follows |
| Failure to sense | Pacing spike fires when it shouldn't (e.g., during intrinsic rhythm) |
| Pacemaker-mediated tachycardia (PMT) | Regular tachycardia at upper rate limit in dual-chamber pacemakers |
14. LOCALIZATION OF MI BY LEADS
| Territory | Leads with STE | Artery (usual) |
|---|---|---|
| Inferior | II, III, aVF | RCA (80%), LCx (20%) |
| Anterior | V1–V4 | LAD |
| Anteroseptal | V1–V3 | Septal branches of LAD |
| Anterolateral | V4–V6, I, aVL | LAD / LCx |
| Lateral (high) | I, aVL | LCx / Diagonal |
| Posterior | STD in V1–V3 (reciprocal) + tall R/T in V1 | LCx / RCA |
| Right ventricular | V1 + V4R | RCA (proximal) |
Quick Reference Summary
RATE → Normal 60–100 bpm
RHYTHM → Sinus? AF? Flutter? Block? VT?
AXIS → Normal / LAD / RAD / extreme
P WAVES → Present? Morphology? PR interval?
PR → 120–200 ms; short = WPW; long = heart block
QRS → Width (BBB); voltage (LVH/RVH); Q waves; delta/epsilon/J waves
ST SEGMENT → Elevation (STEMI/pericarditis/Brugada) or depression (ischemia/digoxin)?
T WAVES → Peaked (hyperK/hyperacute), inverted (ischemia/PE/Wellens), flat (ischemia/hypoK)
QT → Prolonged = Torsades risk; short = hyperCa/short QT syndrome
U WAVES → Prominent = hypokalemia
Sources: Tintinalli's Emergency Medicine, Braunwald's Heart Disease, Goldman-Cecil Medicine, StatPearls (NBK549803), GeekyMedics ECG Guide
This is a shared conversation. Sign in to Orris to start your own chat.